Transurethral resection of the prostate
Definition
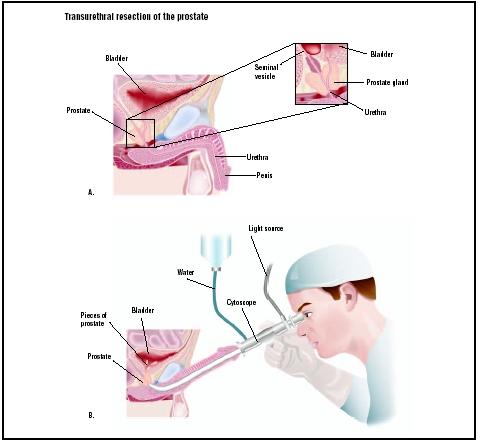
Transurethral resection of the prostate (TURP) is a surgical procedure by which portions of the prostate gland are removed through the urethra.
Purpose
The prostate is a gland that is part of the male reproductive system. It consists of three lobes, and surrounds the neck of the bladder and urethra (tube that channels urine from the bladder to the outside through the tip of the penis). The prostate weighs approximately one ounce (28 g), and is walnut-shaped. It is partly muscular and partly glandular, with ducts opening into the urethra. It secretes an antigen called prostate-specific antigen (PSA), and a slightly alkaline fluid that forms part of the seminal fluid (semen) that carries sperm.
A common prostate disorder is called benign prostatic hyperplasia (BPH) or benign prostatic enlargement (BPE). BPH is due to hormonal changes in the prostate, and is characterized by the enlargement or overgrowth of the gland as a result of an increase in the number of its constituent cells. BPH can raise PSA levels two to three times higher than normal. Men with increased PSA levels have a higher chance of developing prostate cancer. BPH usually affects the innermost part of the prostate first, and enlargement frequently results in a gradual squeezing of the urethra at the point where it runs through the prostate. The squeezing sometimes causes urinary problems, such as difficulty urinating. BPH may progress to the point of generating a dense capsule that blocks the flow of urine from the bladder, resulting in the inability to completely empty the bladder. Eventually, this could lead to bladder and kidney malfunction.
Transurethral resection of the prostate (TURP) is the treatment of choice for BPH, and the most common surgery performed for the condition. "Transurethral" refers to the procedure being performed through the urethra. "Resection " refers to surgical removal.
Demographics
Prostate disease usually occurs in men over age 40. BPH eventually develops in approximately 80% of all men. Prostate cancer occurs in one out of 10 men. In the United States, more than 30,000 men die of prostate cancer each year.
Description
TURP is a type of transurethral surgery that does not involve an external incision. The surgeon reaches the prostate by inserting an instrument through the urethra. In addition to TURP, two other types of transurethral surgery are commonly performed, transurethral incision of the prostate (TUIP), and transurethral laser incision of the prostate (TULIP). The TUIP procedure widens the urethra by making small cuts in the bladder neck (where the urethra and bladder meet), and in the prostate gland itself. In TULIP, a laser beam directed through the urethra melts the tissue.
The actual TURP procedure is simple. It is performed under general or local anesthesia. After an IV is inserted, the surgeon first examines the patient with a cystoscope, an instrument that allows him or her to see inside the bladder. The surgeon then inserts a device up the urethra via the penis opening, and removes the excess capsule material that has been restricting the flow of urine. The density of the normal prostate differs from that of the restricting capsule, making it relatively easy for the surgeon to tell exactly how much to remove. After excising the capsule material, the surgeon inserts a catheter into the bladder through the urethra for the subsequent withdrawal of urine.
Diagnosis/Preparation
BPH symptoms include:
- increase in urination frequency, and the need to urinate during the night
- difficulty starting urine flow
- a slow, interrupted flow and dribbling after urinating
- sudden, strong urges to pass urine
- a sensation that the bladder is not completely empty
- pain or burning during urination
In evaluating the prostate gland for BPH, the physician usually performs a complete physical examination as well as the following procedures:
- Digital rectal examination (DRE). Recommended annually for men over the age of 50, the DRE is an examination performed by a physician who feels the prostate through the wall of the rectum. Hard or lumpy areas may indicate the presence of cancer.
