Appendectomy
Definition
Appendectomy is the surgical removal of the appendix. The appendix is a worm-shaped hollow pouch attached to the cecum, the beginning of the large intestine.
Purpose
Appendectomies are performed to treat appendicitis, an inflamed and infected appendix.
Description
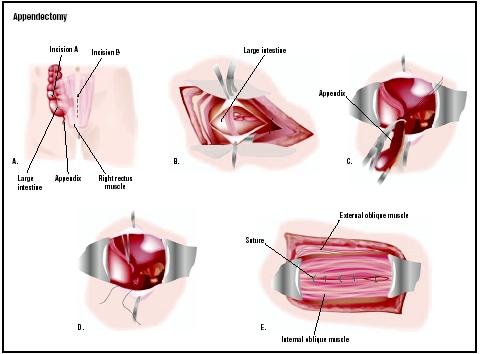
After the patient is anesthetized, the surgeon can remove the appendix either by using the traditional open procedure (in which a 2–3 in [5–7.6 cm] incision is made in the abdomen) or via laparoscopy (in which four 1-in [2.5-cm] incisions are made in the abdomen).
Traditional open appendectomy
When the surgeon uses the open approach, he makes an incision in the lower right section of the abdomen. Most incisions are less than 3 in (7.6 cm) in length. The surgeon then identifies all of the organs in the abdomen and examines them for other disease or abnormalities. The appendix is located and brought up into the wounds. The surgeon separates the appendix from all the surrounding tissue and its attachment to the cecum, and then removes it. The site where the appendix was previously attached, the cecum, is closed and returned to the abdomen. The muscle layers and then the skin are sewn together.
Laparoscopic appendectomy
When the surgeon performs a laparoscopic appendectomy, four incisions, each about 1 in (2.5 cm) in length, are made. One incision is near the umbilicus, or navel, and one is between the umbilicus and the pubis. Two other incisions are smaller and are on the right side of the lower abdomen. The surgeon then passes a camera and special instruments through these incisions. With the aid of this equipment, the surgeon visually examines the abdominal organs and identifies the appendix. The appendix is then freed from all of its attachments and removed. The place where the appendix was formerly attached, the cecum, is stitched. The appendix is removed through one of the incisions. The instruments are removed and then all of the incisions are closed.
Studies and opinions about the relative advantages and disadvantages of each method are divided. A skilled surgeon can perform either one of these procedures in less than one hour. However, laparoscopic appendectomy (LA) always takes longer than traditional appendectomy (TA). The increased time required to do a LA the greater the patient's exposure to anesthetics, which increases the risk of complications. The increased time requirement also increases the fees charged by the hospital for operating room time and by the anesthesiologist. Since LA also requires specialized equipment, the fees for its use also increase the hospital charges. Patients with either operation have similar pain medication needs, begin eating diets at comparable times, and stay in the hospital equivalent amounts of time. LA is of special benefit in women in whom the diagnosis is difficult and gynecological disease (such as endometriosis, pelvic inflammatory disease, ruptured ovarian follicles, ruptured ovarian cysts, and tubal pregnancies) may be the source of pain and not appendicitis. If LA is done in these patients, the pelvic organs can be more thoroughly examined and a definitive diagnosis made prior to removal of the appendix. Most surgeons select either TA or LA based on the individual needs and circumstances of the patient.
Insurance plans do cover the costs of appendectomy. Fees are charged independently by the hospital and the physicians. Hospital charges include fees for operating and recovery room use, diagnostic and laboratory testing, as well as the normal hospital room charges. Surgical fees vary from region to region and range between $250–750. The anesthesiologist's fee depends on the health of the patient and the length of the operation.
Preparation
Once the diagnosis of appendicitis is made and the decision has been made to perform an appendectomy, the patient undergoes the standard preparation for an operation. This usually takes only one to two hours and includes signing the operative consents, patient identification procedures, evaluation by the anesthesiologist, and moving the patient to the operating area of the hospital. Occasionally, if the patient has been ill for a prolonged period of time or has had protracted vomiting, a delay of few to several hours may be necessary to give the patient fluids and antibiotics .
