Myomectomy
Definition
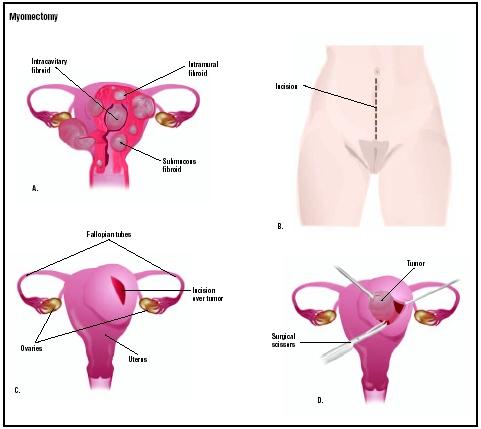
Myomectomy is the removal of fibroids (non-cancerous tumors) from the wall of the uterus. Myomectomy is the preferred treatment for symptomatic fibroids in women who want to keep their uterus. Larger fibroids must be removed with an abdominal incision, but small fibroids can be taken out by laparoscopy or hysteroscopy .
Purpose
A myomectomy can remove uterine fibroids that are causing such symptoms as abnormal bleeding or pain. It is an alternative to surgical removal of the whole uterus ( hysterectomy ). The procedure can relieve fibroid-induced menstrual symptoms that have not responded to medication. Myomectomy also may be an effective treatment for infertility caused by the presence of fibroids.
Demographics
Uterine fibroids are more common among African-American women than among women of other ethnicities.
Fibroids affect 20–40% of all women over the age of 35, and 50% of African-American women. A 2001 study by the National Institute of Environmental Health Sciences found that the incidence of fibroids among African-American women in their late 40s was as high as 80%, while approximately 70% of white women of that age were diagnosed as having fibroids. Women who are obese, are older, or started menstruating at an early age are also at an increased risk of developing uterine fibroids. Another study published in 2003 indicated that women with less education were more likely to have a hysterectomy performed to treat fibroids, instead of a less-invasive procedure such as myomectomy.
Description
Usually, fibroids are buried in the outer wall of the uterus, and abdominal surgery is required. If they are on the inner wall of the uterus, uterine fibroids can be removed using hysteroscopy. If they are on a stalk (pedunculated) on the outer surface of the uterus, laparoscopy can be performed.
Removing fibroids through abdominal surgery is a more difficult and slightly more risky operation than a hysterectomy. This is because the uterus bleeds from the sites where the fibroids were removed, and it may be difficult or impossible to stop the bleeding. This surgery is usually performed under general anesthesia, although some patients may be given a spinal or epidural anesthesia.
The incision may be horizontal (the "bikini" incision) or a vertical incision from the navel downward. After separating the muscle layers underneath the skin, the surgeon makes an opening in the abdominal wall. Next, the surgeon makes an incision over each fibroid, grasping and pulling out each growth.
Every opening in the uterine wall is then stitched with sutures. The uterus must be meticulously repaired in order to eliminate potential sites of bleeding or infection. The surgeon then sutures the abdominal wall and muscle layers above it with absorbable stitches, and closes the skin with clips or non-absorbable stitches.
When appropriate, a laparoscopic myomectomy may be performed. In this procedure, the surgeon removes fibroids with the help of a viewing tube (laparoscope) inserted into the pelvic cavity through an incision in the navel. The fibroids are removed through a tiny incision under the navel that is much smaller than the 4–5 in (10–13 cm) opening required for a standard myomectomy.
If the fibroids are small and located on the inner surface of the uterus, they can be removed with a thin, telescope-like device called a hysteroscope. The hysteroscope is inserted into the vagina through the cervix and into the uterus. This procedure does not require any abdominal incision, so hospitalization is shorter.
Diagnosis/Preparation
Surgeons often recommend hormone treatment with a drug called leuprolide (Lupron) two to six months before surgery in order to shrink the fibroids. This makes the fibroids easier to remove. In addition, Lupron stops menstruation, so women who are anemic have an opportunity to build up their blood count. While the drug treatment may reduce the risk of excess blood loss during surgery, there is a small risk that smaller fibroids might be missed during myomectomy, only to enlarge later after the surgery is completed.
