Kidney transplant
Definition
Kidney transplantation is a surgical procedure to remove a healthy, functioning kidney from a living or brain-dead donor and implant it into a patient with nonfunctioning kidneys.
Purpose
Kidney transplantation is performed on patients with chronic kidney failure, or end-stage renal disease (ESRD). ESRD occurs when a disease, disorder, or congenital condition damages the kidneys so that they are no longer capable of adequately removing fluids and wastes from the body or of maintaining the proper level of certain kidney-regulated chemicals in the bloodstream. Without long-term dialysis or a kidney transplant, ESRD is fatal.
Demographics
Diabetes mellitus is the leading single cause of ESRD. According to the 2002 Annual Data Report of the United States Renal Data System (USRDS), 42% of non-Hispanic dialysis patients in the United States have ESRD caused by diabetes. People of Native American and Hispanic descent are at an elevated risk for both kidney disease and diabetes.
Hypertension (high blood pressure) is the second leading cause of ESRD in adults, accounting for 25.5% of the patient population, followed by glomerulonephritis (8.4%). African Americans are more likely to develop hypertension-related ESRD than Caucasians and Hispanics.
Among children and young adults under 20 on dialysis, glomerulonephritis is the leading cause of ESRD
Description
Kidney transplantation involves surgically attaching a functioning kidney, or graft, from a brain-dead organ donor (a cadaver transplant) or from a living donor to a patient with ESRD. Living donors may be related or unrelated to the patient, but a related donor has a better chance of having a kidney that is a stronger biological match for the patient.
Open nephrectomy
The surgical procedure to remove a kidney from a living donor is called a nephrectomy . In a traditional, open nephrectomy, the kidney donor is administered general anesthesia and a 6–10-in (15.2–25.4-cm) incision through several layers of muscle is made on the side or front of the abdomen. The blood vessels connecting the kidney to the donor are cut and clamped, and the ureter is also cut and clamped between the bladder and kidney. The kidney and an attached section of ureter are removed from the donor. The vessels and ureter in the donor are then tied off and the incision is sutured together again. A similar procedure is used to harvest cadaver kidneys, although both kidneys are typically removed at once, and blood and cell samples for tissue typing are also taken.
Laparoscopic nephrectomy
Laparoscopic nephrectomy is a form of minimally invasive surgery using instruments on long, narrow rods to view, cut, and remove the donor kidney. The surgeon views the kidney and surrounding tissue with a flexible videoscope. The videoscope and surgical instruments are maneuvered through four small incisions in the abdomen, and carbon dioxide is pumped into the abdominal cavity to inflate it for an improved visualization of the kidney. Once the kidney is freed, it is secured in a bag and pulled through a fifth incision, approximately 3 in (7.6 cm) wide, in the front of the abdominal wall below the navel. Although this surgical technique takes slightly longer than an open nephrectomy, studies have shown that it promotes a faster recovery time, shorter hospital stays, and less postoperative pain for kidney donors.
A modified laparoscopic technique called hand-assisted laparoscopic nephrectomy may also be used to remove the kidney. In the hand-assisted surgery, a small incision of 3–5 in (7.6–12.7 cm) is made in the patient's abdomen. The incision allows the surgeon to place his hand in the abdominal cavity using a special surgical glove that also maintains a seal for the inflation of the abdominal cavity with carbon dioxide. The technique gives the surgeon the benefit of using his or her hands to feel the kidney and related structures. The kidney is then removed through the incision by hand instead of with a bag.
Once removed, kidneys from live donors and cadavers are placed on ice and flushed with a cold preservative solution. The kidney can be preserved in this solution for 24–48 hours until the transplant takes place. The sooner the transplant takes place after harvesting the kidney, the better the chances are for proper functioning.
