Hip replacement
Definition
Hip replacement is a procedure in which the surgeon removes damaged or diseased parts of the patient's hip joint and replaces them with new artificial parts. The operation itself is called hip arthroplasty . Arthroplasty comes from two Greek words, arthros or joint and plassein , "to form or shape." It is a type of surgery done to replace or reconstruct a joint. The artificial joint itself is called a prosthesis. Hip prostheses may be made of metal, ceramic, plastic, or various combinations of these materials.
Purpose
Hip arthroplasty has two primary purposes: pain relief and improved functioning of the hip joint.
Pain relief
Because total hip replacement (THR) is considered major surgery, with all the usual risks involved, it is usually not considered as a treatment option until the patient's pain cannot be managed any longer by more conservative nonsurgical treatment. These alternatives are described below.
Joint pain interferes with a person's quality of life in many ways. If the pain in the hip area is chronic, affecting the person even when he or she is resting, it can lead to depression and other emotional disturbances. Severe chronic pain also strains a person's relationships with family members, employer, and workplace colleagues; it is now recognized to be as the most common underlying cause of suicide in the United States.
In most cases, however, pain in the hip joint is a gradual development. Typically, the patient finds that their hip begins to ache when they are exercising vigorously, walking, or standing for a long time. They may cut back on athletic activities only to find that they are starting to limp when they walk and that sitting down is also becoming uncomfortable. Many patients then begin to have trouble driving, sitting through a concert or movie, or working at a desk without pain. It is usually at this point, when a person's ability to live independently is threatened, that he or she considers hip replacement surgery.
Joint function
Restoration of joint function is the other major purpose of hip replacement surgery. The hip joint is one of the most active joints in the human body, designed for many different types of movement. It consists of the head (top) of the femur (thighbone), which is shaped like a ball; and a part of the pelvic bone called the acetabulum, which looks like a hollow or socket. In a healthy hip joint, a layer of cartilage lies between the head of the femur and the acetabulum. The cartilage keeps the bony surfaces from grinding against each other, and allows the head of the femur to rotate or swivel in different directions inside the socket formed by the acetabulum. It is this range of motion, as well as the hip's ability to support the weight of the upper body, that is gradually lost when the hip joint deteriorates. The prostheses that are used in hip replacement surgery are intended to restore as much of the functioning of to the hip joint as possible. The level of function in the hip after the surgery depends in part on the reason for the damage to the joint.
Disorders and conditions that may lead to the need for hip replacement surgery include:
- Osteoarthritis (OA). Osteoarthritis is a disorder in which the cartilage in the joints of the body gradually breaks down, allowing the surfaces of the bones to rub directly and wear against each other. Eventually the patient experiences swelling, pain, inflammation, and increasing loss of mobility. OA most often affects appears most often in adults over age 45, and is thought to result from a combination of wear and tear on the joint, lifestyle, and genetic factors. As of 2003, OA is the most common cause of joint damage requiring hip replacement.
- Rheumatoid arthritis (RA). Rheumatoid arthritis is a disease that begins earlier in life than OA and affects the whole body. Women are three times as likely as men to develop RA. Its symptoms are caused by the immune system's attacks on the body's own cells and tissues. Patients with RA often suffer intense pain even when they are not putting weight on the affected joints. One man described his pain as " … like a hot poker that's stuck from this hip right through to the other one."
- Trauma. Damage to the hip joint from a fall, automobile accident, or workplace or athletic injury may trigger the process of cartilage breakdown in the hip joint.
- Avascular necrosis. Avascular necrosis, which is also called osteonecrosis, is a disorder caused by the loss of blood supply to bone tissue. Bone starved for blood supply becomes weak and eventually collapses. The most common reasons for loss of blood supply include trauma, the use of steroid medications, certain blood disorders, and alcoholism. Avascular necrosis often affects the top of the femur that forms part of the hip joint. It develops most frequently in adults between the ages of 30 and 50.
- Ankylosing spondylitis (AS). Ankylosing spondylitis is a less common form of arthritis that primarily affects the bones in the spine and pelvis. These bones gradually fuse together when the body replaces inflamed tendons or ligaments with new bone instead of elastic connective tissue. AS typically develops in the patient's late teens or early twenties, with three times as many men affected as women.