- Prostate-specific antigen (PSA) test. Also recommended annually for men over the age of 50, the PSA test measures the levels of prostate-specific antigen secreted by the prostate. It is normal to observe small quantities of PSA in the blood. PSA levels vary with age, and tend to increase gradually in men over age 60. They also tend to rise as a result of infection (prostatitis), BPH, or cancer.
If the results of the DRE and PSA tests are indicative of a significant prostate disorder, the examining
physician usually refers the patient to a urologist, a physician who specializes in diseases of the urinary tract and male reproductive system. The urologist performs additional tests, including blood and urine studies, to establish a diagnosis.
To prepare for TURP, patients should:
- Select an experienced TURP surgeon to perform the procedure.
- Purchase a mild natural bulk-forming laxative.
- Wear loose clothing on the morning of surgery.
- Ask friends or family to be available for assistance after surgery.
- Schedule a week off from work.
- Get sufficient sleep on the night before surgery.
Aftercare
When the patient awakens in the recovery room after the procedure, he already has a catheter in his penis, and is receiving pain medication via the IV line inserted prior to surgery.
The initial recovery period lasts approximately one week, and includes some pain and discomfort from the urinary catheter. Spastic convulsions of the bladder and prostate are expected as they respond to the surgical changes. The following medications are commonly prescribed after TURP:
- B&O suppository (Belladonna and Opium). This medication has the dual purpose of providing pain relief and reducing the ureteral and bladder spasms that follow TURP surgery. It is a strong medication that must be used only as prescribed.
- Bulk-forming laxative. Because of the surgical trauma and large quantities of liquids that patients are required to drink, they may need some form of laxative to promote normal bowel movements.
- Detrol. This pain reliever is not as strong as B&O. There may be wide variations in its effectiveness and the patient's response. It also controls involuntary bladder contractions.
- Macrobid. This antibiotic helps prevent urinary tract infections.
- Pyridium. This medication offers symptomatic relief from pain, burning, urgency, frequency, and other urinary tract discomfort.
When discharged from the hospital, patients are advised to:
- Refrain from alcoholic beverages.
- Avoid sexual activities for a few weeks.
- Avoid driving a car for a week or more.
- Keep domestic activities to a minimum.
- Avoid weight lifting or strenuous exercise.
- Check their temperature and report any fever to the physician.
- Practice good hygiene, especially of the hands and penis.
- Drink plenty of liquids.
Risks
Serious complications are less common for prostate surgery patients because of advances in operative methods. Nerve-sparing surgical procedures help prevent permanent injury to the nerves that control erection, as well as injury to the opening of the bladder. However, there are risks associated with prostate surgery. The first is the possible development of incontinence, the inability to control urination, which may result in urine leakage or dribbling, especially just after surgery. Normal control usually returns within several weeks or months after surgery, but some patients have become permanently incontinent. There is also a risk of impotence, the inability to achieve penile erection. For a month or so after surgery, most men are not able to become erect. Eventually, approximately 40–60% of men will be able to have an erection sufficient for sexual intercourse. They no longer ejaculate semen because removal of the prostate gland prevents that process. This effect is related to many factors, such as overall health and age. Other risks associated with TURP include:
- blood loss requiring transfusion
- postoperative urinary tract infection
- unsatisfactory long-term outcome
TURP syndrome effects 2–6% of TURP patients. Symptoms may include temporary blindness due to irrigation fluid entering the bloodstream. On very rare occasions, this can lead to seizures, coma, and even death. The syndrome may also include toxic shock due to bacteria entering the bloodstream, as well as internal hemorrhage.
