Laparoscopy
Definition
Laparoscopy is a minimally invasive procedure used as a diagnostic tool and surgical procedure that is performed to examine the abdominal and pelvic organs, or the thorax, head, or neck. Tissue samples can also be collected for biopsy using laparoscopy and malignancies treated when it is combined with other therapies. Laparoscopy can also be used for some cardiac and vascular procedures.
Purpose
Laparoscopy is performed to examine the abdominal and pelvic organs to diagnose certain conditions and—depending on the condition—can be used to perform surgery. Laparoscopy is commonly used in gynecology to examine the outside of the uterus, the fallopian tubes, and the ovaries—particularly in pelvic pain cases
where the underlying cause cannot be determined using diagnostic imaging (ultrasound and computed tomography). Examples of gynecologic conditions diagnosed using laparoscopy include endometriosis, ectopic pregnancy, ovarian cysts, pelvic inflammatory disease [PID], infertility, and cancer. Laparoscopy is used in general surgery to examine the abdominal organs, including the gallbladder, bile ducts, the liver, the appendix, and the intestines.
During the laparoscopic surgical procedure, certain conditions can be treated using instruments and devices specifically designed for laparoscopy. Medical devices that can be used in conjunction with laparoscopy include surgical lasers and electrosurgical units. Laparoscopic surgery is now preferred over open surgery for several types of procedures because of its minimally invasive nature and its association with fewer complications.
Microlaparoscopy can be performed in the physician's office using smaller laparoscopes. Common clinical applications in gynecology include pain mapping (for endometriosis), sterilization, and fertility procedures. Common applications in general surgery include evaluation of chronic and acute abdominal pain (as in appendicitis), basic trauma evaluation, biopsies, and evaluation of abdominal masses.
Laparoscopy is commonly used by gynecologists, urologists, and general surgeons for abdominal and pelvic applications. Laparoscopy is also being used by orthopedic surgeons for spinal applications and by cardiac surgeons for minimally invasive heart surgery . As of 2003, procedures under investigation for possible laparoscopy included thyroidectomy and parathyroidectomy .
Demographics
At first, laparoscopy was only been performed on young, healthy adults, but the use of this technique has greatly expanded. Populations on whom laparoscopies are now performed include infants, children, the elderly, the obese, and those with chronic disease states, such as cancer. The applications of this type of surgery have grown considerably over the years to include a variety of patient populations, and will continue to do so with the refinement of laparascopic techniques.
Description
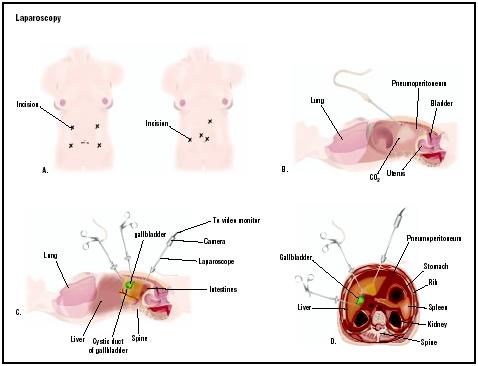
Laparoscopy is typically performed in the hospital under general anesthesia, although some laparoscopic procedures can be performed using local anesthetic agents. Once under anesthesia, a urinary catheter is inserted into the patient's bladder for urine collection. To begin the procedure, a small incision is made just below the navel and a cannula or trocar is inserted into the incision to accommodate the insertion of the laparoscope. Other incisions may be made in the abdomen to allow the insertion of additional laparoscopic instrumentation. A laparoscopic insufflation device is used to inflate the abdomen with carbon dioxide gas to create a space in which the laparoscopic surgeon can maneuver the instruments. After the laparoscopic diagnosis and treatment are completed, the laparoscope, cannula, and other instrumentation are removed, and the incision is sutured and bandaged.
Laparoscopes have integral cameras for transmitting images during the procedure, and are available in various sizes depending upon the type of procedure performed. The images from the laparoscope are transmitted to a viewing monitor that the surgeon uses to visualize the internal anatomy and guide any surgical procedure. Video and photographic equipment are also used to document the surgery, and may be used postoperatively to explain the results of the procedure to the patient.
Robotic systems are available to assist with laparoscopy. A robotic arm, attached to the operating table may be used to hold and position the laparoscope. This serves to reduce unintentional camera movement that is common when a surgical assistant holds the laparoscope. The surgeon controls the robotic arm movement by foot pedal with voice-activated command, or with a handheld control panel.
