Snoring surgery
Definition
Snoring is defined as noisy or rough breathing during sleep, caused by vibration of loose tissue in the upper airway. Surgical treatments for snoring include several different techniques for removing tissue from the back of the patient's throat, reshaping the nasal passages or jaw, or preventing the tongue from blocking the airway during sleep.
Purpose
The purpose of snoring surgery is to improve or eliminate the medical and social consequences of heavy snoring. Most insurance companies, however, regard surgical treatment of snoring as essentially a cosmetic procedure—which means that patients must cover its expenses themselves. The major exception is surgery to correct a deviated septum or other obstruction in the nose, on the grounds that nasal surgery generally improves the patient's breathing during the day as well as at night.
Snoring as a medical problem
The connection between heavy snoring, breathing disorders, and other health problems is a relatively recent discovery. Obstructive sleep apnea (OSA) is a breathing disorder that was first identified in 1965. OSA is marked by brief stoppages in breathing during sleep resulting from partial blockage of the airway. A person with OSA may stop breathing temporarily as often as 20–30 times per hour. He or she usually snores or makes choking and gasping sounds between these episodes. The person is not refreshed by nighttime sleep and may suffer from morning headaches as well as daytime sleepiness. He or she may be misdiagnosed as suffering from clinical depression when the real problem is physical tiredness. In addition, the high levels of carbon dioxide that build up in the blood when a person is not breathing normally may eventually lead to high blood pressure, irregular heartbeat, heart attacks, and stroke. In children, heavy snoring appears to be a major risk factor for attention-deficit/hyperactivity disorder.
Although people with OSA snore, not everyone who snores has OSA. It is thought that OSA affects about 4% of middle-aged males and 2% of middle-aged females. Most adults who snore have what is called primary snoring, which means that the loud sounds produced in the upper airway during sleep are not interrupted by episodes of breathing cessation. Other terms for primary snoring are simple snoring, benign snoring, rhythmical snoring, continuous snoring, and socially unacceptable snoring (SUS). Although primary snoring is not associated with severe disorders to the same extent as OSA, it has been shown to have some negative consequences for health. A study published in April 2003 reported that habitual primary snoring is a risk factor for chronic daily headaches.
Snoring as a social problem
As the term SUS suggests, primary snoring can cause the same social problems for a person as does snoring associated with OSA. People who snore heavily often keep other family members, roommates, or even neighbors from getting a good night's sleep, which leads to considerable anger and resentment. Recent studies have found that the nonsnoring partner or roommate loses an average of an hour's sleep each night. According to Dr. Kingman Strohl, head of a sleep disorders program in a Veterans Administration hospital, even the average volume of snoring (60 decibels or dB) is as loud as normal speech. Some people, however, snore around 80–82 dB, the sound level of a loud yell; a few have been recorded as reaching 90 dB, the sound level of loud rock music. One study found that 80% of people married to heavy snorers end up sleeping in separate rooms. A group of Swedish researchers reported that heavy snoring has the same level of negative effects on quality of life among adult males as high blood pressure, chronic obstructive pulmonary disease, heart disease, and similar chronic medical conditions.
Risk factors for snoring
Some people are at higher risk of developing problem snoring than others. Risk factors in addition to sex and age include:
- Genetic factors. The size and shape of the uvula, soft palate, tonsils, and other parts of the airway are largely determined by heredity.
- Family history of heavy snoring.
- Obesity. Severe overweight increases a person's risk of developing OSA.
- Lack of exercise . Physical activity helps to keep the muscles of the throat firm and strong as well as the larger muscles of the body.
- Heavy consumption of alcohol and tobacco.
- A history of frequent upper respiratory infections or allergies.
- Trauma to the nose, face, or throat.
Demographics
Snoring is a commonplace problem in the general population in North America. About 12% of children over the age of five are reported to snore frequently and loudly. Among adults, 45% snore occasionally, while 25% snore almost every night. The problem usually grows worse as people age; 50% of people over age 65 are habitual snorers.