Demographics
Between 200,000 and 300,000 hip replacement operations are performed in the United States each year, most of them in patients over the age of 60. According to the American Academy of Orthopaedic Surgeons (AAOS), only 5–10% of total hip replacements as of 2002 were in patients younger than 50. There are two reasons for this concentration in older adults. Arthritis and other degenerative joint disorders are the most common health problems requiring hip replacement, and they become more severe as people grow older. The second reason is the limited life expectancy of the prostheses used in hip replacements. Because THR is a complex procedure and requires a long period of recovery after surgery, doctors generally advise patients to put off the operation as long as possible so that they will not need to undergo a second operation later to insert a new prosthesis.
This demographic picture is changing rapidly, however, because of advances in designing hip prostheses, as well as changes in older Americans' rising expectations of quality of life. Many people are less willing to tolerate years of pain or limited activity in order to postpone surgery. In addition, hip prostheses are lasting longer than those used in the 1960s; one study found that 65% of the prostheses in patients who had had THR before the age of 50 were still intact and functioning well 25 years after the surgery. A larger number of hip replacements are now being done in younger patients, and the operation itself is being performed more often. One expert estimates that the annual number of hip replacements in the United States will rise to 600,000 by 2015.
Description
Hip replacement surgery is a relatively recent procedure that had to wait for the invention of plastics and other synthetic materials to make reliable prostheses that could withstand years of wear. The first successful total hip replacement was performed in 1962 by Sir John Charnley (1911–1982), a British orthopedic surgeon who designed a device that is still known as a Charnley prosthesis. Charnley used a stainless steel ball mounted on a stem that was inserted into the patient's thighbone to replace the femoral head. A high-density polyethylene socket was fitted into the acetabular side of the joint. Both parts of the Charnley prosthesis were secured to their respective sides of the joint with an acrylic polymer cement. More recent developments include the use of cobalt chrome alloys or ceramic materials in place of stainless steel, as well as methods for holding the prosthesis in place without cement.
As of 2003, there are three major types of hip replacement surgery performed in the United States: a standard procedure for hip replacement; a newer technique known as minimally invasive surgery (MIS), pioneered in Chicago in February 2001; and revision surgery, which is done to replace a loosened or damaged prosthesis.
Standard hip replacement surgery
A standard hip replacement operation takes 1-1/2–3 hours. The patient may be given a choice of general, spinal, or epidural anesthesia. An epidural anesthesia, which is injected into the space around the spinal cord to block sensation in the lower body, causes less blood loss and also lowers the risk of blood clots or breathing problems after surgery. After the patient is anesthetized, the surgeon makes an incision 8–12 in (20–30 cm) long down the side of the patient's upper thigh. The surgeon may then choose to enter the joint itself from the side, back, or front. The back approach is the most common. The ligaments and muscles under the skin are then separated.
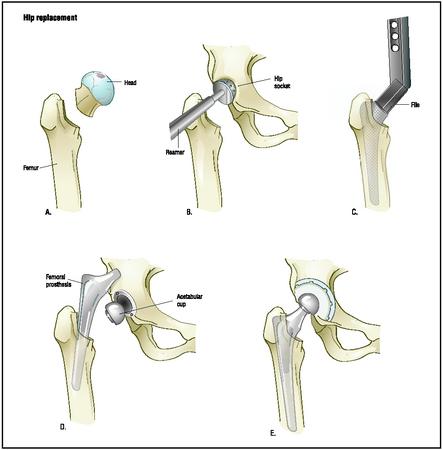
Once inside the joint, the surgeon separates the head of the femur from the acetabulum and removes the head with a saw. The surgeon uses a power drill and a special reamer to remove the cartilage from the acetabulum and shape it to accept the acetabular part of the prosthesis. This part of the new prosthesis is a curved piece of metal lined with plastic or ceramic.
After selecting the correct size for the patient, the surgeon inserts the acetabular component. If the new joint is to be cemented, the surgeon will attach the component to the bone with a type of epoxy. Otherwise the metal plate will be held in place by screws or by the tightness of the fit itself.
