Aortic valve replacement
Definition
Aortic valve replacement is the insertion of a mechanical or tissue valve in place of the diseased native aortic valve.
Purpose
Aortic valve replacement is necessary when the aortic valve has become diseased. The aortic valve can suffer from insufficiency (inability to perform adequately) or stenosis. An insufficient valve is leaky and allows blood flow retrograde from the aorta to the left ventricle during diastole. A stenotic valve prevents the flow of blood antegrade from the left ventricle to the aorta, during systole.
Either situation can result in heart failure and an enlarged left ventricle. With aortic stenosis (narrowing), angina pectoris, fainting, and congestive heart failure will develop with the severity of the narrowing. There is an increased rate of sudden death of patients with aortic stenosis. Dyspnea (labored breathing), fatigue, and palpitations are late symptoms of aortic insufficiency. Angina pectoris is associated with the latest stages of aortic insufficiency.
Demographics
Congenital birth defects involving a bicuspid aortic valve can develop stenosis. These patients may become symptomatic in mid-teen years through age 65. Patients with a history rheumatic fever have a disposition for aortic stenosis, but may live symptom free for more then four decades. Calcification of the aortic valve tends to effect an older population with 30% of patients over age 85 having stenosis at autopsy.
Patients with aortic stenosis who have angina, dyspnea, or fainting are candidates for aortic valve replacement. Asymptomatic patients undergoing coronary artery bypass grafting should be treated with aortic valve replacement, but otherwise are not candidates for preventive aortic valve replacement.
Patients with a history of rheumatic fever or syphilitic aortitis (inflammation of the aorta) face the possibility of developing aortic insufficiency. Successful treatment has decreased this causative relationship. Primary causes of aortic disease commonly include bacterial endocarditis, trauma, aortic dissection, and congenital diseases.
Patients showing acute symptoms, including pulmonary edema, heart rhythm problems, or circulatory collapse, are candidates for aortic valve replacement. Chronic pathologies are recommended for surgery when patients appear symptomatic, demonstrating angina and dyspnea. Asymptomatic patients must be monitored for heart dysfunction. Left ventricular dimensions greater then 2 in (50 mm) at diastole or 3 in (70 mm) at systole are indications for replacement when aortic insufficiency is diagnosed.
Description
While receiving general anesthesia in preparation for the surgery, the patient's cardiac function will be monitored. A sternotomy (incision in the sternum) or thoracotomy may be used to expose the heart, with the thoracotomy providing a smaller incision through the ribs. Anticoagulant is administered in preparation for cardiopulmonary bypass. Cardiopulmonary bypass is instituted by exposing and cannulating (putting tubes in) the great blood vessels of the heart, or by cannulating the
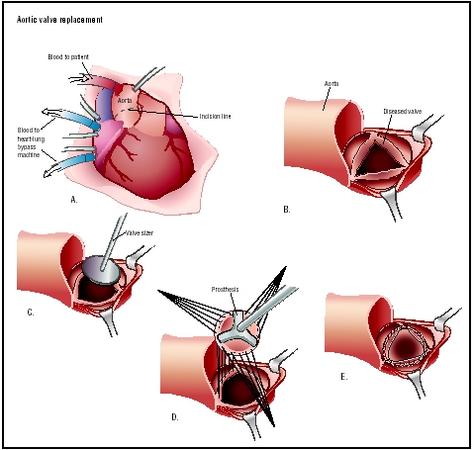
femoral artery and vein. A combination of cannulation sites may also be used. The heart is stopped after the aorta is clamped. The aortic root is opened and the diseased valve is removed. Sutures are placed in the aortic rim and into the replacement valve. The replacement valve can be either mechanical or biological tissue. The replacement valve will be sized prior to implant to ensure that it fits the patient based on the size of the aortic valve annulus. Once seated, the valve is secured by tying the individual sutures. The heart is then deaired. The cross clamp is removed and the heart is allowed to beat as deairing continues by manipulation of the left ventricle. Cardiopulmonary bypass is terminated, the tubes are removed and drugs to reverse anticoagulation are administered.