Normal results
TURP patients usually notice urine flow improvement as soon as the catheter is removed. Other improvements depend on the condition of the patient's prostate before TURP, his age, and overall health status. Patients are told to expect the persistance of some pre-surgery symptoms. In fact, some new symptoms may appear following TURP, such as occasional blood and tissue in the urine, bladder spasms, pain when urinating, and difficulty judging when to urinate. TURP represents a major adaptation for the body, and healing requires some time. Full recovery may take up to one year. Patients are almost always satisfied with their TURP outcome, and the adaptation to new symptoms is offset by the disappearance of previous problems. For example, most patients no longer have to take daily prostate medication, and quickly learn to gradually increase the time between urinating while enjoying uninterrupted and more restful sleep at night.
Normal post-operative symptoms include:
- urination at night and reduced flow
- mild burning and stinging sensation while urinating
- reduced semen at ejaculation
- bladder control problems
- mild bladder spams
- fatigue
- urination linked to bowel movements
To eliminate these symptoms, patients are advised to:
- Exercise.
- Retrain their bladder
- Take all medications that were prescribed after TURP
- Inform themselves via support groups or pertinent reading
- Get plenty of rest to facilitate the post-surgery healing process
Morbidity and mortality rates
TURP reduces symptoms in 88% of BPH patients. TURP mortality rates are 0.2%, but they can be as high as 10% in patients over 80 years of age. Following surgery, inadequate relief of BPH symptoms occurs in 20–25% of patients, and 15–20% require another operation within 10 years. Urinary incontinence affects 2–4%, and 5–10% of TURP patients become impotent.
Alternatives
Conventional surgical alternatives for BPH patients include:
- Interstitial laser coagulation. In this procedure, a laser beam inserted in the urethra via a catheter heats and destroys the extra prostate capsule tissue.
- Transurethral needle ablation (TUNA). This technique was approved by the FDA in 1996. It uses radio waves to heat and destroy the enlarged prostate through needles positioned in the gland. It is generally less effective than TURP for reducing symptoms and increasing urine flow.
- Transurethral electrovaporization. This procedure is a modified version of TURP, and uses a device that produces electronic waves to vaporize the enlarged prostate.
- Photoselective vaporization of the prostate (PVP). This procedure uses a strong laser beam to vaporize the tissue in a 20–50 minute outpatient operation.
- Transurethral incision of the prostate (TUIP). In this procedure, a small incision is made in the bladder, followed by a few cuts into the sphincter muscle to release some of the tension.
- Transurethral microwave thermotherapy (TUMT). TUMT uses microwave heat energy to shrink the enlarged prostate through a probe inserted into the penis to the level of the prostate. This outpatient procedure takes about one hour. The patient can go home the same day, and is able to resume normal activities within a day or two. TUMT does not lead to immediate improvement, and it usually takes up to four weeks for urinary problems to completely resolve.
- Water-induced thermotherapy (WIT). WIT is administered via a closed-loop catheter system, through which heated water is maintained at a constant temperature. WIT is usually performed using only a local anesthetic gel to anesthetize the penis, and is very well tolerated. The procedure is FDA approved.
- Balloon dilation. In this procedure, a balloon is inserted in the urethra up to where the restriction occurs. At that point, the balloon expands to push out the prostate tissue and widen the urinary path. Improvements with this technique may only last a few years.
BPH patients have experienced improved prostate health from the following:
- Zinc supplements. This mineral plays an important role in prostate health because it decreases prolactin secretion and protects against heavy metals such as cadmium. Both prolactin and cadmium have been associated with BPH.
- Saw palmetto. Saw palmetto has long been used by Native Americans to treat urinary tract disturbances without causing impotence. It shows no significant side effects. A number of recent European clinical studies have also shown that fat soluble extracts of the berry help increase urinary flow and relieve other urinary problems resulting from BPH.
- Garlic. Garlic is believed to contribute to overall body and prostate health.
- Pumpkin seed oil. This oil contains high levels of zinc and has been shown to help most prostate disorders. Eating raw pumpkin seeds each day has long been a folk remedy for urinary problems, but German health authorities have recently recognized pumpkin seeds as a legitimate BPH treatment.
- Pygeum bark. The bark of the Pygeum africanus tree has been used in Europe since early times in the treatment of urinary problems. In France, 81% of BPH prescriptions are for Pygeum bark extract.