Aftercare
Patients may need four to six weeks of recovery following a standard myomectomy before they can return to normal activities. Women who have had laparoscopic or hysteroscopic myomectomies, however, can usually recover completely within one to three weeks.
Risks
The risks of a myomectomy performed by a skilled surgeon are about the same as hysterectomy (one of the most common and safest surgeries). Removing multiple fibroids is more difficult and slightly more risky. Possible complications include:
- infection
- blood loss
- weakening of the uterine wall to the degree that future deliveries need to be performed via cesarean section
- adverse reactions to anesthesia
- internal scarring (and possible infertility)
- reappearance of new fibroids
There is a risk that removal of the fibroids may lead to such severe bleeding that the uterus itself will have to be removed. Because of the risk of blood loss during a myomectomy, patients may want to consider banking their own blood before surgery ( autologous blood donation ).
Normal results
Removal of uterine fibroids will usually improve any side effects that the patient may have been suffering from, including abnormal bleeding and pain. Under normal circumstances, a woman who has had a myomectomy will be able to become pregnant, although she may have to deliver via cesarean section if the uterine wall has been weakened.
Morbidity and mortality rates
Depending on the surgical approach, the rate of complications for myomectomy is about the same as those for hysterectomy (anywhere between 3% and 9%). The rate of fibroid reoccurrence is approximately 15%. Adhesions (bands of scar tissue between organs that can form after surgery or trauma) occur in 15–53% of women postoperatively.
Alternatives
Hysterectomy (partial or full removal of the uterus) is a common alternative to myomectomy. The most frequent reason for hysterectomy in the United States is to remove fibroid tumors, accounting for 30% of all hysterectomies. A subtotal (or partial) hysterectomy is the preferable procedure because it removes the least amount of tissue (i.e., the opening to the cervix is left in place).
Fibroid embolization is a relatively new, less-invasive procedure in which blood vessels that feed the fibroids are blocked, causing the growths to shrink. The blood vessels are accessed via a catheter inserted into the femoral artery (in the upper thigh) and injected with tiny particles that block the flow of blood. The fibroids subsequently decrease in size and the patient's symptoms improve.
Resources
books
Connolly, Anne Marie and William Droegemueller. "Leiomy omas" In Conn's Current Therapy 2003 . Philadelphia: Elsevier Science, 2003.
Ludmir, Jack and Phillip G. Stubblefield. "Surgical Procedures in Pregnancy: Myomectomy" (Chapter 19). In Obstetrics: Normal & Problem Pregnancies . Philadelphia: Churchill Livingstone, 2002.
organizations
American College of Obstetricians and Gynecologists. 409 12th St., SW, P.O. Box 96920, Washington, DC 20090-6920. http://www.acog.org .
Center for Uterine Fibroids, Brigham and Women's Hospital. 623 Thorn Building, 20 Shattuck Street, Boston, MA 02115. (800) 722-5520. http://www.fibroids.net .
other
de Candolle, G., and D. M. Walker. "Myomectomy." Practical Training and Research in Gynecologic Endoscopy. February 17, 2003 [cited March 13, 2003]. http://www.gfmer.ch/Books/Endoscopy_book/Ch14_Myomectomy.html .
"High Efficacy Rate Shown in Minimally Invasive Treatment of Uterine Fibroids." Doctor's Guide. January 13, 2003 [cited March 14, 2003]. http://www.pslgroup.com/dg/2271BA.htm .
Indman, Paul D. "Myomectomy: Removal of Uterine Fibroids." All About Myomectomy. 2002 [cited March 14, 2003]. http://www.myomectomy.net .
Toaff, Michael E. "Myomectomy." Alternatives to Hysterectomy Page [cited March 14, 2003]. http://www.netreach.net/~hysterectomyedu/myomecto.htm .