Microlaparoscopy has become more common over the past few years. The procedure involves the use of smaller laparoscopes (that is, 2 mm compared to 5–10 mm for hospital laparoscopy), with the patient undergoing local anesthesia with conscious sedation (during which the patient remains awake but very relaxed) in a physician's office. Video and photographic equipment, previously explained, may be used.
Laparoscopy has been explored in combination with other therapies for the treatment of certain types of malignancies, including pelvic and aortic lymph node dissection, ovarian cancer, and early cervical cancer. Laparoscopic radiofrequency ablation is a technique whereby laproscopy assists in the delivery of radiofrequency probes that distribute pulses to a tumor site. The pulses generate heat in malignant tumor cells and destroys them.
The introduction of items such as temperature-controlled instruments, surgical instruments with greater rotation and articulation, improved imaging systems, and multiple robotic devices will expand the utility of laparoscopic techniques in the future. The skills of surgeons will be enhanced as well with further development of training simulators and computer technology.
Diagnosis/Preparation
Before undergoing laparoscopic surgery, the patient should be prepared by the doctor for the procedure both psychologically and physically. It is very important that the patient receive realistic counseling before surgery and prior to giving informed consent . This includes discussion about further open abdominal surgery (laparotomy) that may be required during laparoscopic surgery, information about potential complications during surgery, and the possible need for blood transfusions. In the case of diagnostic laparoscopy for chronic pelvic pain, the procedure may simply indicate that all organs are normal and the patient should be prepared for this possibility. The surgery may be explained using pictures, models, videotapes, and movies. It is especially important for the patient to be able to ask questions and express concerns. It may be helpful, for the patient to have a family member or friend present during discussions with the doctor. Such conversations could understandably cause anxiety, and information relayed may not be adequately recalled under such circumstances.
There is usually a presurgical exam two weeks before the surgery to gather a medical history and obtain blood and urine samples for laboratory testing. It is important that the patient inform the doctor completely about any prior surgeries, medical conditions, or medications taken on a regular basis, including such nonsteroidal anti-inflammatory drugs (NSAIDs) as aspirin . Patients taking blood thinners like Coumadin or Heparin (generic name: warfarin) should not adjust their medication themselves, but should speak with their prescribing doctors regarding
their upcoming surgery. (Patients should never adjust dosage without their doctors' approval. This is especially important for elderly patients, asthmatics, those with hypertension, or those who are on ACE inhibitors.) If a tubal dye study is planned during the procedure, the patient may also be required to provide information on menstrual history. For some procedures, an autologous (self) blood donation may be suggested prior to the surgery to replace blood that may be lost during the procedure. Chest x rays may also be required. For some obese patients, weight loss may be necessary prior to surgery.
Immediately before to surgery, there are several preoperative steps that the patient may be advised to take. The patient should shower at least 24 hours prior to the surgery, and gently but thoroughly cleanse the umbilicus (belly button) with antibacterial soap and water using a cotton-tipped swab. Because laparoscopy requires general anesthesia in most cases, the patient may be asked to eat lightly 24 hours prior to surgery and fast at least 12 hours prior to surgery. Bowel cleansing with a laxative may also required, allowing the it to be more easily visualized and to prevent complications in the unlikely event of bowel injury. Those who are have diabetes or have hypoglycemia may wish to schedule their procedures early in the morning to avoid low blood sugar reactions. The patient should follow the directions of the hospital staff, arriving early on the day of surgery to sign paperwork and to be screened by the anesthesiology staff. Questions will be asked regarding current medications and dosages, allergies to medication, previous experiences with anesthesia (that is, allergic reactions, and previous experiences regarding time-to-consciousness), and a variety of other questions. It is often helpful for the patient to make a list of this information beforehand so that the information can be easily retrieved when requested by the hospital staff.
Aftercare
Following laparoscopy, patients are required to remain in a recovery area until the immediate effects of anesthesia subside and until normal voiding is accomplished (especially if a urinary catheter was used during the surgery). Vital signs are monitored to ensure that there are no reactions to anesthesia or internal injuries present. There may be some nausea and/or vomiting, which may be reduced by the use of the propofol anesthetic for healthy patients undergoing elective procedures such as tubal ligation , diagnostic laparoscopy, or hernia repair. Laparoscopy is usually an outpatient procedure and patients are discharged from the recovery area within a few hours after the procedure. For elderly patients and those with other medical conditions, recovery may be slower. Patients with more serious medical conditions, or patients undergoing emergency laparoscopy, an overnight hospital stay or a stay of several days may be required.