To replace the femoral head, the surgeon first drills a hollow inside the thighbone to accept a stem for the femoral component. The stem may be cemented in place or held in place by the tightness of the fit. A metal or ceramic ball to replace the head of the femur is then attached to the stem.
After the prosthesis is in place, an x ray is taken to verify that it is correctly positioned. The incision is then washed with saline solution as a safeguard against infection. The sutures used to close the deeper layers of tissue are made of a material that the body eventually absorbs, while the uppermost layer of skin is closed with metal surgical staples. The staples are removed 10–14 days after surgery.
Finally, a large triangular pillow known as a Charnley pillow is placed between the patient's ankles to prevent dislocation of the hip during the first few days after surgery.
Minimally invasive hip replacement surgery
Minimally invasive surgery (MIS) is a new technique of hip replacement introduced in 2001. Instead of making one long incision, the surgeon uses two 2-inch (5 cm) incisions or one 3.5-1/2-inch (9 cm) incision. Using newly designed smaller implements, the surgeon removes the damaged bone and inserts the parts of the new prosthesis. MIS hip replacement takes only an hour and a half; there is less bleeding and the patient can leave the hospital the next day. As of 2002, however, obese patients or those with very weak bones are not considered for MIS.
Revision surgery
Revision surgery is most commonly performed to replace a prosthesis that no longer fits or functions well because the bone in which it is implanted has deteriorated with age or disease. Revision surgery is a much more complicated process than first-time hip replacement; it sometimes requires a specialized prosthesis as well as bone grafts from the patient's pelvis, and its results are not usually as good. On the other hand, some patients have had as many as three revision operations with satisfactory results.
Diagnosis/Preparation
Because pain in the hip joint is usually a gradual development, its cause has been diagnosed in most cases by the time the patient is ready to consider hip replacement surgery. The doctor will have taken a careful medical
and employment history in order to determine the most likely cause of the pain and whether the patient's job may be a factor. The doctor will also ask about a family history of osteoarthritis as well as other disorders known to run in families. The patient will be asked about injuries, falls, or other accidents that may have affected the hip joint; and about his or her use of alcohol and prescription medications—particularly steroids, which can cause avascular necrosis.
The patient will then be given a complete physical examination to evaluate his or her fitness for surgery. Certain disorders, including Parkinson's disease; dementia and other conditions of altered mental status; kidney disease; advanced osteoporosis; disorders associated with muscle weakness; diabetes; and an unstable cardiovascular system are generally considered contraindications to hip replacement surgery. People with weakened immune systems may also be advised against surgery. In the case of obesity, the operation may be postponed until the patient loses weight. The stress placed on the hip joint during normal walking can be as high as three times the patient's body weight; thus each pound in weight reduction equals three pounds in stress reduction. Consequently, weight reduction lowers an obese patient's risk of complications after the operation.
The doctor will also order a radiograph, or x ray, of the affected hip. The results will show the location and extent of damage to the hip joint.
Diagnostic tests
The doctor may also order one or more specialized tests, depending on the known or suspected causes of the pain:
- Aspiration. Aspiration is a procedure in which fluid is withdrawn from the joint by a needle and sent to a laboratory for analysis. It is done to check for infection in the joint.
- Arthrogram. An arthrogram is a special type of x ray in which a contrast dye is injected into the hip to outline the cavity surrounding the joint.
- Magnetic resonance imaging (MRI). An MRI uses a large magnet, radio waves, and a computer to generate images of the head and back. It is helpful in diagnosing avascular necrosis.
- Computed tomography (CAT) scan. A CAT scan is another specialized type of x ray that uses computers to generate three-dimensional images of the hip joint. It is most often used to evaluate the severity of avascular necrosis and to obtain a more accurate picture of malformed or unusually shaped joints.
- Bone densitometry test. This test measures the density or strength of the patient's bones. It does not require injections; the patient lies flat on a padded table while an imager passes overhead. This test is most often given to patients at risk for osteoporosis or other disorders that affect bone density.
Preoperative preparation
Hip replacement surgery requires extensive and detailed preparation on the patient's part because it affects so many aspects of life.