"Uterine Fibroids: Disproportionate Number of Black Women with More, Larger Tumors." National Institute of Environmental Sciences. March 2001 [cited March 14, 2003]. http://www.niehs.nih.gov/oc/crntnws/2001mar/fibroids.htm .
Carol A. Turkington
Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Myomectomies are usually performed in a hospital operating room or an outpatient setting by a gynecologist, a medical doctor who has specialized in the areas of women's general health, pregnancy, labor and childbirth, prenatal testing, and genetics.
QUESTIONS TO ASK THE DOCTOR
- Why is a myomectomy being recommended?
- How many myomectomies do you perform a year?
- What type of myomectomy will be performed?
- What are the risks if I decide against the myomectomy?
- What alternatives to myomectomy are available to me?
Thanks
leave info at pam7778@yahoo.com THANK YOU a thousand THANK YOUS!!!! There must be at least one real Doctor out there with both true skill, and morally ethical practices. HURRY!
Thank You
\
and tell me pls what can I do to reduce the chances of adhesions.
Thank in advance
i have done a scan and it results that i have a submucosal, a pendiculated and subserosal in the lower segment of the uterine.
the docter recomended a myomectomy can i do a laparascopic or abdominal sugery?
can the fallopian tubes with adhesions be unblocked when they are doing the sugery?
thankyou for the information you provide.
Thanks a lot
It's 2 weeks today and I'm feeling not too bad. I've got 2 weeks before I go back to work and I'm confident that I'm going to feel ok. My wounds are ok, although there is still some bruising around each of the incisions. They are starting to itch a little! I still have brownish/red discharge. The worst thing is the little shooting pains in my private bits, particularly when I change position in bed. At least I can now sleep on my sides - I found I had to sleep on my back for the first week or so.
If you're about to go through the same operation, I want to wish you the best of luck and to reassure you that it probably won't be as bad as you think, but be prepared to take things easy for a while and let yourself recover. Good luck!
I have an unstable pelvis and wear a special brace just under my hips to hold it together. I'm worried that the surgery would mean I can't get support for my pelvis for a long time as the brace is in line with bikini pants - not to mention the damage from cut muscles, the surgical man-handling, and the sustained position through surgery.
It's been a while since you posted, but if you check back, I'd love to hear from you. Thanks again for sharing, and hope you're doing great now.
I have also suffered with fibrodes for years, and took me a while to decide the best course for me. I consulted different doctors and tried also chinese medicine for removal of fibroids.
In the end, i was still with painful long periods and finally decided to do a myomectomy since i am 32 and still want to have children.
The surgery went well, i am 3 weeks after operation and it was not as bad as i thought. Spent 3 nights in hospital, on the first day with pains and under medication. Second day after operation, they removed the catheter and i was forced to go pee and walk a bit,weird at first.
I had 7 miomas removed, and i had one in the uterus. The incision was in the bikini line.
The best tips i can give to anyone who is going through that:
Stay calm (doctor gave a mild sleeping pill the night before procedure), it is a fairly common procedure and choose your doctor properly
Walk slowly from the second day of operation for about 10 minutes, it helps on recovery a lot. I did a few walks during the days in the clinic, and felt better.
Drink plenty of fluids
Bowl movement will only return after a week or so after operations, i think i was scared but ended up eating prunes to make the job easier lol
Rest a lot
Wear loose comfortable clothing and underwear that does not touch the bikini line, so as to not cause abrasion at the incision point and cover the lower abdomen (which is swollen after operation)
So far no complaints, no pain and not under medication.
I stopped all medication within a week after operation and feeling great, my period is back to normal, so amazing, i am so happy. Still have a week off work and walk for a few minutes everyday, increasing time at a normal pace each day.
Good luck :)
I am so confused. My kids are 15 and 25 years old and I do not want anymore. I have had fibroids for years and I have had the freezing done twice and my fibroids are back again. I have them inside of my uterus and my doctor told me that I needed a hysterectomy. I am scared because I have extremely high blood-pressure and the fibroids are growing as I speak. I wonder should I get a third opinion or just go ahead with the hysterectomy? I really do not want a hysterectomy. Any suggestions?
