Myringotomy and ear tubes
Definition
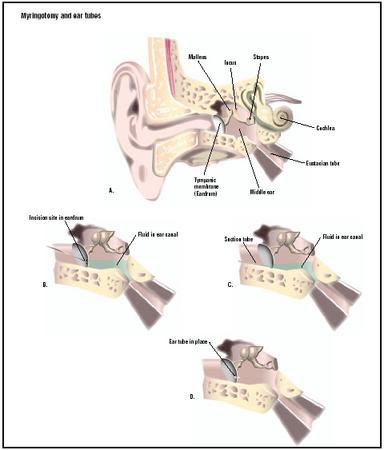
Myringotomy is a surgical procedure in which a small incision is made in the eardrum (the tympanic membrane), usually in both ears. The English word is derived from myringa, modern Latin for drum membrane, and tome, Greek for cutting. It is also called myringocentesis, tympanotomy, tympanostomy, or paracentesis of the tympanic membrane. Fluid in the middle ear can be drawn out through the incision.
Ear tubes, or tympanostomy tubes, are small tubes open at both ends that are inserted into the incisions in the eardrums during myringotomy. They come in various shapes and sizes and are made of plastic, metal, or both. They are left in place until they fall out by themselves or until they are removed by a doctor.
Purpose
Myringotomy with the insertion of ear tubes is an optional treatment for inflammation of the middle ear
with fluid collection (effusion) that lasts longer than three months (chronic otitis media with effusion) and does not respond to drug treatment. This condition is also called glue ear. Myringotomy is the recommended treatment if the condition lasts four to six months. Effusion refers to the collection of fluid that escapes from blood vessels or the lymphatic system. In this case, the effusion collects in the middle ear.
Initially, acute inflammation of the middle ear with effusion is treated with one or two courses of antibiotics . Antihistamines and decongestants have been used, but they have not been proven effective unless there is also hay fever or some other allergic inflammation that contributes to the problem. Myringotomy with or without the insertion of ear tubes is not recommended for initial treatment of otherwise healthy children with middle ear inflammation with effusion.
In about 10% of children, the effusion lasts for three months or longer, when the disease is considered chronic. In children with chronic disease, systemic steroids may help, but the evidence is not clear, and there are risks.
When medical treatment doesn't stop the effusion after three months in a child who is one to three years old, is otherwise healthy, and has hearing loss in both ears, myringotomy with insertion of ear tubes becomes an option. If the effusion lasts for four to six months, myringotomy with insertion of ear tubes is recommended.
The purpose of myringotomy is to relieve symptoms, to restore hearing, to take a sample of the fluid to examine in the laboratory in order to identify any microorganisms present, or to insert ear tubes.
Ear tubes can be inserted into the incision during myringotomy and left there. The eardrum heals around them, securing them in place. They usually fall out on their own in six to 12 months or are removed by a doctor.
While the tubes are in place, they keep the incision from closing, keeping a channel open between the middle ear and the outer ear. This allows fresh air to reach the middle ear, allowing fluid to drain out, and preventing pressure from building up in the middle ear. The patient's hearing returns to normal immediately and the risk of recurrence diminishes.
Demographics
In the United States, myringotomy and tube placement have become a mainstay of treatment for recurrent otitis media in children. An article published in the March 1998 Consumer Reports stated that the " … number of myringotomies has risen nearly 250 percent in recent years, making the operation the sixth most common operation in the United States." According to the New York University School of Medicine, myringotomy and tube placement is the most common surgical procedure performed in children as of 2003, largely because otitis media is the most common reason for children to be taken to a doctor's office.
Myringotomy in adults is a less common procedure than in children, primarily because adults benefit from certain changes in the anatomy of the middle ear that occur after childhood. In particular, the adult ear is less likely to accumulate fluid because the Eustachian tube, which connects the middle ear to the throat area, lies at about a 45-degree angle from the horizontal. This relatively steep angle means that the force of gravity helps to keep fluids from the throat containing disease organisms out of the middle ear. In children, however, the Eustachian tube is only about 10 degrees above the horizontal, which makes it relatively easy for disease organisms to migrate from the nose and throat into the inner ear. Myringotomies in adults are usually performed as a result of barotrauma that is also known as pressure-related ear pain or barotitis media. Barotrauma refers to earache caused by unequal air pressure on the inside and outside of the eardrum. Adults with very narrow Eustachian tubes may experience barotrauma in relation to scuba diving, using elevators, or frequent flying. A myringotomy with tube insertion may be performed if the condition is not helped by decongestants or antibiotics.