Problem snoring is worse among males than among females in all age brackets. With regard to racial and ethnic differences, a sleep research study published in 2003 reported that frequent snoring is more common (in the United States) among African American women, Hispanic women, and Hispanic men than their Caucasian counterparts, even after adjusting for weight and body mass index (BMI). African American, Native American, and Asian American males have the same rates of snoring as Caucasian males. Further research is needed to determine whether these differences are related to variations in the rates and types of health problems in these respective groups.
According to international researchers, heavy snoring appears to be more common in persons of Asian origin than in persons of Middle Eastern, European, or African origin.
Description
With the exception of UPPP, all of the surgical treatments for snoring described in this section are outpatient or office-based procedures.
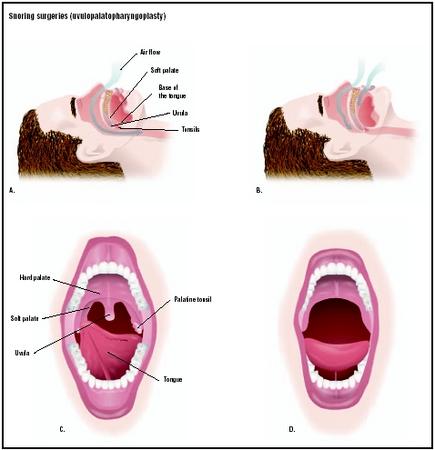
Uvulopalatopharyngoplasty (UPPP)
Uvulopalatopharyngoplasty, or UPPP, is the oldest and most invasive surgical treatment for snoring. It was first performed in 1982 by a Japanese surgeon named S. Fujita. UPPP requires general anesthesia, one to two nights of inpatient care in a hospital, and a minimum of two weeks of recovery afterward. In a uvulopalatopharyngoplasty, the surgeon resects (removes) the patient's tonsils, part of the soft palate, and the uvula. The procedure works by enlarging the airway and removing some of the soft tissue that vibrates when the patient snores. It is not effective in treating snoring caused by obstructions at the base of the tongue.
UPPP has several drawbacks in addition to its cost and lengthy recovery period. It can result in major complications, including severe bleeding due to removal of the tonsils as well as airway obstruction. In addition, the results may not be permanent; between 50% and 70% of patients who have been treated with UPPP report that short-term improvements in snoring do not last longer than a year.
Laser-assisted uvulopalatoplasty
Laser-assisted uvulopalatoplasty, or LAUP, is an out-patient surgical treatment for snoring in which a carbon dioxide laser is used to vaporize part of the uvula, a small triangular piece of tissue that hangs from the soft palate above the back of the tongue. The patient is seated upright in a comfortable chair in the doctor's office. The doctor first sprays a local anesthetic—usually lidocaine—over the back of the patient's throat, covering the patient's soft palate, tonsils, and uvula. The second step is the injection of more anesthetic into the muscle tissue in the uvula. After waiting for the anesthetic to take effect, the surgeon uses a carbon dioxide laser to make two vertical incisions in the soft palate on either side of the uvula. A third incision is used to remove the tip of the uvula. The surgeon also usually removes part of the soft palate itself. The total procedure takes about half an hour.
LAUP is typically performed as a series of three to five separate treatments. Additional treatment sessions, if needed, are spaced four to eight weeks apart.
LAUP was developed in the late 1980s by Dr. Yves-Victor Kamami, a French surgeon whose first article on the technique was published in 1990. Kamami claimed a high rate of success for LAUP in treating a condition known as obstructive sleep apnea (OSA) as well as snoring. The procedure has become controversial because other surgeons found it less effective than the first reports indicated, and also because most patients suffer considerable pain for about two weeks after surgery. Although some surgeons report a success rate as high as 85% in treating snoring with LAUP, the effectiveness of the procedure is highly dependent on the surgeon's experience and ability.
Somnoplasty
Somnoplasty, or radiofrequency volumetric tissue reduction (RFVTR) is a newer technique in which the surgeon uses a thin needle connected to a source of radiofrequency signals to shrink the tissues in the soft palate, throat, or tongue. It was approved by the Food and Drug Administration (FDA) for the treatment of snoring in 1997. The needle is inserted beneath the surface layer of cells and heated to a temperature between 158°F (70°C) and 176°F (80°C). The upper layer of cells is unaffected, but the heated tissue is destroyed and gradually reabsorbed by the body over the next four to six weeks. Somnoplasty stiffens the remaining layers of tissue as well as reducing the total volume of tissue. Some patients require a second treatment, but most find that their snoring is significantly improved after only one. The procedure takes about 30 minutes and is performed under local anesthesia.