A heart valve is an orifice that blood passes through in systole, and it is also an occluding (blocking) mechanism necessary to prevent the flow of blood during diastole. Heart valves can be mechanical or biological tissue valves. For patients younger then 65 years of age, the mechanical valve offers superior longevity. Anticoagulation is required for the life of the patient implanted with a mechanical valve. The biological tissue valve does not require anticoagulation but suffers from deterioration, leading to reoperation particularly in those under age 50. Women considering bearing children should be treated with biological tissue valves as the anticoagulant of choice with mechanical valves, warfarin, is associated with teterogenic effects in the fetus. Aspirin can be substituted in certain circumstances.
Diagnosis/Preparation
Initial diagnosis by auscultation (listening) is done with a stethoscope . Additional procedures associated with diagnosis to judge severity of the lesion include chest x ray , echocardiography , and angiography with cardiac catheterization . In the absence of angiography, magnetic resonance imaging (MRI) or computed tomographic (CT) imaging may be used.
Aftercare
The patient will have continuous cardiac monitoring performed in the intensive care unit (ICU) postoperatively. Medications or mechanical circulatory assist may be instituted during the surgery or postoperatively to help the heart provide the necessary cardiac output to sustain the pulmonary and systemic circulations. These will be discontinued as cardiac function improves. As the patient is able to breathe without assistance, ventilatory support will be discontinued. Drainage tubes allow blood to be collected from the chest cavity during healing and are removed as blood flow decreases. Prophylaxis antibiotics are given. Anticoagulation (warfarin, aspirin, or a combination) therapy is instituted and continued for patients who have received a mechanical valve. The ICU stay is approximately three days with a final hospital discharge occurring within a week after the procedure.
The patient receive wound care instructions prior to leaving the hospital. The instructions include how to recognize such adverse conditions as infection or valve malfunction, contact information for the surgeon, and guidelines on when to return to the emergency room.
Risks
There are unassociated risks with general anesthetic and cardiopulmonary bypass. Risks associated with aortic valve replacement include embolism, bleeding, and operative valvular endocarditis. Hemolysis is associated with certain types of mechanical valves, but is not a contraindication for implantation.
Normal results
Myocardial function typically improves rapidly, with decrease in left ventricle enlargement and dilation over several months, allowing the heart to return to normal dimensions. Anticoagulation therapy will be continued to elevate the INR to between 2.0 and 4.5, depending on the type of mechanical valve implanted. Implantation of biological tissue valves with maintenance of an INR of 2.0–3.0 for the initial three months post implant are associated with blood clot complications. If non-cardiac surgery or dental care is needed the antithrombotic therapy will be adjusted to prevent bleeding complications.
Morbidity and mortality rates
There is a 3–5% hospital mortality associated with aortic valve replacement. There is an average survival rate of five years in 85% of patients suffering from aortic stenosis that undergo aortic valve replacement. Structural valve deterioration can occur and is higher in mechanical valves during the first five years; however, biological tissue and mechanical valves have the same failure incidence at 10 years, with a 60% probability of death at 11 years as a result of a valve-related complications. Patients with a mechanical valve are more likely to experience bleeding complications. Reoperation is more likely for patients treated with a biological tissue valve, but not significantly different when compared to their mechanical valve counterparts. This combines to an average rate of significant complications of 2–3% per year, with death rate of approximately 1% per year associated directly with the prosthesis.
Alternatives
Balloon valvotomy may provide short term relief of aortic stenosis, but is considered palliative until valve replacement can be accomplished. Aortic valve repair by direct commisurotimy may also be successful for some cases of aortic stenosis. Medical treatment for inoperable patients with severe aortic stenosis is used to relive pulmonary congestion and prevent atrial fibrillation.
Severe aortic insufficiency can be treated with medical therapy. Pharmaceuticals to decrease blood pressure, with diuretics and vasodilators, are helpful in patients with aortic insufficiency.