Most myringotomies in children are performed in children between one and two years of age. One Canadian study found that the number of myringotomies performed was 12.8 per thousand for children 11 months old or younger; 54.2 per thousand for children between 12 and 23 months old; and 11.1 per thousand for children between three and 15 years old. Sex and race do not appear to affect the number of myringotomies in any age group, although boys are reported to have a slightly higher rate of ear infections than girls.
Description
When a conventional myringotomy is performed, the ear is washed, a small incision made in the eardrum, the fluid sucked out, a tube inserted, and the ear packed with cotton to control bleeding.
Recent developments include the use of medical acupuncture to control pain during the procedure, and the use of carbon dioxide lasers to perform the myringotomy itself. Laser-assisted myringotomy can be performed in a doctor's office with only a local anesthetic. It has several advantages over the older technique: it is less painful; less frightening to children; and minimizes the need for tube insertion because the hole in the eardrum produced by the laser remains open longer than an incision done with a scalpel.
Another technique to keep the incision in the eardrum open without the need for tube insertion is application of a medication called mitomycin C, which was originally developed to treat bladder cancer. The mitomycin prevents the incision from sealing over. As of 2003, however, this approach is still in its experimental stages.
There has also been an effort to design ear tubes that are easier to insert or to remove, and to design tubes that stay in place longer. As of 2003, ear tubes come in various shapes and sizes.
Diagnosis/Preparation
The diagnosis of otitis media is based on the doctor's visual examination of the patient's ear and the patient's symptoms. Patients with otitis media complain of earache and usually have a fever, sometimes as high as 105°F (40.5°C). There may or may not be loss of hearing. Small children may have nausea and vomiting. When the doctor looks in the ear with an otoscope, the patient's eardrum will look swollen and may bulge outward. The doctor can evaluate the presence of fluid in the middle ear either by blowing air into the ear, known as insufflation, or by tympanometry, which is an indirect measurement of the mobility of the eardrum. If the eardrum has already ruptured, there may be a watery, bloody, or pus-streaked discharge.
Fluid removed from the ear can be taken to a laboratory for culture. The most common bacteria that cause otitis media are Pneumococcus , Haemophilus influenzae , and Moraxella catarrhalis . Some cases are caused by viruses, particularly respiratory syncytial virus (RSV).
A child scheduled for a myringotomy should not have food or water for four to six hours before anesthesia. Antibiotics are usually not needed.
If local anesthesia is used, a cream containing lidocaine and prilocaine is applied to the ear canal about 30 minutes before the myringotomy. If medical acupuncture is used for pain control, the acupuncture begins about 40 minutes before surgery and is continued during the procedure.
Aftercare
The use of antimicrobial drops is controversial. Water should be kept out of the ear canal until the eardrum is intact. A doctor should be notified if the tubes fall out.
Risks
The risks include:
- cutting the outer ear
- formation at the myringotomy site of granular nodes due to inflammation
- formation of a mass of skin cells and cholesterol in the middle ear that can grow and damage surrounding bone (cholesteatoma)
- permanent perforation of the eardrum
It is also possible that the incision won't heal properly, leaving a permanent hole in the eardrum. This result can cause some hearing loss and increases the risk of infection.
The ear tube may move inward and get trapped in the middle ear, rather than move out into the external ear, where it either falls out on its own or can be retrieved by a doctor. The exact incidence of tubes moving inward is not known, but it could increase the risk of further episodes of middle-ear inflammation, inflammation of the eardrum or the part of the skull directly behind the ear, formation of a mass in the middle ear, or infection due to the presence of a foreign body.
The surgery may not be a permanent cure. As many as 30% of children undergoing myringotomy with insertion of ear tubes need to undergo another procedure within five years.
