Type and screen
Definition
Blood typing is a laboratory test that identifies blood group antigens (substances that stimulate an immune response) belonging to the ABO blood group system. The test classifies blood into four groups designated A, B, AB, and O. Antibody screening is a test to detect atypical antibodies in the serum that may have been formed as a result of transfusion or pregnancy. An antibody is a protein produced by lymphocytes (nongranular white blood cells) that binds to an antigen, facilitating its removal by phagocytosis (or engulfing by macrophages) or lysis (cell rupture or decomposition). The type and screen (T&S) is performed on persons who may need a transfusion of blood products. These tests are followed by the compatibility test (cross-match). This test insures that no antibodies are detected in the recipient's serum that will react with the donor's red blood cells.
Purpose
Blood typing and screening are most commonly performed to ensure that a person who needs a transfusion will receive blood that matches (is compatible with) his or her own; and that clinically significant antibodies are identified if present. People must receive blood of the same blood type; otherwise, a severe transfusion reaction may result.
Prenatal care
Parents who are expecting a baby have their blood typed to diagnose and prevent hemolytic disease of the newborn (HDN), a type of anemia also known as erythroblastosis fetalis. Babies who have a blood type different from their mother's are at risk for developing this disease.
Determination of paternity
A child inherits factors or genes from each parent that determine his or her blood type. This fact makes blood typing useful in paternity testing. The blood types of the child, mother, and alleged father are compared to determine paternity.
Forensic investigations
Legal investigations may require typing of blood or such other body fluids as semen or saliva to identify criminal suspects. In some cases typing is used to identify the victims of crime or major disasters.
Description
Blood typing and screening tests are performed in a blood bank laboratory by technologists trained in blood bank and transfusion services. The tests are performed on blood after it has been separated into cells and serum (the yellow liquid left after the blood cells are removed). Costs for both tests are covered by insurance when the tests are determined to be medically necessary.
Blood bank laboratories are usually located in blood center facilities, such as those operated by the American Red Cross, that collect, process, and supply blood that is donated. Blood bank laboratories are also found in most hospitals and other facilities that prepare blood for transfusion. These laboratories are regulated by the United States Food and Drug Administration (FDA) and are inspected and accredited by a professional association such as the American Association of Blood Banks (AABB).
Blood typing and screening tests are based on the reaction between antigens and antibodies. An antigen can be anything that triggers the body's immune response. The body produces a special protein called an antibody that has a uniquely shaped site that combines with the antigen to neutralize it. A person's body normally does not produce antibodies against its own antigens.
The antigens found on the surface of red blood cells are important because they determine a person's blood type. When red blood cells having a certain blood type antigen are mixed with serum containing antibodies against that antigen, the antibodies combine with and stick to the antigen. In a test tube, this reaction is visible as clumping or aggregating.
Although there are over 600 known red blood cell antigens organized into 22 blood group systems, routine blood typing is usually concerned with only two systems: the ABO and Rh blood group systems. Antibody screening helps to identify antibodies against several other groups of red blood cell antigens.
Blood typing
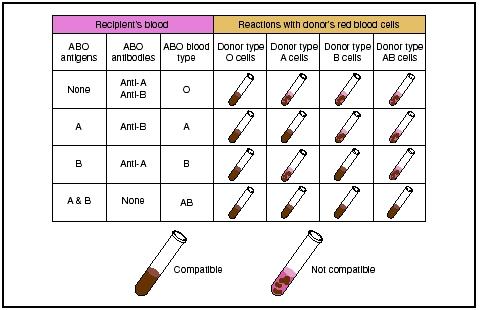
THE ABO BLOOD GROUP SYSTEM. In 1901, Karl Landsteiner, an Austrian pathologist, randomly combined the serum and red blood cells of his colleagues. From the reactions he observed in test tubes, he developed the ABO blood group system. This discovery earned him the 1930 Nobel Prize in Medicine. A person's ABO blood type—A, B, AB, or O—is based on the presence or absence of the A and B antigens on his red blood cells. The A blood type has only the A antigen and the B blood type has only the B antigen. The AB blood type has both A and B antigens, and the O blood type has neither the A nor the B antigen.
By the time a person is six months old, he or she will have developed antibodies against the antigens that his or her red blood cells lack. That is, a person with A blood type will have anti-B antibodies, and a person with B blood type will have anti-A antibodies. A person with AB blood type will have neither antibody, but a person with O blood type will have both anti-A and anti-B antibodies. Although the distribution of each of the four ABO blood types varies among racial groups, O is the most common and AB is the least common in all groups.