Which brings me to the myomectomy. My before gynecologist retired and ended with a new one. He was okay with doing a hysterectomy,but, told me about the myomectomy. I was still head over, I want a hysterectomy and wanted one for years. After some talk from my Besty and mom I decided to go with the lesser first just to avoid later regret.
So, December 31 I went in at about 12. I did get anxious the week leading up to the procedure. I had a second opinion earlier in the month because I wanted to get it done sooner. Do try to have a second opinion just to make sure everyone is on the same sheet of music. All the test align and both doctors are aligning in prognosis. Do your homework! The Internet has so mush information everything from forums to doctor and medical research. Read it. I was anxious the day of, I've never been in a hospital past a few hours! Make sure you have all affairs in order so you won't have to worry about things. That's the second key,PLANNING. Everything from who is walking the dog. If you live upstairs or have an upstairs home. Who is going to drive you around town,down to what you're packing for the hospital. I went in surgery came out and was admitted. There will be pain. I had the button administered meds,push and it sends the meds. Use it! You're paying for
it. The catheter was removed on day two. I was ready to get up and walk immediately. Pain is part of it but you need to get up and started trying to walk,going to the bathroom. You're not rushing your recovery you're helping it along. Use the spirometer that builds your breathing. Read all the paperwork the nurses give you before you go in the hospital. Start practicing the breathing techniques and how to hold a pillow against you to cough. I did need a blood transfusion mainly because I had my cycle the week before and there is quite a bit of bleeding in the surgery. They check to make sure you pass gas or have a bowel movement. I didn't start passing gas until day three but I had to use a laxative ( magnesium citrate) to help with the bowel movement. I already take stool softeners but I needed a little help. By the way, day one and two is liquid diet! Day three I came home and I actually had a LazBoy chair so it was easier to sleep in that, kicked back. You definitely have to sleep on your back for
Once again start helping your body recover by MOVING! At week two or so started trying to sleep a little on the side, just a little. Use a pillow lay the pillow beside u and turn just a little if it hurts don't do it a lots. Just work it everyday a little at a time. Walk around the house to the bathroom, the kitchen, like that. Don't pick up heavy things, nothing heavier than a gallon of milk maybe less at first.start with half gallon,lol. Don't bend over, use your legs. Bend your legs, not your body! Put things at arms length. Water,remotes,phone,ect. That's where the prior planning comes in, setting up the area where you will be most of the time. Do NOT DRIVE the first week or two. You don't want to kill anyone,the meds they give like Vicodin slip up on you. Be responsible! For the first week keep the meds steadily in your system to keep down pain. This will help you recover better, because you can do a little more if you're not in a lot of pain. Then gradually try to scale back as you will realize you can handle doing just a little bit more. Don't overdo it! GRADUALLY!
I'm on three weeks or so. I went back to school January 7th, the first night was hard, the meds were making me sleepy. The second night I took my meds slightly earlier and was better the
So recap,
Dr visit/ second opinion if u can
Study myomectomy in and out forums and medical articles including doctors who do the procedure
Plan
Go get it done
Recovery, don't baby sit it but don't overdo it
Anything ridiculously abnormal for more than a day don't go to a forum call or visit dr.
Note: i am only sharing my experience and what I did to make this process less stressful and back on my feet. I am not a doctor and each woman's body is different.
my gynecologist plans to myomectomy. what kind of incision and anesthesia is required?
doesn't it shrink by use of medication (luprun)?or should I use medication befor surgery?
how long does it take to recover?
can I exercise after surgery?how mwny weeks after it?
The type of incision depends on the size and location of the fibroids, and probably your physician's preference for removing them. I would have preferred a bikini cut, but my largest fibroid was about 9 cm, and she needed to do a vertical incision for the best access to my uterus. My incision extends from just below my navel to just below the bikini line.The bottom of the incision is still very sensitive, probably because it's an area that's always covered. I think I had general anesthesia. (Suggestion: bring a pillow with you to leave in the car going to surgery. You will need it to "cushion" your tummy on the ride home.)