LEGAL AND FINANCIAL CONSIDERATIONS. In the United States, physicians and hospitals are required to verify the patient's insurance benefits before surgery and to obtain precertification from the patient's insurer or from Medicare . Without health insurance, the total cost of a hip replacement as of 2002 can run as high as $35,000–$45,000. In addition to insurance documentation, patients are legally required to sign an informed consent form prior to surgery. Informed consent essentially signifies that the patient is a knowledgeable participant in making healthcare decisions. The doctor will discuss all of the following with the patient before he or she signs the form: the nature of the surgery; reasonable alternatives to the surgery; and the risks, benefits, and uncertainties of each option. Informed consent also requires the doctor to make sure that the patient understands the information that has been given.
MEDICAL CONSIDERATIONS. Patients are asked to do the following in preparation for hip replacement surgery:
- Get in shape physically by doing exercises for strengthening the heart and lungs, building up the muscles around the hip, and increasing the range of motion of the hip joint. Many clinics and hospitals distribute illustrated pamphlets of preoperation exercises.
- Loose weight if the surgeon recommends it.
- Quit smoking. Smoking weakens the cardiovascular system and increases the risks that the patient will have breathing difficulties under anesthesia.
- Make donations of one's own blood for storage in case a transfusion is necessary during surgery. This procedure is known as autologous blood donation ; it has the advantage of avoiding the risk of transfusion reactions or transmission of diseases from infected blood donors.
- Have necessary dental work completed before the operation. This precaution is necessary because small numbers of bacteria enter the bloodstream whenever a dentist performs any procedure that causes the gums to bleed. Bacteria from the mouth can be carried to the site of the hip replacement and cause an infection.
- Discontinue taking birth control pills and any anti-inflammatory medications ( aspirin or NSAIDs) two weeks before surgery. Most doctors also recommend discontinuing any alternative herbal preparations at this time, as some of them interact with anesthetics and pain medications.
LIFESTYLE CHANGES. Hip replacement surgery requires a long period of recovery at home after leaving the hospital. Since the patient's physical mobility will be limited, he or she should do the following before the operation:
- Arrange for leave from work, help at home, help with driving, and similar tasks and commitments.
- Obtain a handicapped parking permit.
- Check the house or apartment living quarters thoroughly for needed adjustments to furniture, appliances, lighting, and personal conveniences. People recovering from hip replacement surgery must minimize bending, stooping, and any risk of falling. There are several good guides available that describe household safety and comfort considerations in detail.
- Stock up on nonperishable groceries, cleaning supplies, and similar items in order to minimize shopping.
- Have a supply of easy-care clothing with elastic waistbands and simple fasteners in front rather than complicated ties or buttons in the back. Shoes should be slipons or fastened with Velcro.
Many hospitals and clinics now have "preop" classes for patients scheduled for hip replacement surgery. These classes answer questions regarding preparation for the operation and what to expect during recovery, but in addition they provide opportunities for patients to share concerns and experiences. Studies indicate that patients who have attended preop classes are less anxious before surgery and generally recover more rapidly.
Aftercare
Aftercare following hip replacement surgery begins while the patient is still in the hospital. Most patients will remain there for five to 10 days after the operation. During this period, the patient will be given fluids and antibiotic medications intravenously to prevent infection. Medications for pain will be given every three to four hours, or through a device known as a PCA (patient-controlled anesthesia). The PCA is a small pump that delivers a dose of medication into the IV when the patient pushes a button. To get the lungs back to normal functioning, a respiratory therapist will ask the patient to cough several times a day or breathe into blow bottles.
Aftercare during the hospital stay is also intended to lower the risk of a venous thromboembolism (VTE), or blood clot in the deep veins of the leg. Prevention of VTE involves medications to thin the blood; exercises for the feet and ankles while lying in bed; and wearing thromboembolic deterrent (TED) or deep vein thrombosis (DVT) stockings. TED stockings are made of nylon (usually white) and may be knee-length or thigh-length; they help to reduce the risk of a blood clot forming in the leg vein by putting mild pressure on the veins. TED stockings are worn for two to six weeks after surgery.