Recent developments in BPH treatment options include:
- The Urologix Targis TM System. This is a microwave device that uses the same heating method as TUMT. The procedure takes about an hour, and requires no anesthesia. The urologist inserts a flexible tube into the penis. This tube contains a unique microwave antenna that is able to generate very localized hot spots while cooling the surrounding areas. Diseased prostate tissue is destroyed with very little discomfort and a short recovery time. To date, men who have had this procedure have yet to develop impotence or incontinence.
- The Dornier MedTech Urowave. This device is another proprietary microwave heating device, similar to the Targis System.
- Transurethral alcohol treatment. This recent development is very promising for the treatment of BPH. The procedure involves injecting ethyl alcohol into the lateral and middle lobes of the prostate. The alcohol kills prostate tissue, which the body then absorbs. Early results are encouraging, and show that all patients (who were originally scheduled for TURP) were able to urinate freely after 24 hours. More studies are required to assess long-term outcomes.
- Prostatic stents. Stents are wire devices shaped like small springs or coils. They are placed within the prostate channel to maintain its patency (keep it open). These devices are currently under investigation and are not yet FDA-approved.
- Aromatase. This inhibitor drug suppresses excess levels of estrogen in the blood. In many men, estrogen is the primary growth-stimulating agent that causes prostatic overgrowth.
See also Cryotherapy ; Open prostatectomy .
Resources
books
Barrett, D. M., ed. Mayo Clinic on Prostate Health: Answers from the World-Renowned Mayo Clinic on Prostate Inflammation-Enlargement Cancer. New York: Kensington Pub. Corp., 2000.
Blandy, J. P. & R. G. Notley. Transurethral Resection. Boston: Butterworth-Heinemann, 1992.
Childs, S. J. Laser-Assisted Transurethral Resection of the Prostate (TURP). Philadelphia: Lippincott, Williams & Wilkins, 1993.
periodicals
Cimentepe, E., A. Unsal, and R. Saglam. "Randomized Clinical Trial Comparing Transurethral Needle Ablation with Transurethral Resection of the Prostate for the Treatment of Benign Prostatic Hyperplasia: Results at 18 Months." Journal of Endourology 17 (March 2003): 103-7.
Kaplan, S. A. "Comparison of Long-term Results of Transurethral Incision of the Prostate with Transurethral Resection of the Prostate, in Patients with Benign Prostatic Hypertrophy." Journal of Urology 168 (October 2002): 1657.
Kumar, P. V., M. P. Gomes, B. L. Davies, and A. G. Timoney. "A Computer Assisted Surgical Trainer for Transurethral Resection of the Prostate." Journal of Urology 168 (November 2002): 2111-14.
Kursh, E. D., R. Concepcion, S. Chan, P. Hudson, M. Ratner, and R. Eyre. "Interstitial Laser Coagulation versus Transurethral Prostate Resection for Treating Benign Prostatic Obstruction: A Randomized Trial with 2-year Follow-up." Urology 61 (March 2003): 673-8.
McAllister, W. J., O. Karim, R. O. Plail, D. R. Samra, M. J. Steggall, Q. Yang, and C. G. Fowler. "Transurethral electrovaporization of the Prostate: Is it Any Better than Conventional Transurethral Resection of the Prostate." British Journal of Urology International 91 (February 2003): 211-14.
Merrill, R. M., & C. L. Wiggins. "Incidental Detection of Population-based Prostate Cancer Incidence Rates through Transurethral Resection of the Prostate." Urologic Oncology 7 (September/October 2002): 213-19.
van Melick. H. H., G. E. van Venrooij, M. D. Eckhardt, and T. A. Boon. "A Randomized Controlled Trial Comparing Transurethral Resection of the Prostate, Contact Laser Prostatectomy and Electrovaporization in Men with Benign Prostatic Hyperplasia: Analysis of Subjective Changes, Morbidity and Mortality." Journal of Urology 169 (April 2003): 1411-16.