Somnoplasty appears to have a higher success rate (about 85%) than LAUP and is considerably less painful. Most patients report two to three days of mild swelling after somnoplasty compared to two weeks of considerable discomfort for LAUP.
Tongue suspension procedure
The tongue suspension procedure, which is also known as the Repose™ system, is a minimally invasive surgical treatment for snoring that stabilizes the base of the tongue during sleep, preventing it from falling backward and obstructing the airway. The Repose system was approved by the FDA in 1998. It consists of a titanium screw inserted into the lower jaw on the floor of the mouth and a suture passed through the base of the tongue that is then attached to the screw. The attachment holds the tongue forward during sleep.
The Repose system is done as an outpatient procedure under total anesthesia. It takes about 15–20 minutes to complete. The advantages of the tongue suspension procedure include the fact that it is reversible, since no incision is made; and that it can be combined with UPPP, LAUP, or a tonsillectomy . Its disadvantages include its relatively long healing time (one to two weeks) and the fact that it appears to be more effective in treating OSA than primary snoring. One team of American and Israeli researchers who conducted a multicenter trial concluded that the tongue suspension procedure requires further evaluation.
Injection snoreplasty
Injection snoreplasty was developed by a team of Army physicians at Walter Reed Hospital and introduced to other ear, nose and throat specialists at a professional conference in 2000. In injection snoreplasty, the surgeon gives the patient a local anesthetic and then injects a hardening agent known as sodium tetradecyl sulfate underneath the skin of the roof of the mouth just in front of the uvula. The chemical, which is also used in sclerotherapy, creates a blister that hardens into scar tissue. The scar tissue pulls the uvula forward, reducing the vibration or flutter that causes snoring.
Preliminary research indicates that injection snore-plasty is safe, has a higher rate of success than LAUP (about 92%), and is also less painful. Most patients need only one treatment, and can manage the discomfort the next day with a mild aspirin substitute and throat spray. The primary drawback of injection snoreplasty is that it treats only tissues in the area of the uvula. Snoring caused by tissue vibrations elsewhere in the throat requires another form of treatment. Injection snoreplasty costs about $500 per treatment.
Diagnosis/Preparation
Diagnosis
The most important task in diagnosing a patient's snoring is to distinguish between primary snoring and obstructive sleep apnea. The reason for care in the diagnosis is that surgical treatment without the recommended tests for OSA can complicate later diagnosis of the disorder.
The sounds made when a person snores have a number of different physical causes. Snoring noises may result from one or more of the following:
- An unusually long soft palate and uvula. These structures narrow the airway between the nose and the throat. They act like noisy flutter valves when the person breathes in and out during sleep.
- Too much tissue in the throat. Large tonsils and adenoids can cause snoring, which is one reason why tonsillectomies are sometimes recommended to treat heavy snoring in children.
- Nasal congestion. When a person's nose is stuffy, their attempts to breathe create a partial vacuum in the throat that pulls the softer tissues of the throat together. This suction can also produce a snoring noise. Nasal congestion helps to explain why some people snore only when they have a cold or during pollen season.
- Anatomical deformations of the nose. People who have had their noses or cheekbones fractured or who have a deviated septum are more likely to snore, because their nasal passages develop a twisted or crooked shape and vibrate as air passes through them.
- Sleeping position. People are more likely to snore when they are lying on the back because the force of gravity draws the tongue and soft tissues in the throat backward and downward, blocking the airway.
- Obesity. Obesity adds to the weight of the tissues in the neck, which can cause partial blockage of the airway during sleep.
- Use of alcohol, sleeping medications, or tranquilizers. These substances relax the throat muscles, which may become soft or limp enough to partially close the airway.