First 2-3 days, you will feel pain, but it does get better. The prescription pain meds do help -- use them! I could only sleep sitting upright, as any stretching in the lower regions was too uncomfortable. After about 1.5 weeks, I was able to sleep in my bed, but only on my side. I'm still not able to sleep directly on my tummy. Constipation is common -- they had to open your abdomen to remove something, exposing your intestinal tract. It took me about a week for that to subside, using Colace (stool softener) and occasionally some Miralax.
I have to keep reminding myself that I did have a major surgery, so it's ok that I'm unable to do a lot. As I said, I'm now about 4 weeks post surgery, and I feel really good, except my energy level still hasn't fully returned. Loose clothing like dresses, skirts, and yoga pants are my wardrobe staples! I'm able to drive, and the only time I experience a little pain is while sleeping when I attempt to turn to my other side. I tried grocery shopping by myself yesterday, and though I didn't pick up anything heavy, I was exhausted after pushing the basket through the store. I asked for help pushing the basket to my car and unloading the groceries. I did have to come home and REST. I wanted to start going to the gym, but I know that I'm not ready for that. I can walk, and that's what I'll keep doing unless my body tells me otherwise. Best advice...do move around, but don't overdo it. Take it easy and don't try to rush your recovery. As Nina said in her previous post - every woman's body is different. You have to listen to YOUR body.
At about 6:35 pm I woke up, the first question I asked the nurse if the surgery was finished and how much fibroid was taken out. She said yes and they was one large one and two small ones the size of peas. I did not need any blood transfusion as I had minimal to no bleeding during the operation. I spend two days in the hospital was actually disappointed to leave because the nurses and my doctor really took good care of me. Anyway the first week and a half was most challenging getting out of bed was a task and having to sleep on my back was torture for me. I must say my recovery went quite well did not really have you use much pain killers. My doctor even told me the day after the surgery my uterus snapped back right into place after he removed the large fibroid which he was surprised by. I had a period exactly a month after my surgery and it was normal no heavy bleeding and no large blood cloths passed. I must say doing that surgery was the best decision I have made in a long time. After about three weeks I started to lose weight around my tummy area. I am due for my six week check up tomorrow to see if I am healing as expected on the inside, so I can resume work in a few days.
At first the thought of surgery was really daunting as I hate hospitals & had the fear of the unknown for the surgery. The fact my symptoms were persisting & I was tired of being sick, I made up my mind with some persuasion to do the operation.
I must say God is good all the time as I didn't need blood & my gnae told me that I didn't lose a lot of blood. I took the spinal anaesthetic so I heard most of what was going on except in the last part when I started feeling pain so I was given Morphine thru the IV.
It was a bikini cut & I really found it hard to turn & get up out of the hospital bed. At times I moved too fast forgetting I had done surgerym the nurses had to remind me to take my time + use the rails @ the bedside to assist me to get up.
After all of that I wanted to leave the hospital the next day, but was discharged 3 days post surgery.
Recovery for the 1st two weeks was awful as I felt excrutiating pain after the meds were done. Eating lots of fruits & veggies along with cranberry juices helped to get the body back on track. Walking for 20-30 mins each day helped to heal the body a whole lot & I lost couple lbs by eating less starches.
The cut which was a "bikini cut" was tender & below the navel was sore + scratched/itched a lot.
My advice to any1 about to do myo surgery is: a)seek a good gnae b)build ur blood count by taking iron tabs (don't forget to take vitamin c in the form of citrus fruits) so the body can absorb the iron c)After surgery roll on ur side, use a chair or the bed rail to u in getting out of bed d)eat lots of fruits of veggies 2)eliminate processed foods 6)do lots of walking.
After 10 weeks u may feel near to normal again like me or for other persons, after 6 weeks they feel fine. Every1 has a different body, but our bodies will respond postively if we treat it right.