Kidney transplant
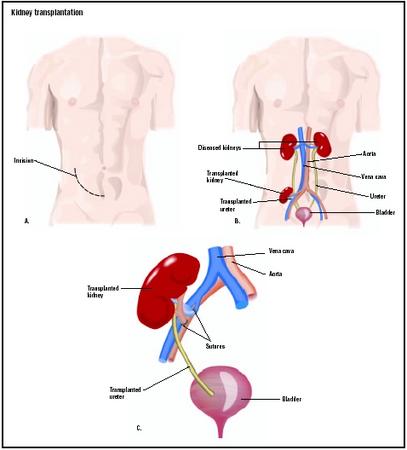
During the transplant operation, the kidney recipient is typically under general anesthesia and administered antibiotics to prevent possible infection. A catheter is placed in the bladder before surgery begins. An incision is made in the flank of the patient, and the surgeon implants the kidney above the pelvic bone and below the existing, non-functioning kidney by suturing the kidney artery and vein to the patient's iliac artery and vein. The ureter of the new kidney is attached directly to the kidney recipient's bladder. Once the new kidney is attached, the patient's existing, diseased kidneys may or may not be removed, depending on the circumstances surrounding the kidney failure. Barring any complications, the transplant operation takes about three to four hours.
Since 1973, Medicare has picked up 80% of ESRD treatment costs, including the costs of transplantation for both the kidney donor and the recipient. Medicare also covers 80% of immunosuppressive medication costs for up to three years. To qualify for Medicare ESRD benefits, a patient must be insured or eligible for benefits under Social Security, or be a spouse or child of an eligible American. Private insurance and state Medicaid programs often cover the remaining 20% of treatment costs.
Patients with a history of heart disease, lung disease, cancer, or hepatitis may not be suitable candidates for receiving a kidney transplant.
Diagnosis/Preparation
Patients with chronic renal disease who need a transplant and do not have a living donor registered with United Network for Organ Sharing (UNOS) to be placed on a waiting list for a cadaver kidney transplant. UNOS is a non-profit organization that is under contract with the federal government to administer the Organ Procurement and Transplant Network (OPTN) and the national Scientific Registry of Transplant Recipients (SRTR).
Kidney allocation is based on a mathematical formula that awards points for factors that can affect a successful transplant, such as time spent on the transplant list, the patient's health status, and age. The most important part of the equation is that the kidney be compatible with the patient's body. A human kidney has a set of six antigens, substances that stimulate the production of antibodies. (Antibodies then attach to cells they recognize as foreign and attack them.) Donors are tissue matched for 0–6 of the antigens, and compatibility is determined by the number and strength of those matched pairs. Blood type matching is also important. Patients with a living donor who is a close relative have the best chance of a close match.
Before being placed on the transplant list, potential kidney recipients must undergo a comprehensive physical evaluation. In addition to the compatibility testing, radiological tests, urine tests, and a psychological evaluation will be performed. A panel of reactive antibody (PRA) is performed by mixing the patient's serum (white blood cells) with serum from a panel of 60 randomly selected donors. The patient's PRA sensitivity is determined by how many of these random samples his or her serum reacts with; for example, a reaction to the antibodies of six of the samples would mean a PRA of 10%. High reactivity (also called sensitization) means that the recipient would likely reject a transplant from the donor. The more reactions, the higher the PRA and the lower the chances of an overall match from the general population. Patients with a high PRA face a much longer waiting period for a suitable kidney match.
Potential living kidney donors also undergo a complete medical history and physical examination to evaluate their suitability for donation. Extensive blood tests are performed on both donor and recipient. The blood samples are used to tissue type for antigen matches, and confirm that blood types are compatible. A PRA is performed to ensure that the recipient antibodies will not have a negative reaction to the donor antigens. If a reaction does occur, there are some treatment protocols that can be attempted to reduce reactivity, including immunosuppresant drugs and plasmapheresis (a blood filtration therapy).
The donor's kidney function will be evaluated with a urine test as well. In some cases, a special dye that shows up on x rays is injected into an artery, and x rays are taken to show the blood supply of the donor kidney (a procedure called an arteriogram).
Once compatibility is confirmed and the physical preparations for kidney transplantation are complete, both donor and recipient may undergo a psychological or psychiatric evaluation to ensure that they are emotionally prepared for the transplant procedure and aftercare regimen.
Aftercare
A typical hospital stay for a transplant recipient is about five days. Both kidney donors and recipients will experience some discomfort in the area of the incision after surgery. Pain relievers are administered following the transplant operation. Patients may also experience numbness, caused by severed nerves, near or on the incision.
A regimen of immunosuppressive, or anti-rejection, medication is prescribed to prevent the body's immune system from rejecting the new kidney. Common immunosuppressants include cyclosporine, prednisone, tacrolimus, mycophenolate mofetil, sirolimus, baxsiliximab, daclizumab, and azathioprine. The kidney recipient will be required to take a course of immunosuppressant drugs for the lifespan of the new kidney. Intravenous antibodies may also be administered after transplant surgery and during rejection episodes.