Because snoring may be related to lifestyle factors, upper respiratory infections, seasonal allergies, and sleeping habits as well as the anatomy of the person's airway, a complete medical history is the first step in determining suitable treatments. In some cases the patient may have been referred by his or her dentist on the basis of findings during a dental procedure. A primary care doctor can take a history and perform a basic examination of the patient's nose and throat. In addition, the primary care doctor may give the patient one or more short questionnaires to evaluate the severity of daytime sleepiness and other problems related to snoring. The test most commonly used is the Epworth Sleepiness Scale (ESS), which was developed by an Australian physician, Dr. Murray Johns, in 1991. The ESS lists eight situations (reading, watching TV, etc.) and asks the patient to rate his or her chances of dozing off in each situation on a four-point scale (0–3, with 3 representing a high chance of falling asleep). A score of 6 or lower indicates that the person is getting enough sleep; a score higher than 9 is a danger sign. The ESS is often used to measure the effectiveness of various treatments for snoring as well as to evaluate patients prior to surgery.
The next stage in the differential diagnosis of snoring problems is a detailed examination of the patient's airway by an otolaryngologist, who is a physician who specializes in diagnosing and treating disorders involving the nose and throat. The American Sleep Apnea Association (ASAA) maintains that no one should consider surgery for snoring until their airway has been examined by a specialist. The otolaryngologist will be able to determine whether the size and shape of the patient's uvula, soft palate, tonsils and adenoids, nasal cartilage, and throat muscles are contributing factors, and to advise the patient on specific procedures. It may be necessary for the patient to undergo more than one type of treatment for snoring, as some surgical procedures correct only one or two structures in the nose or throat.
A complete airway examination consists of an external examination of the patient's face and neck; an endoscopic examination of the nasal passages and throat; the use of a laryngeal mirror or magnifying laryngoscope to study the lower portions of the throat; and various imaging studies. The otolaryngologist may use a nasopharyngoscope, which allows for evaluation of obstructions below the palate and the tongue, and may be performed with the patient either awake or asleep. The nasopharyngoscope is a flexible fiberoptic device that is introduced into the airway through the patient's nose. Other imaging studies that may be done include acoustic reflection, computed tomography (CT) scans, or magnetic resonance imaging (MRI).
In addition to the airway examination, patients considering surgical treatment for snoring must make an appointment for sleep testing in a specialized laboratory. The American Academy of Sleep Medicine recommends this step in order to exclude the possibility that the patient has obstructive sleep apnea. Sleep testing consists of an overnight stay in a special sleep laboratory. Before the patient goes to sleep, he or she will be connected to a polysomnograph, which is an instrument that monitors the patient's breathing, heart rate, temperature, muscle movements, airflow, body position, and other measurements that are needed to evaluate the cause(s) of sleep disorders. A technician records the data in a separate room. As of 2003, some companies are developing portable polysomnographs that allow patients to connect the device to a computer in their home and transmit the data to the sleep center over an Internet connection.
Preparation
Apart from the extensive diagnostic testing that is recommended, preparation for outpatient snoring surgery is usually limited to taking a mild sedative before the procedure. Preparation for UPPP requires a physical examination , EKG, blood tests, and a preoperation interview with the anesthesiologist to evaluate the patient's fitness for general anesthesia.
Aftercare
Aftercare following outpatient snoring surgery consists primarily of medication for throat discomfort, particularly when swallowing. The patient can resume normal work and other activities the same day as the procedure, and speaking is usually not affected.
Risks
In addition to the risk of an allergic reaction to the local anesthetic, snoring surgery is associated with the following risks:
- Severe pain following the procedure that lasts longer than two to three days. This complication occurs more frequently with LAUP than with somnoplasty or injection snoreplasty.
- Causation or worsening of obstructive sleep apnea. LAUP has been reported to cause OSA in patients who had only primary snoring before the operation.
- Nasal regurgitation. This complication refers to food shooting or leaking through the nose when the patient swallows.
- Dehydration. This complication has been reported with the tongue suspension procedure.
- Permanent change in the quality of the patient's voice.
- Recurrence of primary snoring.
Normal results
In general, surgical treatment for snoring appears to be most effective in patients whose primary problem is nasal obstruction. The results of snoring surgery depend to a large degree on a good "fit" between the anatomy of a specific patient's airway and the specific procedure performed, as well as on the individual surgeon's skills.