I had my Myomectomy in 1992 after my doctor suspected an eptopic pregnancy, which turned out that I didn't, but on doing the
operation a very large fibroid was removed. During the operation I lost a great deal of blood and had to have a blood transfusion. I ended up with a large rectus sheath haematoma which completely filled my lower abdomen and I was in agony for months with it. Because of the low blood pressure at that time I had a transient ischdemic attack which is like a mini stroke and this affected my left side. I complained of pain in the left iliac fossa, where the incision was made, many times and found I kept losing my balance and was not co-ordinating very well. In 1993 I had to have a full hysterectomy, the uterus, ovaries and fallopian tubes were all removed. My gynaecologist told me it was a very difficult operation as he had to also make several repairs from the Myomectomy. I had a twisted appendix, a closed loop bowel, numerous adhesions, and hernias. I was put on HRT and Beta blockers as I my blood pressure was high and I was diagnosed with hemiplegic migraine which gives the pain in the head but also left sided weakness. Over the last twenty years I have had several attacks and also have them after anaesthetic and my blood pressure is always very high. I don't have the confidence to go out on my own anymore in case I have an attack, so these complications have caused a lot of problems for me over the years.
I would be interested to hear if anyone else has had similar complications. The advice I would give anyone due to have a Myomectomy or Hysterectomy is to make sure the surgeon has a good reputation and had successful results. I would not wish
anyone to experience the problems I have had and still do. Good luck to you all.
I have been washing with antibacterial soap, using ice during the day and heat at night. Because I was not bleeding I was allowed Motrin for pain. I strongly advise taking a stool softener...trust me!
Today I am 72 hrs post op- and I have been sneezing (seasonal allergies) and I had a bowel movement...I am now bleeding and start to pass clots. I'm clearly upset but the sane part of me is trying to gauge the flow. If anyone has advice I would greatly appreciate it- I'm laying here with tears just pouring down my cheeks. Any advice would be greatly appreciated.
I have just undergone the same surgery (11th Sept) and thankfully am on the way to recovery. I had the epidural anesthesia as recommended by the team and was unable to more for some time (8hrs) so a catheter was fitted and i had no issues with peeing the following day. Passing stool was another matter but i was put on a liquid, then soft food only diet and am now on solids -though avoiding consuming eating much starchy products - sticking to fruit, vegetables and a little chicken. Which i think would help and avoid the need for stool softener and avoid bloating. I was quite swollen after surgery.
I started menstruation 2 days after the surgery and informed the doctor, who explained this was quite normal and that my menstrual cycle will likely be disrupted for several months. So it could be the bleeding you experienced afterwards was a result of that - but of course doctor's advice should be sought. Clots would be normal also but that depends greatly on the size experienced.
I did not have much information on the procedure before surgery, excepting what i read on the internet, as i am in thailand and the doctor's english was limited, patient reassurance does not really come into play here! but these articles helped prepare me in the 3 days between diagnosis and surgery that i had.
I had the standard cut (as illustrated by B above) and apparently this is quicker to heal as it does not cut across the muscles but rather between them. So the post op pain i have felt has been minimal and i was able to get up and walk the following day, and 2 days later was almost walking upright - though slowly. Now a week later I have had the skin clips removed and I am able to walk properly... i made 3km yesterday and plan to walk about the same distance each day to build upon my strength. I am able to lie on my side using a pillow for support and no need for pain killers after the 1st week post-op
Unfortunately due to the anaesthetic I was unable to roll onto my side which left me quite sore in the bottom and I am still slightly numb in the glute muscles - again the doctor has reassured me this will fade and If not i should revisit in 6 weeks. Unfortunately for me I must go on a long haul flight but I'm healing well and able to walk about very easily. Does anyone have any advice for getting comfortable on a plane (12hour flight!)?
best wishes to all who need a myectomy and to those who are in recovery.
I had my 2nd myo on 11/19/13, the 1st in 2007 and had the same symptoms after surgery. It's normal as a side affect from the anesthesia. Just rest and take walks around the house so you do not end up with blood clots. After about 2 weeks you won't remember the pain and will feel better.
