Hysterectomy
Definition
Hysterectomy is the surgical removal of all or part of the uterus. In a total hysterectomy, the uterus and cervix are removed. In some cases, the fallopian tubes and ovaries are removed along with the uterus, which is a hysterectomy with bilateral salpingo-oophorectomy . In a subtotal hysterectomy, only the uterus is removed. In a radical hysterectomy, the uterus, cervix, ovaries, oviducts, lymph nodes, and lymph channels are removed. The type of hysterectomy performed depends on the reason for the procedure. In all cases, menstruation permanently stops and a woman loses the ability to bear children.
Purpose
The most frequent reason for hysterectomy in American women is to remove fibroid tumors, accounting for 30% of these surgeries. Fibroid tumors are non-cancerous (benign) growths in the uterus that can cause pelvic, low back pain, and heavy or lengthy menstrual periods. They occur in 30–40% of women over age 40, and are three times more likely to be present in African-American women than in Caucasian women. Fibroids do not need to be removed unless they are causing symptoms that interfere with a woman's normal activities.
Treatment of endometriosis is the reason for 20% of hysterectomies. The endometrium is the lining of the uterus. Endometriosis occurs when the cells from the endometrium begin growing outside the uterus. The outlying endometrial cells respond to the hormones that control the menstrual cycle, bleeding each month the way the lining of the uterus does. This causes irritation of the surrounding tissue, leading to pain and scarring.
Twenty percent of hysterectomies are done because of heavy or abnormal vaginal bleeding that cannot be linked to any specific cause and cannot be controlled by other means. Another 20% are performed to treat prolapsed uterus, pelvic inflammatory disease, or endometrial hyperplasia, a potentially pre-cancerous condition.
About 10% of hysterectomies are performed to treat cancer of the cervix, ovaries, or uterus. Women with cancer in one or more of these organs almost always have the organ(s) removed as part of their cancer treatment.
Demographics
Hysterectomy is the second most common operation performed on women in the United States. About 556,000 of these surgeries are done annually. By age 60, approximately one out of every three American women will have had a hysterectomy. It is estimated that 30% of hysterectomies are unnecessary.
The frequency with which hysterectomies are performed in the United States has been questioned in recent years. It has been suggested that a large number of hysterectomies are performed unnecessarily. The United States has the highest rate of hysterectomies of any country in the world. Also, the frequency of this surgery varies across different regions of the United States. Rates are highest in the South and Midwest, and are higher for African-American women. In recent years, although the number of hysterectomies performed has declined, the number of hysterectomies performed on younger women aged 30s and 40s is increasing, and 55% of all hysterectomies are performed on women ages 35–49.
Description
A hysterectomy is classified according to what structures are removed during the procedure and what method is used to remove them.
Total hysterectomy
A total hysterectomy, sometimes called a simple hysterectomy, removes the entire uterus and the cervix. The ovaries are not removed and continue to secrete hormones. Total hysterectomies are usually performed in the case of uterine and cervical cancer. This is the most common kind of hysterectomy.
In addition to a total hysterectomy, a procedure called a bilateral salpingo-oophorectomy is sometimes performed. This surgery removes the ovaries and the fallopian tubes. Removal of the ovaries eliminates the main source of the hormone estrogen, so menopause occurs immediately. Removal of the ovaries and fallopian tubes is performed in about one-third of hysterectomy operations, often to reduce the risk of ovarian cancer.
Subtotal hysterectomy
If the reason for the hysterectomy is to remove uterine fibroids, treat abnormal bleeding, or relieve pelvic pain, it may be possible to remove only the uterus and leave the cervix. This procedure is called a subtotal hysterectomy (or partial hysterectomy), and removes the least amount of tissue. The opening to the cervix is left in place. Some women believe that leaving the cervix intact aids in their achieving sexual satisfaction. This procedure, which used to be rare, is now performed more frequently.
