Tooth extraction
Definition
Tooth extraction is the removal of a tooth from its socket in the bone.
Purpose
Extraction is performed for positional, structural, or economic reasons. Teeth are often removed because they are impacted. Teeth become impacted when they are prevented from growing into their normal position in the mouth by gum tissue, bone, or other teeth. Impaction is a common reason for the extraction of wisdom teeth. Extraction is the only known method that will prevent further problems with impaction.
Teeth may also be extracted to make more room in the mouth prior to straightening the remaining teeth (orthodontic treatment), or because they are so badly positioned that straightening is impossible. Extraction may be used to remove teeth that are so badly decayed or broken that they cannot be restored. In addition, some patients choose extraction as a less expensive alternative to filling or placing a crown on a severely decayed tooth.
Demographics
Exact statistics concerning tooth extraction are not available. Experts estimate that over 20 million teeth are extracted each year in the United States. Many of these are performed in conjunction with orthodontic procedures. Some extractions are due to tooth decay.
Description
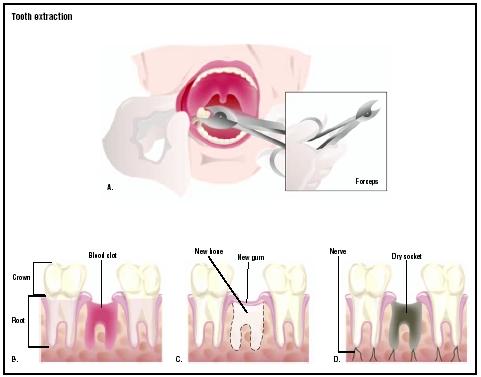
Tooth extraction can be performed with local anesthesia if the tooth is exposed and appears to be easily removable in one piece. The dentist or oral surgeon uses an instrument called an elevator to luxate, or loosen, the tooth; widen the space in the underlying bone; and break the tiny elastic fibers that attach the tooth to the bone. Once the tooth is dislocated from the bone, it can be lifted and removed with forceps.
If the extraction is likely to be difficult, a general dentist may refer the patient to an oral surgeon. Oral surgeons are specialists who are trained to administer nitrous oxide (laughing gas), an intravenous sedative, or a general anesthetic to relieve pain. Extracting an impacted tooth or a tooth with curved roots typically requires cutting through gum tissue to expose the tooth. It may also require removing portions of bone to free the tooth. Some teeth must be cut and removed in sections. The extraction site may or may not require one or more stitches (sutures) to close the incision.
Diagnosis/Preparation
In some situations, tooth extractions may be temporarily postponed. These situations include:
- Infection that has progressed from the tooth into the bone. Infections may complicate administering anesthesia. They can be treated with antibiotics before the tooth is extracted.
- Use of drugs that thin the blood (anticoagulants). These medications include warfarin (Coumadin) and aspirin . The patient should stop using these medications for three days prior to extraction.
- People who have had any of the following procedures in the previous six months: heart valve replacement, open heart surgery, prosthetic joint replacement, or placement of a medical shunt. These patients may be given antibiotics to reduce the risk of bacterial infection spreading from the mouth to other parts of the body.
Before extracting a tooth, the dentist will take the patient's medical history, noting allergies and other prescription medications that the patient is taking. A dental history is also recorded. Particular attention is given to previous extractions and reactions to anesthetics. The dentist may then prescribe antibiotics or recommend stopping certain medications prior to the extraction. The tooth is x rayed to determine its full shape and position, especially if it is impacted.
Patients scheduled for deep anesthesia should wear loose clothing with sleeves that are easily rolled up to allow the dentist to place an intravenous line. They should not eat or drink anything for at least six hours before the procedure. Arrangements should be made for a friend or relative to drive them home after the surgery.
Aftercare
An important aspect of aftercare is encouraging a clot to form at the extraction site. The patient should put pressure on the area by biting gently on a roll or wad of gauze for several hours after surgery. Once the clot is
For the first two days after the procedure, the patient should drink liquids without using a straw and eat soft foods. Any chewing must be done on the side away from the extraction site. Hard or sticky foods should be avoided. The mouth may be gently cleaned with a toothbrush, but the extraction area should not be scrubbed.
Wrapped ice packs can be applied to reduce facial swelling. Swelling is a normal part of the healing process; it is most noticeable in the first 48–72 hours after surgery. As the swelling subsides, the patient's jaw muscles may feel stiff. Moist heat and gentle exercise will restore normal jaw movement. The dentist or oral surgeon may prescribe medications to relieve postoperative pain.
Risks
Potential complications of tooth extraction include postoperative infection, temporary numbness from nerve irritation, jaw fracture, and jaw joint pain. An additional complication is called dry socket. When a blood clot does not properly form in the empty tooth socket, the bone beneath the socket is exposed to air and contamination by food particles; as a result, the extraction site heals more slowly than is normal or desirable.
Normal results
The wound usually closes in about two weeks after a tooth extraction, but it takes three to six months for the bone and soft tissue to be restructured. Such complications as infection or dry socket may prolong the healing process.