Discharged patients will receive instructions regarding activity level, medications, postoperative dietary modifications, and possible side effects of the procedure. It may be helpful to have a friend or family member present when these instructions are given, as the aftereffects of anesthesia may cause some temporary confusion. Postoperative instructions may include information on when one might resume normal activities such as bathing, housework, and driving. Depending on the nature of the laparoscopic procedure and the patient's medical condition, daily activity may be restricted for a few days and strenuous during administration of anesthesia may cause some soreness. Additionally, shoulder pain may persist as long as 36 hours after surgery. Pain-relieving medications and antibiotics may be prescribed for several days postoperatively.
Patients will be instructed to watch for signs of a urinary tract infection (UTI) or unusual pain; either may indicate organ injury. It is important to understand the difference between normal discomfort and pain, because pain may indicate a problem. Patients may also experience an elevated temperature, and occasionally "postlaparoscopy syndrome"; this condition is similar in appearance to peritonitis (marked by abdominal pain, constipation, vomiting, and fever) that disappears shortly after surgery without antibiotics. However, any postoperative symptoms that cause concern for the patient should be discussed with the doctor, so that any fears can be alleviated and recovery can be accomplished. Due to the after-effects of anesthesia, patients should not drive themselves home.
It is advisable for someone to stay with the patient for a few hours following the procedure, in case complications arise. Injury to an organ might not be readily apparent for several days after the procedure. The physical signs that should be watched for and reported immediately include:
- fever and chills
- abdominal distension
- vomiting
- difficulty urinating
- sharp and unusual pain in the abdomen or bowel
- redness at the incision site, which indicate infection
- discharge from any places where tubes were inserted or incisions were made
Additional complications may include a urinary tract infection (resulting from catheterization) and minor infection of the incision site. An injury to the ureter may be indicated by abdominal distention or a pain in the flank. Additional testing may be required if a complication is suspected.
Risks
Complications may be associated with the laparoscopy procedure in general, or may be specific to the type of operation that is performed. Patients should consult with their doctors regarding the types of risks that are specific for their procedures. The most serious complication that can occur during laparoscopy is laceration of a major abdominal blood vessel resulting from improper positioning, inadequate insufflation (inflation) of the abdomen, abnormal pelvic anatomy, and too much force exerted during scope insertion. Thin patients with well-developed abdominal muscles are at higher risk, since the aorta may only be an inch or so below the skin. Obese patients are also at higher risk because more forceful and deeper needle and scope penetration is required. During laparoscopy, there is also a risk of bleeding from blood vessels, and adhesions may require repair by open surgery if bleeding cannot be stopped using laparoscopic instrumentation. In laparoscopic procedures that use electrosurgical devices, burns to the incision site are possible due to passage of electrical current through the laparoscope caused by a fault or malfunction in the equipment.
Complications related to insufflation of the abdominal cavity include gas inadvertently entering a blood vessel and causing an embolism, pneumothorax, or subcutaneous emphysema. One common but not serious side effect of insufflation is pain in the shoulder and upper chest area for a day or two following the procedure.
Any abdominal surgery, including laparoscopy, carries the risk of unintentional organ injury (punctures and perforations). For example, the bowel, bladder, ureters, or fallopian tubes may be injured during the laparoscopic procedure. Many times these injuries are unavoidable due to the patient's anatomy or medical condition. Patients at higher risk for bowel injury include those with chronic bowel disease, PID, a history of pervious abdominal surgery, or severe endometriosis. Some types of laparoscopic procedures have a higher risk of organ injury. For instance, during laparoscopic removal of endometriosis adhesions or ovaries, the ureters may be injured due to their proximity to each other.
Several clinical studies have shown that the complication rate during laparoscopy is associated with inadequate surgeon experience. Surgeons who are more experienced in laparoscopic procedures have fewer complications than those performing their first 100 cases.
Normal results
In diagnostic laparoscopy, the surgeon will be able to see signs of a disease or condition (for example, endometriosis adhesions; ovarian cysts; diseased gallbladder)immediately, and can either treat the condition surgically or proceed with appropriate medical management. In diagnostic laparoscopy, biopsies may be taken of tissue in questionable areas, and laboratory results will govern medical treatment. In therapeutic laparoscopy, the surgeon performs a procedure that rectifies a known medical problem, such as hernia repair or appendix removal. Because laparoscopy is minimally invasive compared to open surgery, patients may experience less trauma and postoperative discomfort, have fewer procedural complications, have a shorter hospital stay, and return more quickly to daily activities. The results will vary, however, depending on the patients's condition and type of treatment.