Subtotal hysterectomy is easier to perform than a total hysterectomy, but leaves a woman at risk for cervical cancer. She will still need to get yearly Pap smears.
Radical hysterectomy
Radical hysterectomies are performed on women with cervical cancer or endometrial cancer that has spread to the cervix. A radical hysterectomy removes the uterus, cervix, above part of the vagina, ovaries, fallopian tubes, lymph nodes, lymph channels, and tissue in the pelvic cavity that surrounds the cervix. This type of hysterectomy removes the most tissue and requires the longest hospital stay and a longer recovery period.
Methods of hysterectomy
There are two ways that hysterectomies can be performed. The choice of method depends on the type of hysterectomy, the doctor's experience, and the reason for the hysterectomy.
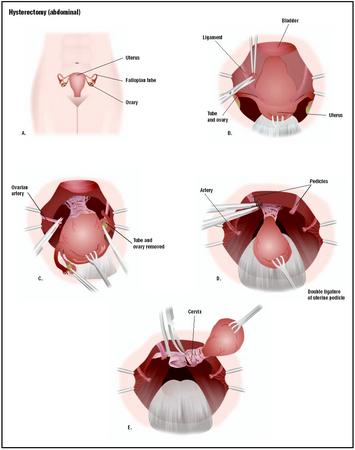
ABDOMINAL HYSTERECTOMY. About 75% of hysterectomies performed in the United States are abdominal hysterectomies. The surgeon makes a 4–6-in (10–15-cm) incision either horizontally across the pubic hair line from hip bone to hip bone or vertically from navel to pubic bone. Horizontal incisions leave a less noticeable scar, but vertical incisions give the surgeon a better view of the abdominal cavity. The blood vessels, fallopian tubes, and ligaments are cut away from the uterus, which is lifted out.
Abdominal hysterectomies take from one to three hours. The hospital stay is three to five days, and it takes four to eight weeks to return to normal activities.
The advantages of an abdominal hysterectomy are that the uterus can be removed even if a woman has internal scarring (adhesions) from previous surgery or her fibroids are large. The surgeon has a good view of the abdominal cavity and more room to work. Also, surgeons tend to have the most experience with this type of hysterectomy. The abdominal incision is more painful than with vaginal hysterectomy, and the recovery period is longer.
VAGINAL HYSTERECTOMY. With a vaginal hysterectomy, the surgeon makes an incision near the top of the vagina. The surgeon then reaches through this incision to cut and tie off the ligaments, blood vessels, and fallopian tubes. Once the uterus is cut free, it is removed through the vagina. The operation takes one to two hours. The hospital stay is usually one to three days, and the return to normal activities takes about four weeks.
The advantages of this procedure are that it leaves no visible scar and is less painful. The disadvantage is that it is more difficult for the surgeon to see the uterus and surrounding tissue. This makes complications more common. Large fibroids cannot be removed using this technique. It is very difficult to remove the ovaries during a vaginal hysterectomy, so this approach may not be possible if the ovaries are involved.
Vaginal hysterectomy can also be performed using a laparoscopic technique. With this surgery, a tube containing a tiny camera is inserted through an incision in the navel. This allows the surgeon to see the uterus on a video monitor. The surgeon then inserts two slender instruments through small incisions in the abdomen and uses them to cut and tie off the blood vessels, fallopian tubes, and ligaments. When the uterus is detached, it is removed though a small incision at the top of the vagina.
This technique, called laparoscopic-assisted vaginal hysterectomy, allows surgeons to perform a vaginal hysterectomy that might otherwise be too difficult. The hospital stay is usually only one day. Recovery time is about two weeks. The disadvantage is that this operation is relatively new and requires great skill by the surgeon.
Any vaginal hysterectomy may have to be converted to an abdominal hysterectomy during surgery if complications develop.
Diagnosis/Preparation
Before surgery the doctor will order blood and urine tests. The woman may also meet with the anesthesiologist to evaluate any special conditions that might affect the administration of anesthesia. On the evening before the operation, the woman should eat a light dinner and then have nothing to eat or drink after midnight.