Morbidity and mortality rates
Mortality from tooth extraction is very rare. Complications include a brief period of pain and swelling; post-extraction infections; and migration of adjacent teeth into the empty space created by an extraction. Most people experience some pain and swelling after having a tooth extracted. With the exception of removing wisdom teeth, migration into the empty space is common. Braces or orthodontic appliances usually control this problem.
Alternatives
Alternatives to tooth extraction depend on the reason for the extraction. Postponing or canceling an extraction to correct tooth crowding will cause malocclusion and an undesirable appearance. Not removing an impacted wisdom tooth may cause eventual misalignment, although it may have no impact. Not removing a decayed or abscessed tooth may lead to septicemia and other complications.
See also Wound care .
Resources
books
Harris, N. O., and F. Garcia-Godoy. Primary Preventative Dentistry , 6th ed. Englewood Cliffs, NJ: Prentice Hall, 2003.
Peterson, L. J. Contemporary Oral and Maxillofacial Surgery , 4th ed. Amsterdam: Elsevier Science, 2002.
Scully, C. Oral and Maxillofacial Medicine: A Practical Guide. London, UK: Butterworth-Heinemann, 2003.
Tronstad, L. Clinical Endodontics. New York: Thieme Medical Publishers, 2003.
periodicals
Devlin, H., and P. Sloan. "Early Bone Healing Events in the Human Extraction Socket." International Journal of Oral and Maxillofacial Surgery 31 (December 2002): 641-645.
Magheri, P., S. Cambi, and R. Grandini. "Restorative Alternatives for the Treatment of an Impacted Canine: Surgical and Prosthetic Considerations." Practical Procedures and Aesthetic Dentistry 14 (October 2002): 659-664.
Moscovich, H. "Fitting Restorations from Extracted Teeth." Journal of the South African Dental Association 55 (August 2000): 411-412.
Rosted, P., and V. Jorgensen. "Acupuncture Treatment of Pain Dysfunction Syndrome After Dental Extraction." Acupuncture in Medicine 20 (December 2002): 191-192.
organizations
American Association of Oral and Maxillofacial Surgeons. 9700 West Bryn Mawr Ave., Rosemont, IL 60018-5701. (847) 678-6200. http://www.aaoms.org .
American Board of Oral and Maxillofacial Surgery. 625 North Michigan Avenue, Suite 1820, Chicago, IL 60611. (312) 642-0070; FAX: (312) 642-8584. http://www.aboms.org .
American Dental Association. 211 E. Chicago Avenue, Chicago, IL 60611. (312) 440-2500. http://www.ada.org .
British Association of Oral and Maxillofacial Surgeons, Royal College of Surgeons. 35–43 Lincoln's Inn Fields, London, UK WC2A 3PN. http://www.baoms.org.uk .
other
American Dental Association. [cited April 3, 2003]. http://www.ada.org/public/topics/extractions.html .
Bristol Biomed. [cited April 3, 2003]. http://www.brisbio.ac.uk/ROADS/subject-listing/toothextraction.html .
Dental Review Online. [cited April 3, 2003]. http://www.dentalreview.com/Tooth_Extraction.htm .
Emory University. [cited April 3, 2003]. http://www.emory.edu/COLLEGE/CULPEPER/RAVINA/PROJECT/Ancient_pages/Tooth_extraction.html .
L. Fleming Fallon, Jr., MD, DrPH
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
In 2003, teeth are most often extracted by maxillofacial or oral surgeons. Occasionally, a general dentist will extract a tooth. Teeth are most commonly removed in an outpatient facility adjacent to a hospital under general anesthesia.
QUESTIONS TO ASK THE DOCTOR
- Why are you suggesting a tooth extraction?
- What will my mouth look like after surgery?
- Is the oral surgeon board certified in maxillofacial surgery?
- How many teeth extractions has the oral surgeon performed?
- What is the oral surgeon's complication rate?
- Will I need medication after surgery?
Wayne Gower
I feel a pain from wisdom teeth
and Its been already 3 days, How long will this pain be and how much longer is it gonna be until my pain is gone??
Thanks.
I bled a hell of alot and it made my throat sore, but other than that everything was fine. I stopped bleeding the next day, however I am not sure if I dislodged the blood clot, my wife says that she sees the bone and for some reason my breath is horrible, but I dont feel any real pain. If I have dry socket, will it set in later?
a speedy reply would much be appreciated,
thanks janet.
The gum has healed superbly but i am left with what can only be described as shrapnal in the gum, this is so painful but i am told it is left over tooth from the extraction which will fall away over a time.If i touch it i can feel it almost like a splinter where the end stands up, but the skin is forming over. Anyone had this problem?
Thanks for any info.
Is it normal to still hurt this much and for breath to smell like a compost heap? I also drank quite a bit of alcohol last night, have I done an damage?