Aftercare
Recovery from an appendectomy is similar to other operations. Patients are allowed to eat when the stomach and intestines begin to function again. Usually the first meal is a clear liquid diet—broth, juice, soda pop, and gelatin. If patients tolerate this meal, the next meal usually is a regular diet. Patients are asked to walk and resume their normal physical activities as soon as possible. If TA was done, work and physical education classes may be restricted for a full three weeks after the operation. If a LA was done, most patients are able to return to work and strenuous activity within one to three weeks after the operation.
Risks
Certain risks are present when any operation is performed under general anesthesia and the abdominal cavity is opened. Pneumonia and collapse of the small airways (atelectasis) often occurs. Patients who smoke are at a greater risk for developing these complications. Thrombophlebitis, or inflammation of the veins, is rare but can occur if the patient requires prolonged bed rest. Bleeding can occur but rarely is a blood transfusion required. Adhesions (abnormal connections to abdominal organs by thin fibrous tissue) are a known complication of any abdominal surgery such as appendectomy. These adhesions can lead to intestinal obstruction that prevents the normal flow of intestinal contents. Hernia is a complication of any incision. However, they are rarely seen after appendectomy because the abdominal wall is very strong in the area of the standard appendectomy incision.
The overall complication rate of appendectomy depends upon the status of the appendix at the time it is removed. If the appendix has not ruptured, the complication rate is only about 3%. However, if the appendix has ruptured, the complication rate rises to almost 59%. Wound infections do occur and are more common if the appendicitis was severe, far advanced, or ruptured. An abscess may also form in the abdomen as a complication of appendicitis.
Occasionally, an appendix will rupture prior to its removal, spilling its contents into the abdominal cavity. Peritonitis or a generalized infection in the abdomen will occur. Treatment of peritonitis as a result of a ruptured appendix includes removal of what remains of the appendix, insertion of drains (rubber tubes that promote the flow of infection inside the abdomen to outside of the body), and antibiotics. Fistula formation (an abnormal connection between the cecum and the skin) rarely occurs. It is only seen if the appendix has a broad attachment to the cecum and the appendicitis is far advanced, causing destruction of the cecum itself.
The complications associated with undiagnosed, misdiagnosised, or delayed diagnosis of appendicitis are very significant. This has led surgeons to perform an appendectomy any time that they feel appendicitis is the diagnosis. Most surgeons feel that in approximately 20% of their patients, a normal appendix will be removed. Rates much lower than this would seem to indicate that the diagnosis of appendicitis was being frequently missed.
Normal results
Most patients feel better immediately after an operation for appendicitis. Many patients are discharged from the hospital within 24 hours after the appendectomy. Others may require a longer stay, from three to five days. Almost all patients are back to their normal activities within three weeks.
Morbidity and mortality rates
The mortality rate of appendicitis has dramatically decreased over time. Currently, the mortality rate is estimated at one to two per 1,000,000 cases of appendicitis. Death is usually due to peritonitis, intra abdominal abscess, or severe infection following rupture.
Alternatives
Appendectomies are usually carried out on an emergency basis to treat appendicitis. There are no alternatives, due to the serious consequence of not removing the inflamed appendix, which is a ruptured appendix and peritonitis, a life-threatening emergency.
See also Laparoscopy .
Resources
books
Schwartz, Seymour I. "Appendix." In Principles of Surgery, edited by Seymour Schwartz, et al. New York: McGraw-Hill, 1994.
Silen, William. "Acute Appendicitis." In Harrison's Principles of Internal Medicine , edited by Anthony S. Fauci, et al. New York: McGraw-Hill, 1997.
periodicals
Eypasch, E., S. Sauerland, R. Lefering, and E. A. Neugebauer. "Laparoscopic versus Open Appendectomy: Between Evidence and Common Sense." Digestive Surgery 19 (2002): 518–522.
Peiser, J. G. and D. Greenberg. "Laparoscopic versus open appendectomy: results of a retrospective comparison in an Israeli hospital." Israel Medical Association Journal 4 (February, 2002): 91–94.
Piskun, G., D. Kozik, S. Rajpal, G. Shaftan, and R. Fogler. "Comparison of laparoscopic, open, and converted appendectomy for perforated appendicitis." Surgery and Endoscopy 15 (July 2001): 660–662.
Long, K. H., M. P. Bannon, S. P. Zietlow, E. R. Helgeson, et al. "A prospective randomized comparison of laparoscopic appendectomy with open appendectomy: Clinical and economic analyses." Pathology Case Reviews 129 (April, 2001): 390–400.