Morbidity and mortality rates
Laparoscopic surgery, like most surgeries, is not without risk. Risks should be thoroughly explained to the patient. Complications from laparoscopic surgeries arise in 1–5% of the cases, with a mortality of about 0.05%. Complications may arise from the laparoscopic entry during procedure, and the risks vary depending on the elements specific to a particular procedure. For example, the risk of injury to the common bile duct in laparoscopic biliary surgery is 0.3–0.6% of cases. The factors that contribute to morbidity are currently under study and debate. Injury may occur to blood vessels and internal organs. Some studies examining malpractice data indicate that trocar injury to the bowel or blood vessels may account up to one-fourth of laparoscopic medical claims. It has been suggested that these injuries can be reduced by alterations in the placement and use of the Verses needle, or by using an open technique of trocar insertion in which a blunt cannula (non-bladed) is inserted into the abdominal cavity through an incision. The insertion of secondary trocars may be of particular interest as a risk factor. There is still some debate, however, as to which method of trocar insertion is most appropriate in a particular situation, as no technique is without risk. The most commonly cited injury in laparoscopic malpractice claims has been injury to the bile duct (66%). Proper identification of this structure by an experienced surgeon, or by a cholangiogram, may reduce this type of injury. Other areas of the body may be injured during access including the stomach, bladder, and liver. Hemorrhages may also occur during the operation.
Laparoscopic entry injuries have been the subject of recent study. Data collected from insurance companies and medical device regulation indicate that bowel and vascular injuries may account for 76% of the injuries that occur when a primary port is created. Delayed recognition of bowel injuries was noted to be an important factor in mortality. The risk of possible injury or death in laparoscopy depends on such factors as the anatomy of the patient, the force of entry, and the type operative procedure being performed.
Alternatives
The alternatives to laparoscopy vary, depending on the medical condition being treated. Laparotomy (open abdominal surgery with larger incision) may be pursued when further visualization is needed to treat the condition, such as in the case of pain of severe endometriosis with deeper lesions. For those female patients with pelvic masses, transvaginal sonography may be a helpful technique in obtaining information about whether such masses are malignant, assisting in the choice between laparoscopy or laparotomy.
Resources
books
Merrell, Ronald C., ed. Laparoscopic Surgery. New York: Springer-Verlag New York, Inc., 1999.
Pasic, Resad P., Ronald L. Levine. A Practical Manual of Laparoscopy: A Clinical Cookbook. New York: The Parthenon Publishing Group, 2002.
Schier, Felix. Laparoscopy in Children. Berlin: Springer, 2003.
Soderstrom, Richard M., ed. Operative Laparoscopy, 2nd ed. Philadelphia: Lippincott-Raven, 1998.
Webb, Maurice, ed. J. Mayo Clinic Manual of Pelvic Surgery, 2nd ed. Philadelphia, 2000.
Zucker, Karl A., ed. Surgical Laparoscopy, 2nd ed. Philadelphia, 2001.
periodicals
Abu-Rustum, Nadeem R. "Laparoscopy 2003: Oncologic Perspective." Clinical Obstetrics and Gynecology 46, no.1 (March 2003): 61-69.
Bieber, Eric. "Laparoscopy: Past, Present, and Future." Clinical Obstetrics and Gynecology 46, no.1 (March 2003): 3–14.
Boike, Guy M., and Brian Dobbins. "New Equipment for Operative Laparoscopy." Contemporary OB/GYN, no. 2 (April 1998). http://consumer.pdr.net/consumer/psrecord.htm .
Chandler, J.G., S.L. Corson, L.W. Way. "Three Spectra of Laparoscopic Entry Access Injuries." Journal of American College of Surgeons 192, no.4 (April 2001):478–490.
organizations
American College of Obstetricians and Gynecologists. 409 12th Street SW, P.O. Box 96920, Washington, DC 20090-6920. http://www.acog.org .
Society of American Gastrointestinal Endoscopic Surgeons (SAGES). 2716 Ocean Park Boulevard, Suite 3000, Santa Monica, CA 90405. (310) 314-2404. http://www.endoscopy-sages.com .
Society of Laparoendoscopic Surgeons. 7330 SW 62nd Place, Suite 410, Miami, FL 33143-4825. (305) 665-9959. http://www.sls.org .
other
Agency for Healthcare Research and Quality. http://www.webmm.ahrq.gov/cases.aspx?ic=3 .