Physical therapy is also begun during the patient's hospital stay, often on the second day after the operation. The physical therapist will introduce the patient to using a walker or crutches and explain how to manage such activities as getting out of bed or showering without dislocating the new prosthesis. In addition to increasing the patient's level of physical activity each day, the physical therapist will help the patient select special equipment for recovery at home. Commonly recommended devices include a reacher for picking up objects without bending too far; a sock cone and special shoehorn; and bathing equipment.
Following discharge from the hospital , the patient may go to a skilled nursing facility, rehabilitation center, or directly home. Ongoing physical therapy is the most important part of recovery for the first four to five months following surgery. Most HMOs in the United States allow home visits by a home health aide, visiting nurse, and physical therapist for three to four weeks after surgery. The physical therapist will monitor the patient's progress, as well as suggest specific exercises to improve strength and range of motion. After the home visits, the patient is encouraged to take up other forms of physical activity in addition to the exercises; swimming, walking, and pedaling a stationary bicycle are all good ways to speed recovery. The patient may take a mild medication for pain (usually aspirin or ibuprofen) 30–45 minutes before an exercise session if needed.
Most patients can start driving six to eight weeks after the operation and return to work full time after eight to 10 weeks, depending on the amount and type of physical exertion their jobs requires. Some patients arrange to work on a part-time basis until their normal level of energy returns.
Risks
Hip replacement surgery involves both short- and long-term risks.
Short-term risks
The most common risks associated with hip replacement are as follows:
- Dislocation of the new prosthesis. Dislocation is most likely to occur in the first 10–12 weeks after surgery. It is a risk because the ball and socket in the prosthesis are smaller than the parts of the natural joint, and can move out of place if the patient places the hip in certain positions. The three major rules for avoiding dislocation are: Do not cross the legs when lying, sitting, or standing; never lean forward past a 90-degree angle at the waist; do not roll the legs inward toward each other—keep the feet pointed forward or turned slightly outward.
- Deep vein thrombosis (DVT). There is some risk (about 1.5% in the United States) of a clot developing in the deep vein of the leg after hip replacement surgery because the blood supply to the leg is cut off by a tourniquet during the operation. The blood-thinning medications and TED stockings used after surgery are intended to minimize the risk of DVT.
- Infection. The risk of infection is minimized by storing autologous blood for transfusion and administering intravenous antibiotics after surgery. Infections occur in fewer than 1% of hip replacement operations.
- Injury to the nerves that govern sensation in the leg. This problem usually resolves over time.
Long-term risks
The long-term risks of hip replacement surgery include:
- Inflammation related to wear and tear on the prosthesis. Tiny particles of debris from the prosthesis can cause inflammation in the hip joint and lead eventually to dissolution and loss of bone. This condition is known as osteolysis.
- Heterotopic bone. Heterotopic bone is bone that develops in the space between the femur and the pelvis after hip replacement surgery. It can cause stiffness and pain, and may have to be removed surgically. The cause is not completely understood as of 2002 but is thought to be a reaction to the trauma of the operation. In the United States, patients are usually given indomethacin (Indocin) to prevent this process; in Germany, surgeons are using postoperative radiation treatments together with Indocin.
- Changed length of leg. Some patients find that the operated leg remains slightly longer than the other leg even after recovery. This problem does not interfere with mobility and can usually be helped by an orthotic shoe insert.
- Loosening or damage to the prosthesis itself. This development is treated with revision surgery.
Normal results
Normal results are relief of chronic pain, greater ease of movement, and much improved quality of life. Specific areas of improvement depend on a number of factors, including the patient's age, weight, and previous level of activity; the disease or disorder that caused the pain; the type of prosthesis; and the patient's attitude toward recovery. In general, total hip replacement is considered one of the most successful procedures in modern surgery.
It is difficult to estimate the "normal" lifespan of a hip prosthesis. The figure quoted by many surgeons—10 to 15 years—is based on statistics from the early 1990s. It is too soon to tell how much longer the newer prostheses will last. In addition, as hip replacements become more common, the increased size of the worldwide patient database will allow for more accurate predictions. As of 2002, it is known that younger patients and obese patients wear out hip prostheses more rapidly.