Selby, W. S., S. Griffin, N. Abraham, and M. J. Solomon. "Appendectomy protects against the development of ulcerative colitis but does not affect its course." American Journal of Gastroenterology 97 (November, 2002): 2834–2838.
organizations
American College of Surgeons. 633 N. Saint Clair St., Chicago, IL 60611-3211. (312) 202-5000. http://www.facs.org .
other
"Appendectomy." MEDPLINE PLUS. [cited June 27, 2003]. http://www.nlm.nih.gov/medlineplus .
"The Appendix." Mayo Clinic Online. http://www.mayo health.org .
Mary Jeanne Krob, M.D., F.A.C.S.
Monique Laberge, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
An appendectomy is performed by a fully trained surgeon who, after medical school, has gone through years of training in an accredited residency program to learn the specialized skills of a surgeon. A sign of a surgeon's competence is certification by a national surgical board approved by the American Board of Medical Specialties (ABMS). All board-certified surgeons have completed an approved training program and have passed a rigorous specialty examination. The letters F.A.C.S. (Fellow of the American College of Surgeons) after a surgeon's name are a further indication of a surgeon's qualifications.
Appendectomy is considered a major surgical operation. Therefore, the surgeon must perform this operation in the operating room of a hospital. An anesthesiologist is also present during the operation to administer an anesthetic.
QUESTIONS TO ASK THE DOCTOR
- What are the possible risks involved with this surgery?
- What are the expected results after having a laparoscopic appendectomy versus having an open abdominal appendectomy?
- Will I have a scar?
- Which procedure will you use to perform the appendectomy?
- Must I do anything special after the operation?
- How long does it take to recover?
- How many appendectomies do you perform each year?
I had laparoscopic appendectomy done about a week ago. I was told I could shower 1 day after leaving the hospital, so 48 hours after my surgery.
Yesterday took my small bandages off and was amazed about the size of the scars! SO SMALL :D I expected much bigger but because I had the laparoscopic appendectomy, there's only 3 X 3/4 inch scars and I bet they'll heal into almost nothing. My advice, if scarring is an issue for you, definitely have a LA done.
Mine was very routine and a very smooth procedure. They even had me on solid foods for breakfast.
I should have 3 very tiny scars. One of mine will also be on the left which surprised me also.
i was wondering if anyone knew when i could have a cigarette or if there is anytime limit on when i could do so.
please let me know!
thank you.
The only thing I would question in this article is the cost. My bill was over $18,000 (billed to insurance, who knows what I'll have to pay). Granted, that includes the Emergency Room, the CT scan, my overnight hospital stay (since the surgery was at 10pm) etc. But just the surgery was over $6,000 of that. I'm in the Pacific NW. Maybe it's more expensive here?
I'm back to work (desk job) after a week off. As with any abdominal surgery, it was very painful for a few days till the muscles start to heal again. Taking it easy on housework and not lifting anything heavy. I feel a little soreness on the incisions now and again but everything seems to be healing well.
My work have told me that I will be fired unless I return today - Nov 23rd. Surgeon faxed my workplace advising 2 weeks off work. I'm in an at will state and have no access to FMLA, am I screwed?
Anyway, it was done via LA, I was meant to be discharged at 10am on Friday, a mere 11 hours after leaving the surgery! But due to the pain in my shoulders from the air being pumped in to me, I had to stay a few extra hours.
I'm taking Lortab, I'm trying to get around and get mobile but it always puts me in uncomfortable pain around the incision area at night and first thing in the morning.
My right shoulder bothered me a little bit and I knew that was from the CO2 they fill your abdomen with- pretty normal. I did take some Miralax on Friday and a dose on Saturday as I was nervous about having a soft bowel movement. Worked great and had no pain when I finally had a bowel movement Sunday evening.
My husband is a respiratory therapist so here is a great tip for coughing. Take a towel and roll it up, when you have to cough, press the towel to your abdomen firmly before coughing- this helps immensely. I was told that I shouldn't drive (not using Percocet anymore) because it is an abdominal surgery. I thought that statement was ridiculous so I drove to the store (about 5 miles)for a few things. I live in Minnesota and we just got 5 inches of snow- it was a little slippery and I found myself riding the brake, needless to say my abdomen was pretty sore after I got home. I understand why I shouldn't have been driving- back to taking a Percocet tonight. Is anyone have a stinging sensation at one or more of there incision sites? I think that is what bugs me the most.