Morbidity and mortality rates
Mortality rates for UPPP are related to complications of OSA rather than to the procedure itself. With regard to the outpatient procedures for snoring, mortality rates are very close to zero because these surgeries are performed under local anesthesia. Complication rates, however, are high with both UPPP and LAUP. According to one European study, as many as 42% of patients have complications following UPPP, with 14% reporting general dissatisfaction with the results of surgery. Specific complication rates for UPPP are 15% for recurrence of snoring; 13% for nasal regurgitation; 10% for excessive throat secretions; 9% for swallowing problems; and 7% for speech disturbances. Complications for LAUP have been estimated to be 30–40% for recurrence of snoring; 30% for causing or worsening of OSA; 5%–10% for persistent nasal regurgitation; 1% for permanent change in vocal quality.
As of early 2003, no morbidity figures have been published for somnoplasty or injection snoreplasty.
Alternatives
Oral devices and appliances
Oral appliances are intended to reduce snoring by changing the shape of the oral cavity or preventing the tongue from blocking the airway. There are three basic types of mouthpieces: those that push the lower jaw forward; those that raise the soft palate; and those that restrain the tongue from falling backward during sleep. To work properly, oral appliances should be fitted by an experienced dentist or orthodontist and checked periodically for proper fit. Their major drawback is a low rate of patient compliance; one German study found that only 30% of patients fitted with these devices were still using them after four years. In addition, oral appliances cannot be used by patients with gum disease, dental implants , or teeth that are otherwise in poor condition.
Continuous positive airway pressure (CPAP) devices
CPAP devices are masks that fit over the nose during sleep and deliver air into the airway under enough pressure to keep the airway open. If used correctly, CPAP devices can be an effective alternative to surgery. Their main drawback is a relatively low rate of patient compliance; the mask must be used every night, and some people feel mildly claustrophobic when using it. In addition, patients are often asked to lose weight or stop smoking while using CPAP, which are lifestyle adjustments that some would rather not make.
Lifestyle changes
Patients who snore only occasionally or who are light snorers may be helped by one or more of the following changes without undergoing surgery:
- Losing weight and getting adequate physical exercise.
- Avoiding tranquilizers, sleeping pills, antihistamines, or alcoholic beverages before bedtime.
- Quitting smoking.
-
Sleeping on the side rather than the back. One do-it-yourself device
that is sometimes recommended to
l
keep the patient turned on his or her side is a tennis ball placed inside a sock and attached to the back of the pajamas or nightgown. This approach seems to work for some patients with simple snoring. - Tilting the head of the bed upward about 4 in (10 cm).
Complementary and alternative (CAM) approaches
There are three forms of alternative treatment that have been shown to be helpful in reducing primary snoring in patients with histories of nasal congestion or swollen tissues in the throat. The first is acupuncture. Treatments for snoring usually focus on acupuncture points on the stomach, arms, and legs associated with the production of excess mucus. Insertion of the acupuncture needles at these points is thought to stimulate the body to release the excess moisture or phlegm.
Homeopathy and aromatherapy also appear to benefit some patients whose snoring is related to colds, allergies, or sore throats. Homeopathic remedies for snoring are available as nose drops and throat sprays as well as the traditional pill formulations. Aromatherapy formulas for snoring typically contain marjoram oil, which may be used alone or combined with lavender and other herbs that clear the nasal passages. Some people find aromatherapy preparations helpful alongside mainstream treatments because their fragrance is pleasant and relaxing.
See also Tonsillectomy ; Weight management .
Resources
books
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders , 4th edition, text revision, "Sleep Disorders.". Washington, DC: American Psychiatric Association, 2000.
"Disorders of the Oral Region." Section 9, Chapter 105 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, M.D., and Robert Berkow, M.D. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
Pelletier, Kenneth R., M.D. The Best Alternative Medicine , Part I, Chapter 5, "Acupuncture," and Chapter 8, "Homeopathy." New York: Simon & Schuster, 2002.
Price, Shirley. Practical Aromatherapy , 3rd ed. London, UK: Thorsons, 1994.