Morbidity and mortality rates
Information about mortality and complication rates following THR is limited because the procedure is considered elective. In addition, different states and countries use different sets of measurements in evaluating THR outcomes. One Norwegian study found that patients who had THR between 1987 and 1999 had a lower long-term mortality rate than the age- and gender-matched Norwegian population. A Canadian study found a 1.6% mortality rate within 30 days of surgery for THR patients between 1981 and 1999. A 2002 report from the Mayo Clinic found that the overall frequency of serious complications (heart attack, pulmonary embolism, deep vein thrombosis, or death) within 30 days of THR was 2.2%, the risk being higher in patients over 70. The most important factor affecting morbidity and mortality rates in the United States, according to a 2002 Harvard study, is the volume of THRs performed at a given hospital or by a specific surgeon; the higher the volume, the better the outcomes.
Alternatives
Nonsurgical alternatives
The most common conservative alternatives to hip replacement surgery are assistive devices (canes or walkers) to reduce stress on the affected hip; exercise regimens to maintain joint flexibility; dietary changes, particularly if the patient is overweight; and analgesics , or painkilling medications. Most patients who try medication begin with an over-the-counter NSAID such as ibuprofen (Advil). If the pain cannot be controlled by nonprescription analgesics, the doctor may give the patient cortisone injections, which relieve the pain of arthritis by reducing inflammation. Unfortunately, the relief provided by cortisone tends to diminish with each injection; moreover, the drug can produce serious side effects.
Complementary and alternative (CAM) approaches
Complementary and alternative forms of therapy cannot be used as substitutes for hip replacement surgery, but they are helpful in managing pain before and after the operation, and in speeding physical recovery. Many patients also find that CAM therapies help them maintain a positive mental attitude in coping with the emotional stress of surgery and physical therapy. CAM therapies that have been shown to relieve the pain of rheumatoid and osteoarthritis include acupuncture, music therapy, naturopathic treatment, homeopathy, Ayurvedic medicine, and certain herbal preparations. Chronic pain from other disorders affecting the hip has been successfully treated with biofeedback, relaxation techniques, chiropractic manipulation, and mindfulness meditation.
Some types of movement therapy are recommended in order to postpone the need for hip surgery. Yoga, tai chi, qigong, and dance therapy help to maintain strength and flexibility in the hip joint, and to slow down the deterioration of cartilage and muscle tissue. Exercise in general has been shown to reduce a person's risk of developing osteoporosis.
Alternative surgical procedures
Other surgical options include:
- Osteotomy. An osteotomy is a procedure in which the surgeon cuts the thigh bone or pelvis in order to realign the hip. It is done more frequently in Europe than in the United States, but it has the advantage of not requiring artificial materials.
- Arthrodesis. This type of operation is rarely performed except in younger patients with injury to one hip. In this procedure, the head of the femur is fused to the acetabulum with a plate and screws. The major advantage of arthrodesis is that it places fewer restrictions on the patient's activity level than a hip replacement.
- Pseudarthrosis. In this procedure the head of the femur is removed without any replacement, resulting in a shorter leg on the affected side. It is usually performed when the patient's bones are too weak for implanting a prosthesis or when the hip joint is badly infected. This procedure is sometimes called a Girdlestone operation, after the surgeon who first used it in the 1940s.
Resources
books
Pelletier, Kenneth R., MD. The Best Alternative Medicine , Part II, "CAM Therapies for Specific Conditions." New York: Simon & Schuster, 2002.
Silber, Irwin. A Patient's Guide to Knee and Hip Replacement: Everything You Need to Know. New York: Simon & Schuster, 1999.
Trahair, Richard. All About Hip Replacement: A Patient's Guide. Melbourne, Oxford, and New York: Oxford University Press, 1998.
periodicals
"Arthritis—Hip Replacement." Harvard Health Letter 27 (February 2002): i4.
Chapman, K., Z. Mustafa, B. Dowling, et al. "Finer Linkage Mapping of Primary Hip Osteoarthritis Susceptibility on Chromosome 11q in a Cohort of Affected Female Sibling Pairs." Arthritis and Rheumatism 46 (July 2002): 1780–1783.
Daitz, Ben. "In Pain Clinic, Fruit, Candy and Relief." New York Times , December 3, 2002.
Drake, C., M. Ace, and G. E. Maale. "Revision Total Hip Arthroplasty." AORN Journal 76 (September 2002): 414–417, 419–427.