Yung, P. M., S. Chui-Kam, P. French, and T. M. Chan. "A Controlled Trial of Music and Pre-operative Anxiety in Chinese Men Undergoing Transurethral Resection of the Prostate." Journal of Advanced Nursing 39 (August 2002): 352-9.
organizations
American Foundation for Urologic Disease (AFUD). 1128 North Charles Street, Baltimore, MD 21201. (410) 468-1800. http://www.afud.org .
American Urological Association (AUA). 1120 North Charles Street, Baltimore, MD 21201. (410) 727-1100. http://www.auanet.org .
Cancer Information Service. National Cancer Institute, Building 31, Room 10A19, 9000 Rockville Pike, Bethesda, MD 20892. (800)4-CANCER. http://www.nci.nih.gov/cancerinfo/index.html .
other
"Anatomy of the Prostate Gland." University of Maryland Medicine. http://www.umm.edu/prostate/panat.htm .
"Prostate Disease Awareness." Monash University. http://www.med.monash.edu.au/healthpromotion/pamphlets/prostate/index.html .
"Transurethral Resection of the Prostate (TURP)." Family Practice Notebook. http://www.fpnotebook.com/URO110.htm .
"What is the Prostate?" AFUD. http://www.afud.org/conditions/pdbefore.html .
Monique Laberge, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Transurethral resection of the prostate is performed in hospitals by experienced urologic surgeons who are specialized in prostate disorders and in performing the TURP procedure.
QUESTIONS TO ASK THE DOCTOR
- What are the alternative treatments for benign prostatic hyperplasia?
- What are the risks involved with TURP?
- How long will it take to recover from the surgery?
- How painful is the TURP surgery?
- When and how often will the catheter require flushing?
- How long will it take to feel improvement?
- What are the post-operative problems?
- How will the surgery affect the ability to achieve erection?
- How many TURP procedures does the surgeon perform in a year?
- Will the surgery have to be repeated?
THANK YOU
YOURS TRULY
KAUSHIK SINHA .
keep it up.
what if after the TURP patient come back bleeding without trauma.
yours faithfully,
chigozie ohaegbuchi
port harcourt,
Nigeria
thank u so much.
WHICH ONE OF ALTERNATIVE PROCEDURES DOES NOT HAVE THE EFFECT OF STOPPING EGEJACULAtION OF SEMEN.
Regards
R.Bastani
It was suggested to undergo the operation again? having had the second procedure done every thing seemed to be normal except I was unable to get an erection.Although when my wife maniplates my penis I am able to reach ejaculation WITHOUT A FULL ERECTION. It never gets erect enough to penetrate my wife.
Now after about 21/2 years all the symtems are back, although I can sleep through the night.
BPH symptoms include:
•increase in urination frequency, (and the need to urinate during the night, this is now only very occasionally)
•difficulty starting urine flow
•a slow, interrupted flow and dribbling after urinating
•sudden, strong urges to pass urine
•a sensation that the bladder is not completely empty
•pain or burning during urination
Thank You For your considderation and time spent.
Best wishes John Slabbert
My problem is that in the last 4 weeks I have been awakened with a painful erection which I can only relieve by passing urine and this is happening on average 3 to 4 times per night do I have a problem.
KR - Las Vegas, Nevada
Now,urinating is not normal during the day time,. it still dribbles during the day (on and off). is this symptom a part of the recovery process?
as per the theory TURP requires 4-6 weeks period for recovery.
I have also experienced painful and reduced semen at ejaculation. is this normal? also please reflect on how to prevent and manage post TURP incontinence?
Thank you,
Regards,
KB- Toronto,Canada.
I've just undergone TURP (2 days ago), and I find the information on your site very accurate as I relate them to my own experience. I've read many of the questions posted on your User Contribution section, and I would very much like to know the respective answers. Please, where can I see them?
Thank you.
How long before you need addtl surgery?
Impact on sex life - minimal?
thanks joe
You really need to retrain the bladder--don't go every half hour or hour like you used to. Wait a while, and after a few weeks, the longer wait becomes a habit.