"Sleep Disorders." Section 14, Chapter 173 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, M.D., and Robert Berkow, M.D. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
periodicals
Back, L. J., P. O. Tervahartiala, A. K. Piilonen, et al. "Bipolar Radiofrequency Thermal Ablation of the Soft Palate in Habitual Snorers Without Significant Desaturations Assessed by Magnetic Resonance Imaging." American Journal of Respiratory and Critical Care Medicine 166 (September 15, 2002): 865-871.
Blumen, M. B., S. Dahan, B. Fleury, et al. "Radiofrequency Ablation for the Treatment of Mild to Moderate Obstructive Sleep Apnea." Laryngoscope 112 (November 2002): 2086–2092.
Brietzke, S. E., and E. A. Mair. "Injection Snoreplasty: How to Treat Snoring Without All the Pain and Expense." Otolaryngology and Head and Neck Surgery 124 (May 2001): 503–510.
Cartwright, R., T. K. Venkatesan, D. Caldarelli, and F. Diaz. "Treatments for Snoring: A Comparison of Somnoplasty and an Oral Appliance." Laryngoscope 110 (October 2000): 1680–1683.
Fischer, Y., B. Hafner, and W. J. Mann. "Radiofrequency Ablation of the Soft Palate (Somnoplasty). A New Method in the Treatment of Habitual and Obstructive Snoring." [in German] HNO 48 (January 2000): 33–40.
Grontved, A. M., and P. Karup. "Complaints and Satisfaction After Uvulopalatopharyngoplasty." Acta Otolaryngologica Supplementum 543 (2000): 190–192.
Hessel, N. S., and N. de Vries. "Diagnostic Workup of Socially Unacceptable Snoring. II. Sleep Endoscopy." European Archives of Oto-Rhino-Laryngology 259 (March 2002): 158–161.
Kamami, Y. V. "Laser CO 2 for Snoring. Preliminary Results." Acta Oto-Rhino-Laryngologica Belgica 44 (1990): 451-456.
Kyrmizakis, D. E., C. E. Papadakis, J. G. Bizakis, et al. "Sucralfate Alleviating Post-Laser-Assisted Uvulopalatoplasty Pain." American Journal of Otolaryngology 22 (January-February 2001): 55–58.
Littner, Michael, M.D., Clete A. Kushida, M.D., Ph.D., Kristyna Hartse, Ph.D., et al. "Practice Parameters for the Use of Laser-Assisted Uvulopalatoplasty: An Update for 2000." Sleep 24 (May 2001): 603–609.
Loth, S., B. Petruson, L. Wiren, and L. Wilhelmsen. "Evaluation of the Quality of Life of Male Snorers Using the Nottingham Health Profile." Acta Oto-Laryngologica 118 (September 1998): 723–727.
Morgan, Charles E., M.D., and Kenneth Johnson, M.D. "Snoring and Obstructive Sleep Apnea, Surgery." eMedicine , May 20, 2002 [cited May 10, 2003]. http://www.emedicine.com/ent/topic370.htm .
Nuñez-Fernandez, David, M.D., and Manuel Fernandez-Muradas, M.D. "Snoring and Obstructive Sleep Apnea, Upper Airway Evaluation." eMedicine , June 6, 2002 [cited May 10, 2003]. http://www.emedicine.com/ent/topic410.htm .
O'Brien, L. M., C. R. Holbrook, C. B. Mervis, et al. "Sleep and Neurobehavioral Characteristics of 5- to 7-Year-Old Children with Parentally Reported Symptoms of Attention-Deficit/Hyperactivity Disorder." Pediatrics 111 (March 2003): 554–563.
O'Connor, G. T., B. K. Lind, E. T. Lee, et al. "Variation in Symptoms of Sleep-Disordered Breathing with Race and Ethnicity: The Sleep Heart Health Study." Sleep 26 (February 1, 2003): 74–79.
Raphaelson, M., and T. S. Hakim. "Diagnosing Sleep Apnea in Dental Patients." Dental Clinics of North America 45 (October 2001): 797–816.
Rose, E., R. Staats, J. Schulte-Monting, et al. "Long-Term Compliance with an Oral Protrusive Appliance in Patients with Obstructive Sleep Apnoea." [in German] Deutsche medizinische Wochenschrift 127 (June 7, 2002): 1245–1249.