FORWARD AND REVERSE TYPING. ABO typing is the first test done on blood when it is tested for transfusion. A person must receive ABO-matched blood because ABO incompatibilities are the major cause of fatal transfusion reactions. To guard against these incompatibilities, typing is done in two steps. In the first step, called forward typing, the patient's blood is mixed with serum that contains antibodies against type A blood, then with serum that contains antibodies against type B blood. A determination of the blood type is based on whether or not the blood clots in the presence of these sera.
In reverse typing, the patient's blood serum is mixed with blood that is known to be type A and type B. Again, the presence of clotting is used to determine the type.
An ABO incompatibility between a pregnant woman and her baby is a common cause of HDN but seldom requires treatment. This is because the majority of ABO antibodies are IgM, which are too large to cross the placenta. It is the IgG component that may cause HDN, and this is most often present in the plasma of group O mothers.
Paternity testing compares the ABO blood types of the child, mother, and alleged father. The alleged father cannot be the biological father if the child's blood type requires a gene that neither he nor the mother have. For example, a child with blood type B whose mother has blood type O requires a father with either AB or B blood type; a man with blood type O cannot be the biological father.
In some people, ABO antigens can be detected in body fluids other than blood, such as saliva, sweat, or semen. People whose body fluids contain detectable amounts of antigens are known as secretors. ABO typing of these fluids provides clues in legal investigations.
THE RH BLOOD GROUP SYSTEM. The Rh, or Rhesus, system was first detected in 1940 by Landsteiner and Wiener when they injected blood from rhesus monkeys into guinea pigs and rabbits. More than 50 antigens have since been discovered that belong to this system, making it the most complex red blood cell antigen system.
In routine blood typing and cross-matching tests, only one of these 50 antigens, the D antigen, also known as the Rh factor or Rh o [D], is tested for. If the D antigen is present, that person is Rh-positive; if the D antigen is absent, that person is Rh-negative.
Other important antigens in the Rh system are C, c, E, and e. These antigens are not usually tested for in routine blood typing tests. Testing for the presence of these antigens, however, is useful in paternity testing, and in cases in which a technologist screens blood to identify unexpected Rh antibodies or find matching blood for a person with antibodies to one or more of these antigens.
Unlike the ABO system, antibodies to Rh antigens don't develop naturally. They develop only as an immune response after a transfusion or during pregnancy. The incidence of the Rh blood types varies between
The distribution of ABO and Rh blood groups in the overall United States population is as follows:
- O Rh-positive, 38%
- O Rh-negative, 7%
- A Rh-positive, 34%
- A Rh-negative, 6%
- B Rh-positive, 9%
- B Rh-negative, 2%
- AB Rh-positive, 3%
- AB Rh-negative, 1%
In transfusions, the Rh system is next in importance after the ABO system. Most Rh-negative people who receive Rh-positive blood will develop anti-D antibodies. A later transfusion of Rh-positive blood may result in a severe or fatal transfusion reaction.
Rh incompatibility is the most common and severe cause of HDN. This incompatibility may occur when an Rh-negative mother and an Rh-positive father have an Rh-positive baby. Cells from the baby can cross the placenta and enter the mother's bloodstream, causing the mother to make anti-D antibodies. Unlike ABO antibodies, the structure of anti-D antibodies makes it likely that they will cross the placenta and enter the baby's bloodstream. There, they can destroy the baby's red blood cells, causing a severe or fatal anemia.
The first step in preventing HDN is to find out the Rh types of the expectant parents. If the mother is Rhnegative and the father is Rh-positive, the baby is at risk for developing HDN. The next step is performing an antibody screen of the mother's serum to make sure she doesn't already have anti-D antibodies from a previous pregnancy or transfusion. Finally, the Rh-negative mother is given an injection of Rh immunoglobulin (RhIg) at 28 weeks of gestation and again after delivery, if the baby is Rh positive. The RhIg attaches to any Rh-positive cells from the baby in the mother's bloodstream, preventing them from triggering anti-D antibody production in the mother. An Rh-negative woman
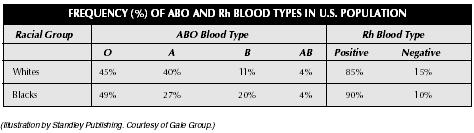
| Racial Group | ABO Blood Type | Rh Blood Type | ||||
| (Illustration by Standley Publishing. Courtesy of Gale Group.) | ||||||
| O | A | B | AB | Positive | Negative | |
| Whites | 45% | 40% | 11% | 4% | 85% | 15% |
| Blacks | 49% | 27% | 20% | 4% | 90% | 10% |
should also receive RhIg following a miscarriage, abortion, or ectopic pregnancy.