The other risks include those associated with sedatives or general anesthesia. Some patients may prefer acupuncture for pain control in order to minimize these risks.
An additional element of postoperative care is the recommendation of many doctors that the child use ear plugs to keep water out of the ear during bathing or swimming to reduce the risk of infection and discharge.
Normal results
Parents often report that children talk better, hear better, are less irritable, sleep better, and behave better after myringotomy with the insertion of ear tubes. Normal results in adults include relief of ear pain and ability to resume flying or deep-sea diving without barotrauma.
Morbidity and mortality rates
Morbidity following myringotomy usually takes the form of either otorrhea, which is a persistent discharge from the ear, or changes in the size or texture of the eardrum. The risk of otorrhea is about 13%. If the procedure is repeated, the eardrum may shrink, retract, or become flaccid. The eardrum may also develop an area of hardened tissue. This condition is known as tympanosclerosis. The risk of hardening is 51%; its effects on hearing aren't known, but they appear to be insignificant.
A report published in 2002 indicates that morbidity following myringotomy in the United States is highest among children from families of low socioeconomic status. The study found that children from poor urban families had more episodes of otorrhea following tube insertion then children from suburban families. In addition, the episodes of otorrhea in the urban children lasted longer.
Mortality rates are extremely low; case studies of fatalities following myringotomy are rare in the medical literature, and most involve adults.
Alternatives
Preventive measures
There are several lifestyle issues related to high rates of middle ear infection. One of the most serious is parental smoking. One study of the effects of passive smoking on children's health estimated that as many as 165,000 of the myringotomies performed each year on American children are related to the use of tobacco in the household.
Another risk factor is daycare placement. A 1997 study at the University of North Carolina found that 31% of the children in a sample of 346 children in daycare required myringotomy with tube insertion as compared to 11% of 63 children cared for at home. In addition, the children in daycare who had ventilation tubes had to have the tubes reinserted three times as often as the children in home care with ventilation tubes.
A third factor that affects a child's risk of recurrent middle ear infection is breastfeeding. Researchers at the University of Arizona reported in 1993 that infants who had been breastfed exclusively for at least four months had significantly fewer middle ear infections as toddlers.
Other surgical approaches
There is some controversy among doctors as to whether removal of the adenoids helps to lower the risk of recurrent ear infections. A 2001 Canadian study reported that removing the child's adenoids at the time of the first insertion of ventilation tubes significantly reduced the likelihood of additional ear operations in children two years of age and older. Other doctors think that adenoidectomy at the time of tube placement should be performed only on children with a large number of risk factors for recurrent otitis media. Most agree that further study of this question is needed.
Alternative medicine
According to Dr. Kenneth Pelletier, former director of the program in complementary and alternative medicine at Stanford University, there is some evidence that homeopathic treatment is effective in reducing the pain of otitis media in children and lowering the risk of recurrence.
Resources
books
"Acute Otitis Media." Section 7, Chapter 84 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 2001.
Lanternier, Matthew L., MD. "Otolaryngology: Ear Pathology," Chapter 20 in The University of Iowa Family Practice Handbook , 4th edition, edited by Mark Graber, MD, and Matthew L. Lanternier, MD. St. Louis, MO: Mosby, 2001.
Pelletier, Kenneth R., MD. The Best Alternative Medicine, Part II: CAM Therapies for Specific Conditions: Otitis Media. New York: Simon & Schuster, 2002.
periodicals
Ah-Tye, C., J. L. Paradise, and D. K. Colborn. "Otorrhea in Young Children After Tympanostomy-Tube Placement for Persistent Middle-Ear Effusion: Prevalence, Incidence, and Duration." Pediatrics 107 (June 2001): 1251–1258.
Coyte, P. C., R. Croxford, W. McIsaac, et al. "The Role of Adjuvant Adenoidectomy and Tonsillectomy in the Outcome of the Insertion of Tympanostomy Tubes." New England Journal of Medicine 344 (April 19, 2001): 1188–1195.
Desai, S. N., J. D. Kellner, and D. Drummond. "Population-Based, Age-Specific Myringotomy with Tympanostomy Tube Insertion Rates in Calgary, Canada." Pediatric Infectious Disease Journal 21 (April 2002): 348–350.