Ryan, C. F., and L. L. Love. "Unpredictable Results of Laser Assisted Uvulopalatoplasty in the Treatment of Obstructive Sleep Apnoea." Thorax 55 (May 2000): 399–404.
Scher, A. I., R. B. Lipton, and W. F. Stewart. "Habitual Snoring as a Risk Factor for Chronic Daily Headache." Neurology 60 (April 22, 2003): 1366–1368.
Seemann, R. P., J. C. DiToppa, M. A. Holm, and J. Hanson. "Does Laser-Assisted Uvulopalatoplasty Work? An Objective Analysis Using Pre- and Postoperative Polysomnographic Studies." Journal of Otolaryngology 30 (August 2001): 212–215.
Truelson, John M., MD, and D. Heath Roberts, DDS. "Snoring and Obstructive Sleep Apnea, Prosthetic Management." eMedicine , April 15, 2002 [cited May 10, 2003]. http://www.emedicine.com/ent/topic498.htm .
Woodson, B. T., A. Derowe, M. Hawke, et al. "Pharyngeal Suspension Suture with Repose Bone Screw for Obstructive Sleep Apnea." Otolaryngology and Head and Neck Surgery 122 (March 2000): 395–401.
organizations
American Academy of Medical Acupuncture (AAMA). 4929 Wilshire Boulevard, Suite 428, Los Angeles, CA 90010. (323) 937-5514. http://www.medicalacupuncture.org .
American Academy of Otolaryngology, Head and Neck Surgery, Inc. One Prince Street, Alexandria, VA 22314-3357. (703) 836-4444. http://www.entnet.org .
American Academy of Sleep Medicine (AASM). One Westbrook Corporate Center, Suite 920, Westchester, IL 60154. (708) 492-0930. http://www.aasmnet.org .
American Dental Association. 211 East Chicago Avenue, Chicago, IL 60611. (312) 440-2500. http://www.ada.org .
American Sleep Apnea Association (ASAA). 1424 K Street NW, Suite 302, Washington, DC 20005. (202) 293-3650. http://www.sleepapnea.org .
National Center on Sleep Disorders Research (NCSDR). Two Rockledge Centre, Suite 10038, 6701 Rockledge Drive, MSC 7920, Bethesda, MD 20892-7920. (301) 435-0199. http://www.nhlbi.nih.gov/about/ncsdr/index.htm .
other
American Sleep Apnea Association (ASAA). Considering Surgery for Snoring? [May 10, 2003]. http://www.sleepapnea.org/snoring.html .
National Heart, Lung, and Blood Institute (NHLBI). Facts About Sleep Apnea . NIH Publication No. 95-3798 [cited April 13, 2003]. http://www.nhlbi.nih.gov/health/public/sleep/sleepapn.htm .
Rebecca Frey, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Snoring surgery is done by a head and neck surgeon, a plastic surgeon, or an otolaryngologist, who is a doctor with special training in treating disorders of the ear, nose, and throat. UPPP is performed under general anesthesia and requires an overnight hospital stay. LAUP, somnoplasty, the tongue suspension procedure, and injection snoreplasty are performed as outpatient surgery , usually in a doctor's office or other outpatient facility.
Prosthetic devices to alter the position of the jaw or restrain the tongue during sleep are prescribed and fitted by general dentists or orthodontists.
Polysomnography as a part of a diagnostic workup is done in a special sleep laboratory by experts who are trained in the use of the equipment and interpretation of the results. Recent advances in technology, however, may allow patients to be monitored at home with portable polysomnographs and a computer with an Internet connection.
QUESTIONS TO ASK THE DOCTOR
- How often have you performed surgery for primary snoring? Which procedures have you performed most frequently?
- What is your opinion of somnoplasty and injection snoreplasty?
- Am I likely to benefit from lifestyle changes or other less invasive alternatives?
- Should I talk to my dentist about an oral appliance to control snoring?
thanks.
with my husband, the snoring keeps him awake. So besides the breathing and waking up at night, the snoring keeps everyone awake. My entire family, parents, siblings and even their children, hav sleep apnea and sores.