For those of you questioning whether or not to have the procedure, think about this. When you were young and outside, you used to see how far you could pee (can I hit that tree over there???). Middle age, you could write your initials in the snow if you were quick about it. When your prostrate enlarged greatly, you were proud to be able to dribble down your leg! At least that was my three stages. Now I think I could do the initials, if not actually hit the tree!
All in all, there were lots of little things that were annoying during recovery, but I would do it again in a flash!
Hope this helps!
Bob
there has not been any change in my symptoms...how long should it take before I feel a better
urine flow?
Can you kindly please provide me with a techincal info about the instrument of Laser TURP.
have read that one must strengthen the PC muscles through Kegel exercises. One way to locate them is to stop peeing midstreem. but I can't do this at the moment. other way is to use the muscles to jerk your penis up and down when erect. this I can do! So I am looking at a lot of pictures while I jiggle! but it is very hard to sense this muscle now. and I think it will be many months of determined exercise. I had a narrow neck to the bladder which was also removed, and i think much of the nerve system is gone and also in shock. I am 50 and have had problems for the last 20 years. I think Coffee is really bad. My father had the same problems. I have been a keen cyclist since I was 7 years old, Not sure that this was the cause, as I experienced pains in prostate area since I was 14 years old holding off on peeing or shitting.
my experience post op was horrible, as my intestines were extreemly bloated. the hospital coffee was really bad, and I would advise against drinking cofee post op for at least a week after the catheter is removed. if you are sensitive to filter coffee, often have a lot of air in the bowles, then make sure you have a neutral ph diet. the combination of urine retention post op and inflamed bowles was for me a nightmare and EXTREEMLY painful. the catheter had to me reinserted twice, and now I have to drain the bladder 3 times a day using a self inserted cathetar. I am convinced that pelvic floor exrcises, and kegel exercises will solve the problem long term. Please reply to these issues as you would a Blog. because your questions are not being answered and I think we should be sharing our experiences. regards, Mark
to help relieve bph symptons.I was able to pass urine,thanks to the
medication,but I was urinating twenty times a day.I chose the spinal block
which I thought, worked out real well, because I was numb from the waist
down and had no pain for several hours after the surgery.The worst part
for me was dealing with the cathater and all the related tubing for
flushing things out etc.Dragging all that stuff into the bathroom for a
bowel movement was a lot of fun.The catheter was very uncomfortable, but
was removed before breakfast on tuesday morning.I was in the hospital
for less than twenty four hours.It has now been four days and i still have
all the symtons i went in for in the first place. My doctor told me before
the surgery that would be the case.I was led to believe that enlarging
the uretha opening was the first step not a cure all instantly. I was
told to make an appointment with my doctor in two to three weeks, and
discuss where things are at that time and we will go from there.
He is keeping me on my three medications at this time which are probably
over stimulating everything. Hopefully he will take me off the meds and
I will get back to a normal life.I have had this problemm for a number
of years and was told by my doctor that turp, gave me the best chance of
not needing more surgery down the road. I feel fine and just waiting for
the healing process to end.Time will tell, but I feel relieved that i took
the first step, and I feel it will be a success, I really trust my doctor.
U.K.
I had TURP surgery at Darent Valley Hospital in KENT on Thursday 10th and I found reading your web-site very, very helpful. I have a couple of simple questions and would really appreciate your answers.
Before my surgery I was told to stop taking my Glucosamine Tablets , a week before surgery which I did. I just wanted to know if it's OK to restart taking them again ?
Also, before my surgery I was taking the following supplements, would it be OK to re-start taking them ? :
1) Vitamin Tablets
2) Omega-3 Fish Oil Tablets abt. 3,000 mg/day
3) Prostate Health Complex ( Tablets which I bought in the U.S. containing Zinc 15mg - Selenium 55mcg - Saw Palmetto extract 320mg - Pumpkin Seed oil 480mg - Lycopene 300mcg - Palmttic Acid 66.7mg -Stearic Acid 27.8mg - Oleic Acid 115.2 mg -and Linoleic Acid 266.4 mg )
4) Tablets to lower Cholesterol naturally (Mainly Plant Sterols/Stanols (Pine Tree) Calcium Carbonate and a load of other ingredients )
I thank you in advance for your reply and look forward to your reply.