OTHER BLOOD GROUP SYSTEMS. Several other blood group systems may be involved in HDN and transfusion reactions, although they are much less common than ABO and Rh incompatibilities. Some of the other groups are the Duffy, Kell, Kidd, MNS, and P systems. Tests for antigens from these systems are not included in routine blood typing, but they are commonly used in paternity testing.
Like Rh antibodies, antibodies in these systems do not develop naturally, but as an immune response after transfusion or during pregnancy. An antibody screening test is done before a cross-match to check for unexpected antibodies to antigens in these systems. A person's serum is mixed in a test tube with commercially prepared cells containing antigens from these systems. If hemagglutination, or clumping, occurs, the antibody is identified.
Antibody screening
Antibody screening is done to look for unexpected antibodies to other blood groups, such as certain Rh (e.g. E, e, C, c), Duffy, MNS, Kell, Kidd, and P system antigens. The recipient's serum is mixed with screening reagent red blood cells. The screening reagent red blood cells are cells with known antigens. This test is sometimes called an indirect antiglobulin or Coombs test. If an antibody to an antigen is present, the mixture will cause agglutination (clumping) of the red blood cells or cause hemolysis (breaking of the red cell membrane). If an antibody to one of these antigens is found, only blood without that antigen will be compatible in a cross-match. This sequence must be repeated before each transfusion a person receives.
Testing for infectious disease markers
As of 2003, pretransfusion testing includes analyzing blood for the following infectious disease markers:
- Hepatitis B surface antigen (HBsAg). This test detects the outer envelope of the heptatitis B virus.
- Antibodies to the core of the hepatitis B virus (Anti-HBc). This test detects an antibody to the hepatitis B virus that is produced during and after an infection.
- Antibodies to the hepatitis C virus (Anti-HCV).
- Antibodies to human immunodeficiency virus, types 1 and 2 (Anti-HIV-1, -2).
- HIV-1 p24 antigen. This test screens for antigens of HIV-1. The advantage of this test is that it can detect HIV-1 infection a week earlier than the antibody test.
- Antibodies to human T-lymphotropic virus, types I and II (Anti-HTLV-I, -II). In the United States, HTLV infection is most common among intravenous drug users.
- Syphilis. This test is performed to detect evidence of infection with the spirochete Treponema pallidum .
- Nucleic acid amplification testing (NAT). NAT uses a new form of blood testing technology that directly detects the genetic material of the HCV and HIV viruses.
- Confirmatory tests. These are done to screen out false positives.
Cross-matching
Cross-matching is the final step in pretransfusion testing. It is commonly referred to as compatibility testing, or "type and cross." Before blood from a donor and the recipient are cross-matched, both are ABO and Rh typed. To begin the cross-match, a unit of blood from a donor with the same ABO and Rh type as the recipient is selected. Serum from the patient is mixed with red blood cells from the donor. The cross-match can be performed either as a short (5–10 min) incubation intended only to verify ABO compatibility or as a long (45 min) incubation with an antihuman globulin test intended to verify compatibility for all other red cell antigens. If clumping occurs, the blood is not compatible; if clumping does not occur, the blood is compatible. If an unexpected antibody is found in either the patient or the donor, the blood bank does further testing to ensure that the blood is compatible.
In an emergency, when there is not enough time for blood typing and cross-matching, O red blood cells may be given, preferably Rh-negative. O-type blood is called the universal donor because it has no ABO antigens for a patient's antibodies to combine with. In contrast, AB blood type is called the universal recipient because it has no ABO antibodies to combine with the antigens on transfused red blood cells. If there is time for blood typing, red blood cells of the recipient type (type-specific cells) are given. In either case, the cross-match is continued even though the transfusion has begun.
Autologous donation
The practice of collecting a patient's own blood prior to elective surgery for later transfusion is called autologous donation. Since the safest blood for transfusion is the patient's own, autologous donation is particularly useful for patients with rare blood types. Two to four units of blood are collected several weeks before surgery, and the patient is given iron supplements to build up his or her hemoglobin levels.