Resources
books
Hensley, Frederick A., Donald E. Martin, and Glenn P. Gravlee, eds. A Practical Approach to Cardiac Anesthesia. 3rd Edition. Philadelphia: Lippincott Williams & Wilkins Philadelphia, 2003.
periodicals
Bonow R, et al. "ACC/AHA Guidelines for the Management of Patients with Valvular Heart Disease." JACC 32 (November 1998): 1486–588.
Allison Joan Spiwak, MSBME
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Hospitals with cardiac surgery services provide aortic valve replacement. Specialization is required for young adults and pediatric patients. Cardiovascular and cardiac surgeons are trained to provide this treatment and the initial follow-up care. These surgeons are trained in their cardiac surgical residency to evaluate and perform these procedures and to care for the patient during the post-operative period.
QUESTIONS TO ASK THE DOCTOR
- What type of valve is best suited for me?
- What are the pros and cons associated with each type of valve for a person with my disease and/or associated diseases?
- Why am I a candidate for valve replacement?
- Are there any other more suitable alternative procedures?
- If I am a female interested in having children, or currently pregnant are there additional options?
- How often has the surgeon performed this procedure and what are the morbidity/mortality statistics for this surgeon and institution?
- If I have an associated disease or complicated scenario does the surgeon have experience with follow-up care?
In my case I new that I might need the operation for many years,(I had heart surgery when I was 14 years old)so in many ways it was a relief to get it over with.
Una.
i would like to thank who ever created this website.
Read more: Aortic Valve Replacement - procedure, blood, complications, adults, infection, heart, types, children, rate, Definition, Purpose, Demographics, Description, Diagnosis/Preparation, Aftercare, Risks, Normal results http://www.surgeryencyclopedia.com/A-Ce/Aortic-Valve-Replacement.html#ixzz0oCuQn2vN
Thanks,
Lenny
Could this been prevented ? especially when the cut down it was noted by the surgeon that there was some disease in the right femoral artery, shouldnt the surgeon used the left groin instead? Isnt it up to the perfusionist to watch that area ? did the surgeon take too long and why did he try to recannulate in the same vien when it was deflated? I hope you can help me understand why this happen ? thank you Julia
What does it mean when the doctor said we need to clean the blood of a patient in ICU currently using an artificial heart?
This is some one I know but not close to only by marriage. But I just want to know what is it. I am an RN in geriatric medical ward.
Some family members are against the surgery, and there concerns are:
1. Suffering during post operational period, and how long it will be
2. After surgery her quality of life will not change, and the risks she faces with aorta labled 'severe' will remain even after the surgery.
Are the concerns of those opposing surgery valid ?
day after operation her heart stopped and was revived within minutes with CPR.
Two days later a standard (non-defib) Pace Maker was implanted.
Question: does anyone know where I can get info regarding frequency of such a scenario,
and statistical outlook.
thank you.
She hasn't been seen by cardiologist yet! But can anyone tell me what this means for her.
Before the surgery we were told that there was a 98% chance of survival the extra 2% related to human error. My mother fell into the 2% category.
The hospital and their staff could not give us an explanation as to WHy this happened. It took three attempts and contacting getting an attorney involved before the hospital provided us with the Autopsy. Needless to say it was like pulling teeth to even get the actual medical reports. On three different attempts we have received three different sets of records even though we requested ALL documents for her. So choose your doctor carefully one 2mm mistake by them could cost you your life.
I was also told her condition could be inherited genetics. That knowledge concerns me because if I happened to inherit these genetics then I do not know if I will be able to move forward with this procedure if I need it because of this surgeons 2mm mistake with my mother.
Thanks, Henry Chavez
Sent to ER by cardiologist and admitted. New test, new echos, new EKGs. They called in I.D. doctor, who put him on antibiotics I.V. Pain starts to subside and he is dismissed.