Nov.27th wonderful "bowel prep" = no food and laxatives all night long.
Nov.28th Endoscope and Colonscopy. Due to having severe stomach cramping and diarrhea. Checking for all gastro issues on both ends of the spectrum.
Nov.29th scope results = ALL NORMAL!
Nov.29th evening before midnight SEVERE stomach pain went to emergency room.
Nov.30th (6:30am) appendicitis surgery scheduled for removal,(5;45pm! various docs,various pain meds, no food)
Apparently my appendix was such a mess it was hard like a woody pulp from ongoing leaking! Nasty
Dec. 1 - Overnighted in hospital, discharged at 4:30pm. Ride home advice!!! Have whomever is picking you up from hospital to bring pillow so you can lean car seat back,place pillow over belly, then seat on. Percocets was the pain pill prescribed to me. Stay on top of taking your pain pills! Never think , hey I'm feeling fine, I don't need them and fall behind on your pain control. Not fun.
Something that has not been mentioned yet in all feedback that I think all should know...
Pain killers from hospital and whatever you are taking at home will cause CONSTIPATION. Your abdomen is sore to begin with, trying to go #2 is a sore/painful experience. Just eat soups or something easy to pass. It feels really odd having a bowel movement also.Best way to put it. You know when you are going to have pain before it happens and the same with relief.
Taking a shower, be careful not to take a overly hot shower, due to lack of food on your stomach combined with pain meds makes it VERY easy to get dizzy and passout.
Dec.5th Due to boredom and frustration of felling useless, I went to post office and got haircut.
SPEEDBUMPS SUCK! Driving the bumps are painful. Obviously I'm not going to take pain meds and drive. After cut I was ready to go home. EXHAUSTED! I ate some, showered, pain med, and went to bed feeling like I climbed Mt.Everest.
Last advice, don't rush into doing stuff and don't lift anything to heavy. Doc told me nothing heavier than a gallon of milk for a week.
Goodluck anyone/everyone and I hope this helped.
At 4:45 pm I went into preop and then surgery shortly after. They did the laparoscopic surgery. It is now day 5 and I am still in some pain, not as intense as the first 3 days after surgery, but very intense at times. Stnading for a long period of time is not optionable at this time as it puts too much pressure on the area where the appendix was. I suppose it's from everything settling into place. The right shoulder pain has not completely gone, depending on how I lay or sit, and the belly button incision is still draining. The i.v. in my hand caused my vein to swell and harden. I am also extremely nauseous and having no easy time with bowel movements-they are painful, again from the pressure I assume-and I immediately have to sit down for a long amount of time. I have showered and change my bandaids every two days. The only one that really needs it is the belly button incision. All three incision sites are slightly raised and hard, not sure if this is normal but intend to inquire about it at my follow up on this coming Friday Dec. 17, 10.
Hopefully this helps if anyone has anything similar with their appendectomy experience.
PLEASE do read. For many years (although very active and fit) I had had many peculiar problems with my stomach and hips - aches and pains. Of course in my mind - I'm thinking it must be because of a riding accident I had - or maybe after having my children. All sorts of things - and then suddenly - bang - I had breast cancer - I was very lucky - and because I went to the hospital very quickly I was treated with cemo therapy and radio therapy and did not have to have my breast removed as the tumer disappeared immediately after my first cemo. However, for some reason and I don't know wether it was the cemo - radio - or drugs - I was at last free of PAIN.