"Hip Replacement Surgery Viable Option for Younger Patients, Thanks to New Prostheses." Immunotherapy Weekly (March 13, 2002): 10.
Hungerford, D. S. "Osteonecrosis: Avoiding Total Hip Arthroplasty." Journal of Arthroplasty 17 (June 2002) (4 Supplement 1): 121–124.
Joshi, A. B., L. Marcovic, K. Hardinge, and J. C. Murphy. " Total Hip Arthroplasty in Ankylosing Spondylitis: An Analysis of 181 Hips." Journal of Arthroplasty 17 (June 2002): 427–433.
Laupacis, A., R. Bourne, C. Rorabeck, et al. "Comparison of Total Hip Arthroplasty Performed With and Without Cement: A Randomized Trial." Journal of Bone and Joint Surgery, American Volume 84-A (October 2002): 1823–1828.
Lie, S. A., L. B. Engesaeter, L. I. Havelin, et al. "Early Postoperative Mortality After 67,548 Total Hip Replacements: Causes of Death and Thromboprophylaxis in 68 Hospitals in Norway from 1987 to 1999." Acta Orthopaedica Scandinavica 73 (August 2002): 392–399.
Mantilla, C. B., T. T. Horlocker, D. R. Schroeder, et al. "Frequency of Myocardial Infarction, Pulmonary Embolism, Deep Venous Thrombosis, and Death Following Primary Hip or Knee Arthroplasty." Anesthesiology 96 (May 2002): 1140–1146.
Solomon, D. H., E. Losina, J. A. Baron, et al. "Contribution of Hospital Characteristics to the Volume-Outcome Relationship: Dislocation and Infection Following Total Hip Replacement Surgery." Arthritis and Rheumatism 46 (September 2002): 2436–2444.
White, R. H. and M. C. Henderson. "Risk Factors for Venous Thromboembolism After Total Hip and Knee Replacement Surgery." Current Opinion in Pulmonary Medicine 8 (September 2002): 365–371.
organizations
American Academy of Orthopaedic Surgeons (AAOS). 6300 North River Road, Rosemont, IL 60018. (847) 823-7186 or (800) 346-AAOS. http://www.aaos.org .
American Physical Therapy Association (APTA). 1111 North Fairfax Street, Alexandria, VA 22314. (703)684-APTA or (800) 999-2782. http://www.apta.org .
National Center for Complementary and Alternative Medicine (NCCAM) Clearinghouse. P.O. Box 7923, Gaithersburg, MD 20898. (888) 644-6226. TTY: (866) 464-3615. Fax: (866) 464-3616. http://www.nccam.nih.gov. .
National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) Information Clearinghouse. National Institutes of Health, 1 AMS Circle, Bethesda, MD 20892. (301) 495-4484. TTY: (301) 565-2966. http://www.niams.nih.gov .
Rush Arthritis and Orthopedics Institute. 1725 West Harrison Street, Suite 1055, Chicago, IL 60612. (312) 563-2420. http://www.rush.edu .
other
Hip Universe. June 15, 2003 [cited July 1, 2003]. http://www.hipuniverse.homestead.com .
Questions and Answers About Hip Replacement. Bethesda, MD: National Institutes of Health, 2001. NIH Publication No. 01-4907.
Rebecca Frey, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Hip replacement surgery is performed by an orthopedic surgeon, who is an MD and who has received advanced training in surgical treatment of disorders of the musculoskeletal system. As of 2003, qualification for this specialty in the United States requires a minimum of five years of training after medical school. Most orthopedic surgeons who perform joint replacements have had additional specialized training in these specific procedures. If surgery is being considered, it is a good idea to find out how many hip replacements the surgeon performs each year; those who perform 200 or more have had more opportunities to refine their technique.
Hip replacement surgery can be performed in a general hospital with a department of orthopaedic surgery, but is also performed in specialized clinics or institutes for joint disorders. As of 2002, MIS is performed in a small number of specialized facilities and teaching hospitals attached to major university medical schools.
QUESTIONS TO ASK THE DOCTOR
- What alternatives to hip replacement might work for me?
- Am I a candidate for minimally invasive surgery?
- How many hip replacement operations do you perform each year?