Preparation
To collect the 10 mL of blood needed for these tests, a healthcare worker ties a tourniquet above the patient's elbow, locates a vein near the inner elbow, cleans the skin overlying the vein, and inserts a needle into that vein. The blood is drawn through the needle into an attached vacuum tube. Collection of the sample takes only a few minutes.
Blood typing and screening must be done three days or less before a transfusion. A person does not need to change diet, medications, or activities before these tests. Patients should tell their health care provider if they have received a blood transfusion or a plasma substitute during the last three months, or have had a radiology procedure using intravenous contrast media. These can give false clumping reactions in both typing and cross-matching tests.
Aftercare
The possible side effects of any blood collection are discomfort, bruising, or excessive bleeding at the site where the needle punctured the skin, as well as dizziness or fainting. Bruising and bleeding is reduced if pressure is applied with a finger to the puncture site until the bleeding stops. Discomfort can be treated with warm packs to the puncture site.
Risks
Aside from the rare event of infection or bleeding, there are no risks from blood collection. Blood transfusions, however, always have the risk of an unexpected transfusion reaction. These complications may include an acute hemolytic transfusion reaction (AHTR), which is most commonly caused by ABO incompatibility. The patient may complain of pain, difficult breathing, fever and chills, facial flushing, and nausea. Signs of shock may appear, including a drop in blood pressure and a rapid but weak pulse. If AHTR is suspected, the transfusion should be stopped at once.
Other milder transfusion reactions include a delayed hemolytic transfusion reaction, which may occur one to two weeks after the transfusion. It consists of a slight fever and a falling hematocrit , and is usually self-limited. Patients may also have allergic reactions to unknown components in donor blood.
Normal results
The blood type is labeled as A+, A-, B+, B-, O+, O-, AB+, or AB-, based on both the ABO and Rh systems. If antibody screening is negative, only a cross-match is necessary. If the antibody screen is positive, then blood that is negative for those antigens must be identified. The desired result of a cross-match is that compatible donor blood is found. Compatibility testing procedures are designed to provide the safest blood product possible for the recipient, but a compatible cross-match is no guarantee that an unexpected adverse reaction will not appear during the transfusion.
Except in an emergency, a person cannot receive a transfusion without a compatible cross-match result. In rare cases, the least incompatible blood has to be given.
See also Blood donation and registry ; Transfusion .
Resources
books
Beadling, Wendy V., Laura Cooling, and John B. Henry. "Immunohematology." In Clinical Diagnosis and Management by Laboratory Methods , 20th ed., edited by John B. Henry. Philadelphia: W. B. Saunders Company, 2001.
Boral, Leonard I., Edward D. Weiss, and John B. Henry. "Transfusion Medicine." In Clinical Diagnosis and Management by Laboratory Methods , 20th ed. Edited by John B. Henry. Philadelphia: W. B. Saunders Company, 2001.
Daniels, Geoff. Human Blood Groups . Oxford, UK: Blackwell, 1995.
Issitt, Peter D. and David J. Anstee Applied Blood Group Serology , 4th ed. Durham, NC: Montgomery Scientific Publications, 1998.
Triulzi, Darrell J., ed. Blood Transfusion Therapy: A Physi cian's Handbook , 7th ed. Bethesda: American Association of Blood Banks, 2002.
organizations
American Association of Blood Banks (AABB). 8101 Glenbrook Road, Bethesda, MD 20814. (301) 907-6977. http://www.aabb.org [cited March 15, 2003].
American College of Obstetricians and Gynecologists. 409 12th Street SW, Washington, DC 20024-2188. (202) 638-5577. http://www.acog.org [cited April 4, 2003].
American Red Cross Blood Services. 430 17th Street NW, Washington, DC 20006. (202) 737-8300. http://www.redcross.org [cited March 15, 2003].
other
American Association of Blood Banks. All About Blood. Bethesda, MD: American Association of Blood Banks, http://www.aabb.org/All_About_Blood/FAQs/aabb_faqs.htm June 2002. [cited April 7, 2003].
Mark A. Best
THX,
KM chan
Yes everyone can receive O. For emergency rooms O negative blood is always in stock because everyone can receive it.
if parents are both o+ can baby be type b if so how does this happen
No. If you have an O blood type your phenotype is OO (because it is recessive) which means they can only have a baby with type O
MAIL ME AT pierre7@webmail.co.za
Thanks
Standard Range
4/9/12 3/1/16
ABO GROUP O O
ANTIBODY SCREEN Negative Negative
RH (D) TYPE Positive Positive
Please explain this I'm read it as O- RH+