You see - I had got so used to pain in my left hip and leg area - it had become the norm. Little did I know - but all those aches and pains - were most probably grumbling apendix all those years - but because I thought I new what it was and because I had not been treated seriously by the doctors and specialists - because I always present myself as O.K. this had been missed, so that suddenly although NOT in pain - I became ill - in that I did not want to eat - I had a very high temperature - I was very tired - which was not unusual because of the cancer treatments - I just thought that I had picked up a bug of some sort. However - things did get
a little worse - so we called the doctor - who on examination - discovered that I was rather dehydrated - and so suggested some sort of medication - or in order to deal with this quickly -
I could go into hospital and be put on a drip - I decided to go for this option - because I remembered being dehydrated before with the cancer treatments and it wasn't very pleasant. On being taken into hospital - I found myself in a hospital bed (by the way the visiting doctor did mention that he thought it could possibly be appendicitis). The following afternoon and after having to go to the toilet I don't know how many times - I had a scan - which certified that it was indeed apendicitis. That evening at about 10.15p.m. or so I was taken into theatre where I had my opertion - only by this time - my apendicitis had unfortunately turned into peritonitis. This meant that I nearly lost my life and had to have a very large incision causing me to at a later date have more surgery (incisional hernia) which has left me with very unsightly scaring and unfortunately the hernia has come back again - so the reason I write this is to say - DO Not be fobbed off - get yourself or whoever properly examined and get the problem sorted as soon as possible - O.K. Thanks for taking the time.
Its now Sunday, and I haven't had a bowl movement. I have had gas, but I feel worried that I should be going to the bathroom. Can someone please tell me when I should start/ should have been going?
I underwent appendix open surgery, after surgery 17 units of blood transfused and lot of antibiotics were given given bcoz of this two my kidney functions elevated to peak. After Two blood dialisis only i came to normal.
After surgey the surgery wound heals took 7 months. After the surgery spot become Herinia and the doctor says it needs to be removed, otherwise it will become more complicated.
can u advise me the best solution for this.
Regards,
Jayaprakash
Thank you so much
Beth new york
Thank you so much
Beth new york
I was dismissed from the hospital one hour after surgery.
The next day, I was in a lot of pain, mostly from the CO2 in my body. My right shoulder was in severe pain.
Days two and three were also painful, and I was also nauseated. I stopped taking hydrocodone on day 3.
Day 4-7 have been much better. I'm sleeping well and have no more pain in my shoulders.
I took the bandages off of my incisions on Day 6 and the wounds look great- very small and almost closed up.
I still have some pain near my belly button area (the largest incision), but I expect that to go away in a few days.
IS THIS NORMAL?
can any one suggest ways to minimize the pain when coughing.
A day later I was back and I was in more pain than before. More tests and scans were done and still they all came back clear. The surgeons had no answers for me so they decided to do surgery to take a look and while they were there they were going to remove my appendix whether it was inflamed or not because they said it is useless.
The plan was for a laparoscopic surgery but they ended up making a last second decision to do an open surgery because they said something about how my belly peircing makes it easier for bacteria to get trapped in the belly button and they were worried that it would cause a greater risk of infection if they went through there. It turns out that my appendix was extremely swollen and had a large amount of pus that they said it could have burst at any time. They kept me in hospital for a couple of days later because the appendicitis was so bad.
And the sonographers prepared some kind of final report saying that after a second look at the ultrasound they can see that the appendix did look somewhat suspicious.
My incisions were just below the belly button, the centre of the lower pelvis and centre left side. They form a near perfect quadrilateral triangle so at least my scars (if any) will be symmetrical.
I am itching but to be honest I think it's a sign of healing.
I couldn't eat full meals but after a couple of days I was back to my normal habits again and eating fine.
I have been given 2 weeks off work which is fair and I am going to take to let the sore feeling and the back aches go away. I will be back to normal working life then.
And they all lived happily ever after. The End.
My incisions were just below the belly button, the centre of the lower pelvis and centre left side. They form a near perfect quadrilateral triangle so at least my scars (if any) will be symmetrical.
I am itching but to be honest I think it's a sign of healing.
I couldn't eat full meals but after a couple of days I was back to my normal habits again and eating fine.
I have been given 2 weeks off work which is fair and I am going to take to let the sore feeling and the back aches go away. I will be back to normal working life then.
And they all lived happily ever after. The End.
My appendectomy went great. I had been experiencing abdominal pains since about 2 pm on Wednesday, and by the time I went to bed I knew something was odd. The pain persisted all night, I figured OK, this isn't gas, and walked five blocks to my local hospital at 6 a.m. Thursday. They did a CT scan by 9:30, and at 10 am the surgeon told me I wouldn't be leaving that day. They did a laparoscopic procedure around 2:30, and by 5 I was in a hospital and feeling so well I wanted to go home that night. They kept me overnight for observation, but I was discharged at 9 am on Friday and walked the five blocks back home.