Gates, George A., MD. "Otitis Media—The Pharyngeal Connection." Journal of the American Medical Association 282 (September 8, 1999): 987–999.
Jassir, D., C. A. Buchman, and O. Gomez-Marin. "Safety and Efficacy of Topical Mitomycin C in Myringotomy Patency." Otolaryngology—Head and Neck Surgery 124 (April 2001): 368–373.
Lin, Yuan-Chi, MD. "Acupuncture Anesthesia for a Patient with Complex Congenital Anomalies." Medical Acupuncture 13 (Fall/Winter 2002) [cited February 22, 2003]. http://www.medicalacupuncture.org/aama_marf/journal/vol13_2/poster3.html .
Perkins, J. A. "Medical and Surgical Management of Otitis Media in Children." Otolaryngology Clinics of North America 35 (August 2002): 811-825.
Siegel, G. J., and R. K. Chandra. "Laser Office Ventilation of Ears with Insertion of Tubes." Otolaryngology—Head and Neck Surgery 127 (July 2002): 60–66.
organizations
American Academy of Medical Acupuncture (AAMA). 4929 Wilshire Boulevard, Suite 428, Los Angeles, CA 90010. (323) 937-5514. http://www.medicalacupuncture.org .
American Academy of Otolaryngology, Head and Neck Surgery, Inc. One Prince Street, Alexandria, VA 22314-3357. (703) 836-4444. http://www.entnet.org .
American Academy of Pediatrics (AAP). 141 Northwest Point Boulevard, Elk Grove Village, IL 60007. (847) 434-4000. http://www.aap.org .
Mary Zoll, PhD
Rebecca Frey, PhD
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Myringotomies are performed by family practitioners, pediatricians, and otolaryngologists, who are surgeons who specialize in treating disorders of the ears, nose, and throat.
A conventional myringotomy is usually done in an ambulatory surgical unit under general anesthesia, although some physicians do it in the office with sedation and local anesthesia, especially in older children and adults. In either case, it is considered same-day surgery. Laserassisted myringotomies are usually performed in doctors' offices or outpatient surgery clinics.
QUESTIONS TO ASK THE DOCTOR
- What alternatives to myringotomy might work for my child?
- How can I lower my child's risk of recurrent ear infections?
- Do you perform laser-assisted myringotomies?
- What is your opinion of removing my child's adenoids to lower the risk of future hospitalizations?
Thanks
Is a third time a charm??? I wont know until then...
now than before I had them put in. This did not happen with the temporary tubes I had put in about
two years ago. The pressure is also bad. Is this caused because the tubes are to big?
Two weeks ago I had my permanent t-tubes removed from both ears and I now have tinnitus in the left ear also a constant beat similar to that of a heart beat, and it feels rather bunged up. The right ear seems to be fine. The physician said that they are healing fine and will see me in two months time. I fly in 17 days.
Is the above normal after surgery and should I be flying?
Thank you
Anne
Thanks
Deb
I am now 29 years old and have had t-tubes in situe in both ears for the last 5 years. Initially they seemed to help with my hearing, but over the last 2 years I seem to be getting constant ear infections. The doctors give me broad spectrum antibiotics which I take as prescribed, these don't work. Do I have any other options if I decide that I want the t-tubes to be taken out?
I know from provious experience that I need holes in my ear drums otherwise infection builds up behind them, one has actually burst in the past due to infection.
I have been suffering with my current ear infection for about 6 months. The pain makes my head throb, the constant discharge out of both ears is a pain and my balance and level of hearing is being adversley affected.
Please help!
TILL NOW whats your kink openion
What should I do? I've read several comments on line that removal of the tube doesn't help. ENT said hearing will
go back to "normal" after removal. What should I do? Please help.
like don't get water in the ear.I don t think I can take much more.Thanks Sharon
don't know how to sleep so I don't disturb my eartube,
its hard to sleep straight, so wondering if I can sleep left or right side?thanks..
Is it advicable ?
Thx for all your time in reading this I do appreciate it!!