Aftercare
After surgery, a woman will feel some degree of discomfort; this is generally greatest in abdominal hysterectomies because of the incision. Hospital stays vary from about two days (laparoscopic-assisted vaginal hysterectomy) to five or six days (abdominal hysterectomy with bilateral salpingo-oophorectomy). During the hospital stay, the doctor will probably order more blood tests.
Return to normal activities such as driving and working takes anywhere from two to eight weeks, again depending on the type of surgery. Some women have emotional changes following a hysterectomy. Women who have had their ovaries removed will probably start hormone replacement therapy.
Risks
Hysterectomy is a relatively safe operation, although like all major surgery it carries risks. These include unanticipated reaction to anesthesia, internal bleeding, blood clots, damage to other organs such as the bladder, and post-surgery infection.
Other complications sometimes reported after a hysterectomy include changes in sex drive, weight gain, constipation, and pelvic pain. Hot flashes and other symptoms of menopause can occur if the ovaries are removed. Women who have both ovaries removed and who do not take estrogen replacement therapy run an increased risk for heart disease and osteoporosis (a condition that causes bones to be brittle). Women with a history of psychological and emotional problems before the hysterectomy are likely to experience psychological difficulties after the operation.
As in all major surgery, the health of the patient affects the risk of the operation. Women who have chronic heart or lung diseases, diabetes, or iron-deficiency anemia may not be good candidates for this operation. Heavy smoking, obesity, use of steroid drugs, and use of illicit drugs add to the surgical risk.
Normal results
Although there is some concern that hysterectomies may be performed unnecessarily, there are many conditions for which the operation improves a woman's quality of life. In the Maine Woman's Health Study, 71% of women who had hysterectomies to correct moderate or severe painful symptoms reported feeling better mentally, physically, and sexually after the operation.
Morbidity and mortality rates
The rate of complications differs by the type of hysterectomy performed. Abdominal hysterectomy is associated with a higher rate of complications (9.3%), while the overall complication rate for vaginal hysterectomy is 5.3%, and 3.6% for laparoscopic vaginal hysterectomy. The risk of death from hysterectomy is about one in every 1,000 women. The rates of some of the more commonly reported complications are:
- excessive bleeding (hemorrhaging): 1.8–3.4%
- fever or infection: 0.8–4.0%
- accidental injury to another organ or structure: 1.5–1.8%
Alternatives
Women for whom a hysterectomy is recommended should discuss possible alternatives with their doctor and consider getting a second opinion , since this is major surgery with life-changing implications. Whether an alternative is appropriate for any individual woman is a decision she and her doctor should make together. Some alternative procedures to hysterectomy include:
- Embolization. During uterine artery embolization, interventional radiologists put a catheter into the artery that leads to the uterus and inject polyvinyl alcohol particles right where the artery leads to the blood vessels that nourish the fibroids. By killing off those blood vessels, the fibroids have no more blood supply, and they die off. Severe cramping and pain after the procedure is common, but serious complications are less than 5% and the procedure may protect fertility.
- Myomectomy . A myomectomy is a surgery used to remove fibroids, thus avoiding a hysterectomy. Hysteroscopic myomectomy, in which a surgical hysteroscope (telescope) is inserted into the uterus through the vagina, can be done on an outpatient basis. If there are large fibroids, however, an abdominal incision is required. Patients typically are hospitalized for two to three days after the procedure and require up to six weeks recovery. Laparoscopic myomectomies are also being done more often. They only require three small incisions in the abdomen, and have much shorter hospitalization and recovery times. Once the fibroids have been removed, the surgeon must repair the wall of the uterus to eliminate future bleeding or infection.