"Diagnostic Laparoscopy." Society of Gastrointestinal Endoscopic Surgeons. http://www.sages.org/pi_diaglap.html .
"Laparoscopy." WebMD.com . October 24, 2002). http://my.webmd.com/content/healthwise/21/5199.htm?lastselectedguid={5FE84E90-BC77-4056-A91C-9531713CA348 .
Jennifer E. Sisk, M.A.
Jill Granger, M.S.
QUESTIONS TO ASK THE DOCTOR
- Will this surgery be covered by my insurance? Will any postsurgical care that I require also be covered?
- What do I need to do to prepare for the surgery? Are there any restrictions on diet, fluid intake, or other measures?
- Are there any medications that should be stopped prior to the surgery?
- Does my medical history pose any potential problems that need to be considered before undergoing this procedure?
- What is your (the doctor's) training in performing this surgery? Will you perform the actual surgery or will a trainee?
- What aftereffects can I expect?
- Are there any post-surgical symptoms that might indicate a complication that I should report, and to whom should these questions be directed? What post-surgical symptoms should be considered "normal" and how might discomfort be relieved?
- What is the expected recovery period from this procedure?
- What special care or self-care is required following this surgery?
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Laparoscopy may be performed by a gynecologist, general surgeon, gastroenterologist, or other physician—depending upon the patient's condition. An anesthesiologist is required during the procedure to administer general and/or local anesthesia and to perform patient monitoring. Nurses and surgical technicians/assistants are needed during the procedure to assist with scope positioning, video system adjustments and image recording, and laparoscopic instrumentation.
Have had 1 prior bowel obstuction surgery, And 2 other abdomen surgery.
Thank you very much and more power.
Yours truly.
Larane
1. HAD A CT CHEST W/O CONTRAST AND THE EXAM CAME OUT AS STABLE FROM THE 4 YRS AGO FINDINGS BUT THE ONE CT CHEST THERE IMPRESSION WAS OLD GRANULOMATOUS DIEASE.
2. HAD A CT SCAN OF ABDOMEN W/O CONTRAST AND THE EXAM FOUND A 4MM NON CALCIFIED JUXTAPLEURAL NODULE IN THE RIGHT MIDDLE LOBE, POST CHOLECYSTECTOMY,ATHEROSCIEROSIS
3. HAD A PELVIS TRANSVAINAL AND THE EXAM FOUNG NO EVIDENCE OF RIGHT ADNEXAL MASS OR FREE FLUID AND NON VISUALIZATION OF MY LEFT OVARY WHICH THE RIGHT ONE WAS REMOVED IN 1982
MY STOMICH IS STILL IN PAIN AFTER MY SURGERY OF LAPASCOPY FOR THE ADHESIONS REMOVED AND I DONT KNOW WHICH DR. TO GO TO NEXT. I HAVE A DR FOR MY LUNGS,OBGYN,GALLBLADDER AND ONE FOR THE CLONOSCOPY I HAD 4 YEARS AGO, I DONT HAVE MUCH MONEY TO CALL ALL THESE DR.S FOR APPTS IF I DONT NEED TO, IVE BEEN TO MY GENERAL DR. 3 TIMES NOW FOR THIS AND I WANT SOME CLEAR RESULTS ON WHAT I HAVE.,MY DR. GIVES ME A CAT THEN I GO BACK TO MY GYN, NO OTHER DR.S HAVE BEEN REQUIRED FOR ME TO SEE..WHAT SHOULD I DO NEXT? I HAVE LIKE 6 DRS AND THEY ALL DO DIFFERENT OPERATIONS, I SURE DONT WANT TO GO THROUGH ALL THESE 6 DRS AGAIN, SO SOMEONE PLEASE HELP ME....
Thank You.
It is very good explaination regarding the procedures and the risks of the different laparascopy.
Thank you very much for this information.
Is open sergery better for umbilical hernia when adhesions are present from traumatic accident and old caesarian operation?
I should be obliged if you could give an information or advice about open sergery.
Thank you again It is a great help.
N Abbott.
Penny
What are the chances for me to have a baby
I am a 64.6 yr.old male and would like to know if this procedure is used for a condition of Diverticulitis?.What would you say is the best method to choose. I'm not at the critical stage but exploring my options. I appreciate your information. I will have it done if elected in Boston, Massachusetts.
So do they remove the scar tissue when they cut it away? Or do they leave it in there?
I had no major pain and the incision seems to be healing well. I am just a bit worried especially regarding the numbness.
Appreciate your help.
Thank you