I did have pain in my neck and shoulders that weekend from the gas, and the surgery aggravated some pre-existing back pain I've had for years. But I was driving by Sunday, went back to work on Monday, and still haven't even filled the prescription for my pain meds. Very happy with the results all around.
If the abdominal pain persisted,especially on my right side,go to the ER,he recommended.
The next day the pain was all on my right side of my abdomen. Drove myself to the ER. After blood tests and a CAT Scan, I was told that my appendix had ruptured. Not a full blown explosion, more of a small leak.
I had an appendectomy about 12 hours after I had checked in. I had a massive antibiotic treatment. Spent a week in the hospital. Had two drains to remove fluids from the sugery site.
I go back to work on Nov. 7. Until then no lifting anything over 10 lbs. No stressing my abdominal muscles. I lost about 10-15 lbs. Didn't eat much in the hospital. Was on liquid diet most of the time.
Still have some tenderness,but it gets better with each passing week.
Has anyone else out there experiencing anything like this? I don't think my appendix needed removing. The doctor put in my medical records that he came outside of the operating room and asked my husband for permission to remove my appendix. My husband had never met, seen, talked to or given permission to this doctor ever. After surgery I had complications and there was no doctor on call while this doctor was on vacation. I could not find anyone to touch me. I ended up in the emergency room in another town.
Its around 5inc long and i have a strange lump above it as the scar dints into my body
Does any one now if i could have sorted out as i am just worried that it may be connected to a muscle in the stomach and later in life i mite have problems when having children as it pulls really bad when i exercise or stretch my stomach in any way.
Please if you have any information about about let me no
Thanks
thank u
I was In the ER. I had the larenscopic procedure. Went well. I left the hospital about 16 hours later.
My first week was painful. I did walk and move around and as for lifting anything like laundry..dont
Do anything over 10 pounds and wait atleast a couple days before you attempt to. Sitting down and getting up
Still is a little painful but it is a little better. Any smokers I would suggest no smoking or drinking for the first week and a half to two weeks. Smoking can very much increase the risk of pneumonia which can be really bad.
Other tips is drink a liter bottle of gatorade a day for a few days after surgery. There are electrolytes I. Gatorade that will help recovery and its a good thing for hydration. No sodas or carbonated drinks cuz the carbonation will make you gassy and a bit painful. No tight clothing...uhn.. Im trying to think of any other tips that cohld be helpful...oh..it is normal to have the following: a uti...loose stool the first 3-4 days after surgery..a LITTLE bit of blood in the stool or a yeast infection during recovery. It can happen so just get antibiotics for it and dont stress too much. And before surgery you can always get the surgeons name and look them up and do some research on them. I did with mine! Dont be afraid to do so. :-)
Im 29, healthy, I had LA done few days ago and I was in and out the ER in 2 and half hours, lol but the 5 hours i had before they started was no joke. Yea pretty amazing recovery for how much pain I was in (kicking and almost screaming), thank you Kaiser. They printed out all the info I needed to read at home and more on their website. Follow up appointment 1-2 weeks later.
No work for a week, said normal eating habits after were fine, but I stuck to soups for the past days and loaded up on electrolytes and water. Screw the pain meds (had norco) gave me a bad headache, little diarrhea and constipation (did not take stool softener) but really didn't have bad pain that needed norco. Experience normal pain and weakness, nothing alarming. Walking longer distance on 3rd day seem fine but still walking hunched like an old man. Lifting after 4-6 weeks but remember doc saying nothing strenuous for a YEAR? No idea, I was in pain when he told me but thankfully I have a follow up appointment to ask questions. If they cut the abdominal wall, it probably won't heal in a month, you risk a Hernia, but a year is long as hell.
Incisions were on the left also, but geez, watch a video how the operation works, it's normal.
Geez, do yourselves a favor and call a nurse or doctor if u have questions. Good luck.
Later, When the throat tube was being removed after the surgery, I was unable to breath. As a result,I developed severe Pulmonary Edema. Extremely scary and very dangerous. I am a teenage. Malpractice?
Three months ago i had a lower right abdominal pain & doctors had my appendix removed by open surgery. Now i experience pains at same, what could be the cause of d post appendicetomy pain?