Because the patient's immune system is suppressed, he or she is at an increased risk for infection. The incision area should be kept clean, and the transplant recipient should avoid contact with people who have colds, viruses, or similar illnesses. If the patient has pets, he or she should not handle animal waste. The transplant team will provide detailed instructions on what should be avoided post-transplant. After recovery, the patient will still have to be vigilant about exposure to viruses and other environmental dangers.
Transplant recipients may need to adjust their dietary habits. Certain immunosuppressive medications cause increased appetite or sodium and protein retention, and the patient may have to adjust his or her intake of calories, salt, and protein to compensate.
Risks
As with any surgical procedure, the kidney transplantation procedure carries some risk for both a living donor and a graft recipient. Possible complications include infection and bleeding (hemorrhage). A lymphocele, a pool of lymphatic fluid around the kidney that is generated by lymphatic vessels damaged in surgery, occurs in up to 20% of transplant patients and can obstruct urine flow and/or blood flow to the kidney if not diagnosed and drained promptly. Less common is a urine leak outside of the bladder, which occurs in approximately 3% of kidney transplants when the ureter suffers damage during the procedure. This problem is usually correctable with follow-up surgery.
A transplanted kidney may be rejected by the patient. Rejection occurs when the patient's immune system recognizes the new kidney as a foreign body and attacks the kidney. It may occur soon after transplantation, or several months or years after the procedure has taken place. Rejection episodes are not uncommon in the first weeks after transplantation surgery, and are treated with high-dose injections of immunosuppressant drugs. If a rejection episode cannot be reversed and kidney failure continues, the patient will typically go back on dialysis. Another transplant procedure can be attempted at a later date if another kidney becomes available.
The biggest risk to the recovering transplant recipient is not from the operation or the kidney itself, but from the immunosuppressive medication he or she must take. Because these drugs suppress the immune system, the patient is susceptible to infections such as cytomegalovirus (CMV) and varicella (chickenpox). Other medications that fight viral and bacterial infections can offset this risk to a degree. The immunosuppressants can also cause a host of possible side effects, from high blood pressure to osteoporosis. Prescription and dosage adjustments can lessen side effects for some patients.
Normal results
The new kidney may start functioning immediately, or may take several weeks to begin producing urine. Living donor kidneys are more likely to begin functioning earlier than cadaver kidneys, which frequently suffer some reversible damage during the kidney transplant and storage procedure. Patients may have to undergo dialysis for several weeks while their new kidney establishes an acceptable level of functioning.
Studies have shown that after they recover from surgery, kidney donors typically have no long-term complications from the loss of one kidney, and their remaining kidney will increase its functioning to compensate for the loss of the other.
Morbidity and mortality rates
Survival rates for patients undergoing kidney transplants are 95–96% one year post-transplant, and 91% three years after transplant. More than 2,900 patients on the transplant waiting list died in 2001. The success of a kidney transplant graft depends on the strength of the match between donor and recipient and the source of the kidney. According to the OPTN 2002 annual report, cadaver kidneys have a five-year survival rate of 63%, compared to a 76% survival rate for living donor kidneys. However, there have been cases of cadaver and living, related donor kidneys functioning well for over 25 years. In addition, advances in transplantation over the past decade have decreased the rate of graft failure; the USRDS reports that graft failure dropped by 23% in the years 1998–2000 compared to failures occurring between 1994 and 1997.
Alternatives
Patients who develop chronic kidney failure must either go on dialysis treatment or receive a kidney transplant to survive.
Resources
books
Cameron, J. S. Kidney Failure: The Facts. New York: Oxford University Press, 1999.
Finn, Robert, ed., et al. Organ Transplants: Making the Most of Your Gift of Life. Cambridge, MA: O'Reilly Publishing, 2000.
Mitch, William, and Saulo Klahr, eds. Handbook of Nutrition and the Kidney, 4th edition. Philadelphia: Lippincott, Williams, and Wilkins, 2002.
Parker, James, and Philip Parker, eds. The 2002 Official Patient Sourcebook on Kidney Failure. San Diego: Icon Health Publications, 2002.