Helen don't give up, my doctor told me to wait at least a yr. before even trying. She definitely stated that I will need infertility treatments and a C-section. I would just focus on your body healing right now and maybe later searching for a more compassionate doctor.
I have terrible periods and i have 2 ultrasounds tomorrow to see whats going on.im nervous so keep me in prayer guys and good luck and blessings to you all!!!
what should I expect from this type of surgery.
I was first diagnosed with fibroids in 2009 after going to get checked for a longer than usual period which occurred two times in one month. The ultrasound revealed a cluster of fibroids measuring just over 3cm. I was put on birth controls for a year and we monitored the fibroid annually. In 2012 I discovered through one of my yearly ultrasounds that my fibroid had doubled in size to just over 6cm, at this time the doctors decided to monitor the growth through ultrasounds every 6 mth. My family doctor felt it was time to do something but the specialist disagreed because the fibroids caused no major symptoms, I didn't have any children and I am young. Six mth later it grew to just over 7cm again my family doctor sent me to the specialist thinking it was time to act. The specialist was not alarmed by the result and simply insisted that I just get pregnant. She even went as far as telling she didn't recommend surgery because she couldn't guarantee not taking out my uterus. I felt like I was stuck between a rock and a hard place as I was just getting to know my boyfriend and we were not ready to have children but yet the fibroid grew. On Jan 2, 2014 I did another ultrasound which revealed a now 8.5cm fibroid. I decided to see a different specialist and was referred to one on the 28th. He recommended surgery and said he would never advise me to get pregnant with such a large fibroid. My myomectomy (bikini cut) is scheduled for this Friday Feb 7th at noon and I am terrified. I'm only 29 and really want to have children. I've only taken 3 weeks off work (I work in an office) Is 3 weeks enough? Please keep me in your prayers...I will post again after surgery if all goes well.
I've read that lupron can make it hard to detect smaller fibroids, so they may be missed. Is this more of a risk for laparascopic surgery? If the surgery is open, my understanding is that the surgeon can feel for even very small fibroids, so is missing them due to lupron still a risk with open myomectomy? Has anyone here done treatment with lupron prior to open myomectomy? How were your outcomes?
. I ended up having a laparoscopic hysterectomy in 2008. Life is much better now.
Not sure if I should fuss about the pain after urination?
Is there anyone experiencing this? Please help
I
Is anyone experienced this complication?
If yes, how much time takes to get feeling back?
But I discovered that after my period am having yellow discharge it was flowing lightly
But now it's flowing much what do I do, is it normal .
I had a myomectomy. It was performed by my GYN. I was put under before I went to the OR because my doctor knew how scared I was. I don't remember the recovery room. I remember the hospital room, and my son being there. I have four tiny insitions, you can barely see them. My uterus was also removed I was told it was very large 17cm my doctor even took a picture of it to show me, but I still have my overies to keep my hormone leves intact. I was given pain medications in the hospital. I stayed for two days. My doctor said it was so I could rest. I had a cathader in place it must have been done while I was under. I had lots of pain for the first week. I am now on my second week and I am not experiencing any pain so I don't have to take pain meds. I am also a diabetic so they thought that my healing and recovery would take longer but so far I am healing faster than they thought. My diabetes has been uncontrolled for a while. I am so thankful to God for providing me with amazing doctors that truely care about my well-being. Dr . Seethapan is an amazing GYN and surgeon. All my doctors are through Med Star in Olney, Maryland. I am feeling so blessed that I am not in in pain, and Today is Sunday June 11, 2017. I had my surgery May 31,2017,and this Wednesday the 14th will make two weeks and I haven't had any complications except constipation, but I was told to expect that and to walk a couple of feet each day to build myself up.