Best Regards
Steve
I am 55+. TURP was done on 26.02.2011 by Dr. Vipul Aggarwal in B L Kapur Hospital, New Delhi & catheter was removed in 1.03.2011.LUTS were observed 5-6 months before and I was assessed with Ultrasound and Uroflowmetery for PVR etc. After getting PVR of 71 ml one one occassion and 261 on other the doctor advised for TURP, though with Flotral D I was feeling better but was not OK with its tendency to cause chest heavyness/pain/lethargy and congestion. Hence to avoid long term medication I gave in to Dr advise for TURP. 4 days in Hospital and post TURP twenty days, I have following experience:
1.Initially flow improved with Flotral D, Pyredium,Nuclai etc. but since last two days the flow has decreased and Blood clot followed by bloody urine happened.
2.Errection happens but it seems penis is shortened more on the left side.
3.Ejaculation also happened once in first week itself without any pain & with usual pleasure but seems it would not have been good enough for inter course. However, all stressful activity including sex is on hold for three weeks as per advise.
4.Revisit for follow up with complaints like: pain in the rectum, reduced flow and stream, urge to urinate etc with bleeding and clot lead the Sr doctor Dr.Rajinder Yadav to examine my rectum and PR again and has recommended to get admitted again for fulgration as the PR is boggy. I am scared and not prepared for another stint in hospital.Finast and Dicynine are prescribed.
5.I did not take Flotral D/Pyredium and now the urine colour is clear and no blood/clot etc.
6.I am off the work since 9.02.2011 since my symptoms lead to acute pain in chest, High BP, Pain in the groins as I also have Hernia etc.
My questions:
What is PR boggy?
How to determine if the PR is continually bleedinf and forming clots in the bladder.
Will irrigation solve the problem or Fulgration is a must?
Long sitting causes soar rectum and pain what to do?
Will TURP ultimately get reid of Flotral and other medicines?
How long will it take to reach fullfleged errection and normal sexual activity?
For those who plan to undertake TURP, a suggestion to try oral therapy and plunge only when extreem incontinence occurs. My choice was to take up TURP so as to get well fast to attend to Work and get rid of medicines.
All the best for your experience with TURP.
Magoo
Grscias, por su atención y quedo atento a su inportante y sabio consejo.
Thanks
Helal
Head of Sales & Marketing,
PFI Properties Limited,
House # 2, Road # 8, Gulshan Avenue,
Gulshan-1, Dhaka, Bangladesh
When standing up to urinate , my urine comes out in small quantity and stop. When sitting down to urinate all the urine comes out better but still a little slow. When my stool comes out the urine comes out better and faster. Would you please tell me what is going on ?
I also would like to know after how long is the best time to start having sex because I am still
feeling some pain due to the surgery even that is getting better.Also please tell me if it is ok to drive.
your,s
Evaluta.
I am seeing my Doctor in a couple of days and asking for a higher pain relief medication.
I had a bad experience after the operation, as the nursing staff were wheeling me out of recovery someone stood on my tube that yanked the catheter so that was a bit painful.
No not scare scaremongering, just my walk with getting through the pain barrier/s. I like the positive reads, hopefully in a few weeks I can print something positive
It's worth a try fella's, saves a lot of grief and pain.
Rich
Q.-Which type of anaesthesias are used for TURP?
Q.-whether it is major operation or minor?
Doc about it , but does not like the idea of taking any form of Testosterone he said my prostate may grow, doing some research on this topic, any feed back please let me know.
Any insights would be greatly appreciated.
Today as I write much better day still drinking plenty stream stronger and only one stream now.I am 65 in good health so I am hoping for a good outcome, if I could give any advice try to avoid constipation if at all possible. Thank you for the article very informative but I do think the forum of sharing real experiences is most helpful.
Thanks in advance.
Hari Shankar Jha
I Do