Now, after 2 great weeks at home, shortness of breath is back, and the pain is back. Tylenol does not even touch the pain. Blood pressure is fine, but heart rate is high.
Cardiologist suggests the E.R. again, but he refuses to go back. Any advice? ?
For the last several yrs she has been widowed now, and she lives close to my brother and each night her heart would pound and her blood pressure would be too high and she would call my brother and the ambulance. Any time she would wait it out my brother would come over to sit with her. This went on constantly. One night she finally couldn't take being alone anymore and she drive herself to my brothers house at 3:00am and told him she could no longer live alone. He took her in and they sold her home and she has talked about her heart valve running out of warranty almost daily for a couple of years I guess. She is falling each time she gets on her feet now. She cannot hold herself up and wets her pants. She cannot tend to her briskness anymore, she forgets everything and when she talks she says strange things. We can not take care of her 24/7 and my brother will take her to the dr st 2:00 pm to get her into a facility and hospital for testing. They sat there in the waiting room emergency room for 6 hrs already and she couldn't sit any longer with her bad back. She is in terrible shape and seems to be in another world already. Has anyone of you lost someone from a failing heart valve? Pigs only live 15 yrs is what I read. Someone please help me. I believe this may be happening. Please share your knowledge with me about symptoms before death. Please. Thank you.
For the last several yrs she has been widowed now, and she lives close to my brother and each night her heart would pound and her blood pressure would be too high and she would call my brother and the ambulance. Any time she would wait it out my brother would come over to sit with her. This went on constantly. One night she finally couldn't take being alone anymore and she drive herself to my brothers house at 3:00am and told him she could no longer live alone. He took her in and they sold her home and she has talked about her heart valve running out of warranty almost daily for a couple of years I guess. She is falling each time she gets on her feet now. She cannot hold herself up and wets her pants. She cannot tend to her briskness anymore, she forgets everything and when she talks she says strange things. We can not take care of her 24/7 and my brother will take her to the dr st 2:00 pm to get her into a facility and hospital for testing. They sat there in the waiting room emergency room for 6 hrs already and she couldn't sit any longer with her bad back. She is in terrible shape and seems to be in another world already. Has anyone of you lost someone from a failing heart valve? Pigs only live 15 yrs is what I read. Someone please help me. I believe this may be happening. Please share your knowledge with me about symptoms before death. Please. Thank you.
For the last several yrs she has been widowed now, and she lives close to my brother and each night her heart would pound and her blood pressure would be too high and she would call my brother and the ambulance. Any time she would wait it out my brother would come over to sit with her. This went on constantly. One night she finally couldn't take being alone anymore and she drive herself to my brothers house at 3:00am and told him she could no longer live alone. He took her in and they sold her home and she has talked about her heart valve running out of warranty almost daily for a couple of years I guess. She is falling each time she gets on her feet now. She cannot hold herself up and wets her pants. She cannot tend to her briskness anymore, she forgets everything and when she talks she says strange things. We can not take care of her 24/7 and my brother will take her to the dr st 2:00 pm to get her into a facility and hospital for testing. They sat there in the waiting room emergency room for 6 hrs already and she couldn't sit any longer with her bad back. She is in terrible shape and seems to be in another world already. Has anyone of you lost someone from a failing heart valve? Pigs only live 15 yrs is what I read. Someone please help me. I believe this may be happening. Please share your knowledge with me about symptoms before death. Please. Thank you.
I just wanted to encourage anyone having to go though decision anxiety... just do it, most people have a very good outcome, like me.
And I am reading way to much doom and gloom here... yep.
Most importantly, pray to God for wisdom and healing.
In Jesus name,
Amen.
sincerely, GT
Thank you for this exciting information that takes me more in depth to something that could have shortened my life immensely.
I was rushed to the hospital for one thing and found my life was saved.
Now about 145-158/79- 85.Normally before this I had 110-120/69-75
Any one know whether this is common. None of the Doctors have mentioned any thing related to the valve. They haven't recommended any medications.