Background & timeline: I am 34 years young, very active and on a balanced diet, no kids. I noticed something is off with my body 1,5 years ago, went for a check up but the nurse refused to send me to a specialist, I have immigrated to his country some years ago and felt hopeless... So, 6 months after that nurse refused to send me to a specialist I went to my home country, did an ultrasound, MRI and saw and gynecologist who said I have two fibroids. Fibroids were 10 cm and 4 cm in diameter then... came back to Canada and managed to get a referral for an ultrasound (again, for a confirmation) by a doctor from a walk-in clinic (bless his soul). The doctor referred me to an amazing gynecologist (bless her soul too) and prescribed iron to bring up the iron level. From the time of ultrasound to my surgery it took less than 8 months. I was referred for monthly iron-level check ups and an MRI before the surgery. I researched a lot about how to treat fibroids and myomectamy was what I went to ask for from my gynecologist. She also prescribed me FIBRISTAL - amazing non-hormonal drug that completely eliminated all symptoms of fibroids along with the periods for three months.
Day of surgery: I was in high spirits, sending selfies of my gown to my friends :) doctors told me I was the healthiest patient they ever had to operate on. Surgery lasted about two hours from 8 am, I had a small horizontal incision around my bikini line and general anesthesia. Post-op recovery room seemed EXTREMELY LOUD when I woke up, no pain, I was very thirsty though and with a catheter. My friend was next to me and seeing her lovely face definitely brought peace. I was in and out of sleep for the next 24 hours, no pain. Tried drinking apple juice in the evening and almost puked. Advice: stick with water day 1.
Day 3: I had a good sleep, still on painkillers, no pain unless I moved awkwardly. More smoothies and granola for breakfast/lunch, took awhile for my doctor to come see me that day and discharge me. My friend picked me up from the hospital and I stayed with her for three days through Christmas.
Day 7: I was feeling good, just relieved from a constipation, eating normally, nothing heavy and still on some painkillers, just low on energy. Came home, made dinner and feeling good.
It's Day 10 today: I really have problems sleeping through the night - nothing to do with pain, just insomnia. No pain, I do my chores at home, groceries are being delivered. I feel like I am on a great path to recovery! No discharges, some bruising around my belly button and incision.
To all of you being anxious about the surgery: 1. Read posts above by Dalila, Erica, Tracy and Nina above - stay positive. 2. I really hope you have a good gynecologist you could read up on, and they have great references, experience and are a nice person. 3. Try to have a balanced diet with as little of processed foods as possible and be active. 4. Have someone you trust to support you through the process, someone to remind you to take good care of yourself and look after you particularly the first few days after the surgery.
Wishing you best of luck and good health!
All my blessings, Mae.
I had them after my myomectomy, very painful. I have been searching all the forums to see if anyone else had this complication but have not been successfully. Can anyone share their experience please . Thanks
I finally had a Myomectomy 11days ago.i was blessed to have a understanding Gyna and the hospital staff were all very nice to me
My mum was very nervous so I had to keep a brave front for her, I remember dancing into the theater to the delight of the nurse who commented she had not seen a patient like me
I was given a spinal anesthesia at first , so I was chatting with my surgeon during the procedure, an hour later I was given a GA when I complained of a headache.
First thing I remember when I woke up was I could not breath, my chest was constricted and it felt like a bag of sand was in my chest, I remember thrashing around and the nurses and my mum had to hold me down, I threw up some thick mucus and immediately felt better I was so thirsty but wasn't allowed to drink water, I kept Drifting in and out of sleep, the sleeping injection they gave me didn't knock me out long enough.
Day 1: catheter was taken out and I was allowed to take liquids, water felt bland I could only manage juice
Day 2: I had a bloody headache, doctor said it's a result of the anesthesia, peeing was painful
Day 3: hurray, I stooled for the first time, it was uncomfortable and painful but I was happy cos I was told it will take a week, I was discharged on day 3.
For the past few days ive been taking it as easy I can, bad case of insomnia as I am not used to sleeping on my back and sleeping on my side is painful. Headache creeps up on me but not as bad as the first few days.
Been passing out gas a lot.. Heheheh
I have light vaginal bleeding so I wear a panty liner it has reduced now
I feel pain on both sides of my stomach and a numbness just above the incision.. Doctor says it's normal
Can't stand for too long, serious pressure around my waist when I do.
Road to recovery is slow but promising
Hope this helps anyone out there