University Renal Research and Education Associates (URREA); United Network for Organ Sharing (UNOS). 2002 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1992–2001. Rockville, MD: HHS/HRSA/OSP/DOT, 2003. http://www.optn.org/data/annualReport.asp. .
U.S. Renal Data System. USRDS 2002 Annual Data Report. Bethesda, MD: The National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2003.
periodicals
Waller, J. R., et al. "Living Kidney Donation: A Comparison of Laparoscopic and Conventional Open Operations." Postgraduate Medicine Journal 78, no. 917 (March 2002): 153.
organizations
American Association of Kidney Patients. 3505 E. Frontage Rd., Suite 315, Tampa, FL 33607. (800) 749-2257. info@aakp.org. http://www.aakp.org .
American Kidney Fund (AKF). Suite 1010, 6110 Executive Boulevard, Rockville, MD 20852. (800) 638-8299. helpline@akfinc.org. http://www.akfinc.org .
National Kidney Foundation. 30 East 33rd St., Suite 1100, New York, NY 10016. (800) 622-9010. http://www.kidney.org .
United Network for Organ Sharing (UNOS). 700 North 4th St., Richmond, VA 23219. (888) 894-6361. http://www.transplantliving.org .
United States Renal Data System (USRDS). USRDS Coordinating Center, 914 S. 8th St., Suite D-206, Minneapolis, MN 55404. (612) 347-7776. http://www.usrds.org .
other
Infant Kidney Transplantation. Lucille Packard Children's Hospital. 725 Welch Road, Palo Alto, CA 94304. (650) 497-8000. http://www.lpch.org/clinicalSpecialtiesServices/COE/Transplant/KidneyTransplant/infantAdultToinfantKidneyTransplant.html .
A Patient's Guide to Kidney Transplant Surgery. University of Southern California Kidney Transplant Program. http://www.kidneytransplant.org/patientguide/index.html .
Paula Anne Ford-Martin
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
A kidney transplant is performed by a transplant surgeon in one of more than 200 UNOS-approved hospitals nationwide. If the patient has no living donor, he or she must go through an evaluation procedure to get on the UNOS national waiting list and the UNOS Organ Center's UNet database.
QUESTIONS TO ASK THE DOCTOR
- How many kidney transplants have both you and the hospital performed?
- What are your transplant success rates? How about those of the hospital?
- Who will be on my transplant team?
- Can I get on the waiting list at more than one hospital?
- Will my transplant be performed with a laparoscopic or an open nephrectomy?
- What type of immunosuppressive drugs will I be on post-transplant?
regards,
pratik
I ahd a kidney Transplant about 5 years ago, but now i work in a cold warehouse is there any reasons why i can not work in a cold warehouse or is it ok to work in those conditions.
I would appreciate a quick response.
Thank you
I am a young man of 30years of age. and have been diagnose with chronic kidney disease. Please I do not have money for the dialysis or the transplanting.what should I do to extend my life, can reduction of salt,protein and others help? also i do have a many brothers can it be that i might have a match? Please do me a favor and advise me on what to do. hope to hear from you soon.
donating a kidney ,for my brother could give as much information for me as well as for him regarding kidney donation/transplant,
thanking you
Christine Mufford
Abdul Qadeer Shami
i would also like to know how long should he not meet with people after the transplant
Thanks.
i would also like to know how long should he not meet with people after the transplant
regards
vijay
i would also like to know how long should he not meet with people after the transplant
regards
vijay
My brother will undergo kidney transplant & he will receive a kidney from our mother after 15 days.
I would like to know more about what precautions we should take before & after the surgery.
Kindly advise us regarding life long precautions donor & receiver will have to take.
Also please inform me if smoking can cause any infection to the receiver ? My brother happens to be a chronic smoker.
I would like to know more about what precautions we should take before & after the surgery.
Kindly advise us regarding life long precautions donor & receiver will have to take.
i am getting a kidney from my mum and are more wanting to know what she will go through she is 40 and quiet active
My recovery was a little more complicated but my kidney function was at 5% before my surgery (never did go on dialysis) and was very sick, so I'm just saying that your recovery time and process depends on your over all health for the recepient AND the donor!
Good luck to you all and may God bless you!
Do you wish to sell your kidney in exchange of money? If yes.
Then contact Dr John Rooney today to get a reliable and good transaction for good money.
Contact email:dr.johnrooney@gmail.com
call me @ +918904592049