- How many patients have you treated with my specific condition have you treated?
- Does the hospital have preop patient groups that I can attend?
I was actually in the Orthopaedic Field and was on my way down the hall to a patient's room and collapsed. After quite an effort and excrusiating pain, I could not get up. We shot x-rays that afternoon and they blatanly showed that I had AVN with notable femural head collapse. Thereafter I had an MRI done of both hips which indicated that I had late stage 3 bi-laterally.
I had THR bi-laterally which seemed tohelp for a short time but within 5 months, I had to have revisions on both hips. Before a year had ended, I had to have 2 more revisions to each hip. After leaving the staples in for 10 days on both hips, the left hip and granulated quite well that the suture line looked well. However, after 30 minutes of removing the staples on my right hip, the incision line burst open. In a matter of 1.5 weeks the wound took on the classic smell of psuedomonus. At this time my temp. hit 106 with many episodes mental cloudiness.
After 3 months in the hospital, I was released only to developed a very high grade fever 8 days later and was told I would have to have aGirdle-Stone Procedure on my left side to save my life. Much to my dismay, I agreed. However, while attemptiong to remove the prosthesis, my femur shattered.
I take Methadone to help with chronic pain but over the years I have developed a toloerance and was wondering is THERE ANYTHING I CAN DO TO REVERSE THIS? I promise you that I am not a drug abuser, I just want to get back to being the best father I know how.
Any help you can provide I would be most appreciative.
thanks Ron
Thanks for taking the time to respond to my questions.
Cheryl
depuyhipimplantrecall .org
ago and had an orthotist fit me for shoes to compensate for the 4" difference in leg length.The
raised shoe is so very heavy it tires me out just walking around our small house. Anyone with
a similar experience and solution who reads this I would appreciate you contacting me please.
MY NAME IS VIBISH I AM FROM INDIA.MY LEG, HIP DAMEGED STAGE 3 .WALKING TIME TOOMUCH PAIN AND STRAIN,IN OPPARATION I DONT HAVE MONEY NOW AFTER 5 MONTHS BACK I NEED TO OPPARATEE THAT ONE.THEY ARE ASKING ONE AND HALF LAKS ,WHAT I WILL DO ANY EXERCISES OR ANY TABLETS NAME GIVE TO ME I NEED TO REALEASE THE LEG PAIN PLS GIVE ANY IDEA FOR ME .PLS
I had a Total hip replacement 6 july 2015 just 2 weeks ago,,they cut me in the front on my thigh and apparently had trouble getting through the muscle,,i woke up with the surgeon telling me that they had complications and a revision would be done in 4 days time and they needed to look at a hole that was drilled.
He told me they cut the bone and removed the ball at the top of the bone and inserted the new ceramic cup that the ball sits in.
Apparently the didn't have the tools to do a different procedure and I needed to wait 4 days in traction as the bone had been cut. I went under the knife the 4th day and the came from a different angle as they told me my muscle was like working on a rhino and prior to the new revision they called it,,i was Xrayed extensively,,CT scan and other Xrays to look for the hole they drilled and get it done right.
I feel ok at this point but I am doped up on Oxycodone,,,Targin,, and Endone all day and all night. My skin behind my neck stinks like Parmisan cheese and I am losing weight and feel great,, I shower 2 times a day and eat healthy. Does this operation sound like it was done right. Will the stink on my skin go away as im back at work in 4 weeks.
Steve Driver.
I have Bilateral AVN of femoral head type 3, used steroids for Asthma for a long time. Am on pain killers(etorix) and I walk with a limp for the last 9 months though I continue with my life as usual despite.
I am on Sodium alendonrate and zedcal (calcium supplement|) for the whole duration- i stopped taking Diacerin, Glucosamine and tramadol.
Am contemplating having bilateral hip replacement as am worried one day I will be wheel chair bound.
Can the condition reverse or stop advancing. Is the hip replacement a good Idea?
George
Thanks in advanced for answering my 2 questions
It can be also solved by using orthofeet Avery Island – Black shoes which reduces your pains and make you feel more comfortable. That’s why people are mostly orthofeet shoes it is not only providing shoes but also reducing the pain caused in legs to the people