The doc came in and said I had a gangrenous appendix but luckily it had not ruptured. By 2 pm I was home and have been taking it easy. I have Percocet but have taken it only a couple of times. The pain is there, but nothing like before surgery. It hurts when I move around and I am walking pretty slow. I am going to take ibuprofen today and save the Percocet for nighttime. I think I might live!!! I see the doc in 2 weeks for a follow up. Hang in there everybody. The pain of an appendicitis is crazy, but it does get better.
A pillow across the abdomen will help ease the pain when coughing, sneezing, laughing or just standing up. Pain in shoulders, under ribs, etc., is most likely from the gas they use to inflate the abdomen during laparoscopic surgery. I had a bubble stuck under my ribs and another under my clavicle that did not want to move. The nurse at my doctor's office told me walking was the best medicine but also OTC gas relief medicine seems to help ease it even though it's not the same kind of gas. I have a treadmill and would make myself walk 3-5 mins at a time (commercial breaks are great for this!), walk to the mailbox and back, around the backyard, etc. As soon as I could drive, I enjoyed going to Walmart to walk around using a shopping cart as a walker.
Recovery can be slow but moving as much as possible (NOT over exertion) and sufficient rest are the keys! If you work full-time, start weaning yourself off those wonderful afternoon naps about a week before your return and try to get back on a regular work day schedule. I was out of work for 6 weeks and was able to make it through full-time days when I returned but was exhausted and achy by the time I got home. Just be patient and take it slower than you think you need to!
Everybody has their own time table. I was one of the more severe cases. I occasionally still have mild pain caused by abdominal adhesions from peritonitis and the surgery itself. My nephew had a little better experience -- no rupture, out of hospital 24 hrs after surgery, 2 1/2 weeks out of college. My brother was even luckier -- no rupture, surgery Thurs, home Fri, back to work on Mon with NO pain meds and NO further issues!! So there you have it, my family's experience ranges from one extreme to the other. The experiences of most others I know have been similar to my nephew's.
Get well soon!
what can I do ?
So I have my appendix removed 7 weeks ago and it was preety bad, a week after the operation I got a drain due to the infection.
My question is: now at 7 weeks after why do I feel like a balloon at my belly and passing a lot of gas and starts to hurt when i Press on my belly? ðŸ˜
Thank you very much
The operation went well, I was able to eat a normal breakfast the next morning, and was discharged at lunchtime 18 hours after the surgery. I am tender, but that is expected.
Apparently the misdiagnosis was due to my pain appearing higher in the abdominal, it is common for the pain to drop over time.
I have cancelled the horseriding adventure I had planned for the weekend, but hope I can get back into yoga in the next couple of weeks. The doctor's advice is to return to exercise if you feel up to it physically.
I still in alot of pain and my incisions still bleed a little. I haven't been able to go to the toilet at all and it really hurts to pee! Should I see a doctor or is this all normal?
Thank you.
i share some information now, in my case, pain started at 10am on wednesday, identically to an indigestion, pain increased as the time passes and focused on my lower right side, it felt like there was a heavy bag in that area and was difficult to pee, didnt want to poop but I felt if i pushed the bag would explode, i had some headache, and felt better laying down, even on my side that sitting or standing, my pulse accelerated but in thursday evening, never had fever, had appetite, the doctor told me to do sth that hurt like hell, stand on my tiptoes and then fall with the feet, also on thursday evening before the operation my abdomen was rigid to touch, i mean due to the pain my abdomen didnt want to be touched and muscles were tensed, i had a high amount of white cells and well that's all i guess
CT scan I had 3 days prior showed nothing until the hospital doctors requested the images. One hour later, I had Lapro surgery. 5 days in with a drain and NG tube. Took about 4 weeks to get back to my normal self again. I'm a tough old Vietnam vet but, this almost did me in. Most everyone will be fine. Make sure to get a colonoscopy in 6 weeks in case something else caused it. Good luck.
Unfortunately, the doctor found the appendix was normal. He checked for mesenteric adenitis,salpingitis etc
My question is that; regardless to other affected organs, the appendectomy has to be done or not though the appendix was normal?
If the appendectomy has to be conducted why? And if not why ?
I'm a medical student, future doctor by the grace of God, i need your assistance.
Thank you