- Endometrial ablation. In this surgical procedure, recommended for women with small fibroids, the entire lining of the uterus is removed. After undergoing endometrial ablation, patients are no longer fertile. The uterine cavity is filled with fluid and a hysteroscope is inserted to provide a clear view of the uterus. Then, the lining of the uterus is destroyed using a laser beam or electric voltage. The procedure is typically done under anesthesia, although women can go home the same day as the surgery. Another newer procedure involves using a balloon, which is filled with superheated liquid and inflated until it fills the uterus. The liquid kills the lining, and after eight minutes the balloon is removed.
- Endometrial resection. The uterine lining is destroyed during this procedure using an electrosurgical wire loop (similar to endometrial ablation).
Resources
periodicals
Kovac, S. Robert. "Hysterectomy Outcomes in Patients with Similar Indications." Obstetrics & Gynecology 95, no. 6 (June 2000): 787–93.
organizations
American Cancer Society. 1599 Clifton Rd., NE, Atlanta, GA 30329-4251. (800) 227-2345. http://www.cancer.org .
American College of Obstetricians and Gynecologists. 409 12th St., SW, P.O. Box 96920, Washington, DC 20090-6920. http://www.acog.org .
National Cancer Institute. Building 31, Room 10A31, 31 Center Drive, MSC 2580, Bethesda, MD 20892-2580. (800) 422-6237. http://www.nci.nih.gov .
other
Bachmann, Gloria. "Hysterectomy." eMedicine. May 3, 2002 [cited March 13, 2003]. http://www.emedicine.com/med/topic3315.htm .
Bren, Linda. "Alternatives to Hysterectomy: New Technologies, More Options." Food and Drug Administration. October 29, 2001 [cited March 13, 2003]. http://www.fda.gov/fdac/features/2001/601_tech.html .
Debra Gordon
Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Hysterectomies are usually performed under the strict conditions of a hospital operating room . The procedure is generally performed by a gynecologist, a medical doctor who has specialized in the areas of women's general health, pregnancy, labor and childbirth, prenatal testing, and genetics.
QUESTIONS TO ASK THE DOCTOR
- Why is a hysterectomy recommended for my particular condition?
- What type of hysterectomy will be performed?
- What alternatives to hysterectomy are available to me?
- Will I have to start hormone replacement therapy?
I would appreciate your reply. Thank you for your time.
Martha
CASE STUDY IN SURGERY:
1. Solutions Used?
2.Suture Name and Size in: PERITONEUM,FASCIA,SUBCUTANEOUS,SUBCUTICULAR SKIN
3. Drains?
4. Needele Name?
5. Needle Tape?
6. Medications required in surgery?
7. Amount used?
Thanks.
Thank you so much for providing the information.
i am concern about the dryness, i am starting a new relationship and i do not how to handle it and how to disclose this to my new partner. i have stayed away from relationships because the fear, please help! I'm only 42 years old.
please advise... anyone?
I was wondering what types of blood tests do they run before a total hysterectomy....and why
Thanks
Sue G.
This site is very informative and helped me a lot with everything else.
March 2, 2009 ---10 days ago I had a hysterectomy, I was diagnosed with having a large cyst that also infected one of my ovaries, I had really good hospital care. Stayed in hospital for two days, felt nausea after I left hospital, I have a soft diet, chicken, fruits and vegetables.The symptoms I have now: Mild discomfort from the incision, my tummy feels swollen, I feel gas, but not problem going to bathroom, I still fell the urge to go pee quite often, my doctor told me to wear a girdle for 6 weeks, not driving for at least two weeks, full rest for 4 weeks, I do walk around my house, get tired after I am up for a while.
My doctor told me that sex life after the hysterectomy is diferent for every woman, also told me not to intent to have sex for 6 weeks after the operation ( she also said some man have a problem waiting for woman to heal) My life and health is much more important than sex, or how my husband feels about waiting until I heal, don't let yours talk to you into engaging in sex if he respects your life and health he will take care of you and wait
like mine is.
I wanted to share this and hope the information is useful.
Thank you and God Bless
I am contemplating going through with a hysterectomy, but am concerned with the fact that Women with pre=existing psychological problems (mine being chronic anxiety and depression disorder) can be a risk for more of these problems, or that it could be difficult recovering psychologically from this.
Would leaving the ovaries in tact illiminate this possible problem? Could you please explain more. I would greatly appreciate it. Thank you
Theresa in Vancouver Canada
My Mom has gone through this subtotal hysterectomy surgery (through abdominal surgery)in 2001.After that she has gained some weight and faced some problems which generally occurred after surgery like tiredness, pain in joints, in bones.Now days(Jan 2010) she has facing a new problem of pain in fallopian tube due to some mis movement of body during work.After consulting with surgeon and getting his treatment, we came to know that her pain is decreased temporary and its side effect occur on her digestion system.Due to that we skip that pain killer antibiotic and firstly concentrate on recovery of digestion.But now it is too much difficult for her to tolerate that pain.So we are planning to go for fallopian tube surgery.
Should we go for that?
Or it will make another problem?
Please tell me an effective solution on this, causes of it and if surgery then what it effects?
Thank You!Waiting for your reply.
My mother was scared to go in after her doctor told her this would be her best option to get her change of life (she hadn't reached menopause and doctor probably just wanted to make money off of her). Anyhow, she went in and was in terrible pain. Her daily calls to the doctor's office turned out to be a nuisance for them as they would tell her "here take more of these pain meds" into a "If its really that bad go to ER". She went to ER 4 days after being released from surgery. They treated her for heart probs and let her go.
Still excrutiating pain... it took them 31 days where she could no longer carry on and went back to ER. There one brilliant doctor decided she was septic. they made a mistake in the surgery.
My mother died after 9 weeks battling to recover from this mistake (she'd be alive today if the hospitals and doctors reexamined her and caught their mistake before it was in her blood and also if they didnt overmedicate her after she survived the big surgery.
We lost my mother on Christmas... what a way to go. I watched her bleed to death in those 9 weeks (literally the blood would run down from the bed from her colon). The worst way to watch your beautiful mother suffer.
If you dont need the surgery, dont do it. If you do it, get a second opinion. Too many male doctors think women over react (hysteria... hence the name) and ignore true real complaints.
If you want to know who did this:
Dr. Melnick (Whittier, CA)
Dr. Maguire (Brea, CA)
St. Jude Hospital (Fullerton, CA)
Beware. Email me if you want further info. But dont go through the pain our family has... its tragic and unnecessary. It changed my life for good.
Now at 60 I test posstivr to the BRAC 2. I guess my question is I went thru menopause at 50 with no hormone replacement and am having no problems with hot flashes . I am now 60 and have just had a histerictomy due to the high risk of ovation cancer. Of course I had everything removed. If I had no hot flashes before the surgry should I expect to have them now? So far it has been a week and I feel great! What should I expect?
Thanks,
Jane
Thanks,
Diane
I HAVE ADOUBT ABOUT THE VAGINAL HISTERECTOMY.MY MOTHER (63YR)IS ADMITTED IN HOSPITAL FOR THE SURGERY.THE DOCTOR TOLD HER UTEREUS ALMOST OUT SIDE THE BODY.SO VAGINAL SURGERY IS BETTER FOR HER.DUE TO THIS PROLAPS THE UTEREUS GOT INFECTED SO NEED 5 DAYS BEFORE SURGERY TO CLEAN IT.SHE IS SO WEAK WITH THIS DISEASE.IS THERE ANY RISK FACTOR IN THIS SURGERY?SHE HAS SOME PSCYCHOLOGICAL PROBLEM ALSO.OVER TENSION AND ANXIETY.IS IT WILL AFFECT HER DURING SURGERY?PLEASE ANSWER ME SOON.BECAUSE THE SURGERY IS ON 8 AUGUEST 2013.
Please help me. I have done my hysterectomy in 2009 November and now I have started bleeding, what can be the couse of this?