I want to go to the hair salon tomorrow (Saturday 3rd July) to get my hair washed, treated, and styled but my mom says thats not a good idea beause I shouldn't be going under any hair dryer or around heat after just recieveing to procedures. She says it's hazardous to my health. Is she right? Is it ok for me to go to the hair salon tomorrow?
I am going to a dentist where 2 friends have had several teeth removed, they are both males, and have afterwards had pieces of their teeth come out from the spot where they were removed. One of them had all of his top teeth pulled for dentures, and the other one just had a molar and wisdom tooth extracted. I am very worried if this is not normal, because I will be going to the same dentist as them, and I don't want it to happen to me if it is not normal!
Thank you!
the problem is that now, i have a big red balloon thing where one or the teeth was...
any ideas what it is? and what to do to get rid of it?
Thanks in advance
My BEST methods for dealing with the pain (which is a dull ache at best and a noticeable ache and soreness in my jaw that hinders activity at worst now) has been to overlap 800mg of ibuprofen and 500mg of acetaminophen every 8 and 5 hours, respectively.
You CAN overlap OTC pain meds with prescription pain meds but I'd check with your dentist if you're unsure of what you're doing. Vicodin contains acetaminophen, so no Tylenol with that- but ibuprofen would be safe, AND help with the swelling (which can remain for up to three days with no worry).
I can't take prescription narcotics- I'm in recovery for addiction to pain pills, so I'm going this the hard way!
I also rinse after every meal and irrigate with a plunger when available (less irritating then rinsing AND less risk to dislodge the clot! Ask your dentist for one!). Warm salt water was my dentists' recommendation and seems to work best. Cold water agitates the already agitated gums for me- avoid the cold.
Also! My sweet mother, taking pity on me, picked up a box of grape Cepacol Fizzlers one day after work. Not ONLY do they taste AWESOME (and they really do fizzle!), they work WONDERS on those poor, sore gums! When I wake up in pain, I use one now! It helps get me back to sleep quicker!
I haven't had a great lot of luck with either Oragel or Kanka gel. The Kanka brush has been nice though, very gentle application and no mess!
I bled a lot the first day, but after my appointment (I was sedated and under nitrous, for anxiety, mostly) I immediately went home and went to bed. I slept all day (from 3pm) through to the next morning (around 8am) with one middle of the night wake up to take pain meds.
SLEEP ON A TOWEL THE FIRST NIGHT UNLESS YOU PLAN TO BLEED ON YOUR PILLOW!
Yesterday was the FIRST night since the extraction that I've slept soundly all night, but I'm still in a fair amount of pain. I would advise getting on a set schedule of pain meds and setting an alarm for HALF AN HOUR before they're scheduled to wear off so you can take your next dose AND give it time to kick in.
AVOID hard foods and large bites. DO NOT CHEW ON THE EXTRACTION SIDE! NO CHEWING ICE! I've had a lot of luck with soft tacos (mostly bean and cheese), soft serve ice cream, simple or cream soups, spaghetti with sauce (no meat- cheese is wonderful), mashed potatoes and gravy, and sandwiches you can dip into soups to soften up (like a French dip).
And if all else fails, call your dentist! Extractions just hurt, unfortunately, but the pain of having the tooth pulled is SO much less then dealing with the long-term decay of a bad tooth- TRUST ME! I waited FIVE YEARS to have this one pulled.
If your tooth was already decaying, infected, or otherwise complicated, the pain might be a bit worse (mine had been decaying for so long I had only the top 1/3 of the crown and the filling left, hence my gum oversensitivity now, I'm also recovering from a gum infection).
It does get better, though, y'all. Promise. If you've made it this far, you're on the opposite side of that hill! Don't worry about getting to the bottom, just sit down and enjoy the sunset for a minute or two.
1-drink soda,2-smoke and finally eat anything besides
soup?I just had the extraction today.
I had a cracked/abscessed tooth that was pulled on Monday (April 26), and it is now Friday!
Monday was an extremely painful day for me! The tooth/jaw was so infected Novocain wasn't working properly to numb the extraction area, the dentist used two whole applicators on me too. To make it worse, when he pulled the tooth the top broke off leaving the root inside, he had to drill, remove tooth, drill, remove tooth. It was terrible. The doctor prescribed me 500 mg amoxicillin 3 times daily for 10 days and a heavy dosage of hydrocodone for pain, but even with painkillers the entire right side of my mouth was throbbing and aching the rest of the day.
I was told not to smoke (you really shouldn't, it's bad for the healing process) for at least 2 days but I smoke 1/2-1 pack a day depending on whether it's a good or bad day, and that day definitely was a bad day. I had about 5-6 cigarettes after I got home but only smoked them about halfway. I was worried about the clot so I soaked a gauze with my saliva before smoking and packed it down good against the socket while I smoked and when I was done removed it.
Tuesday I had a stiff jaw and mild pain, but painkillers helped me manage it pretty well. The clot was visible and well formed.
Wednesday to Thursday I panicked because it appeared that my socket was swelling and the clot was shrinking away!
Today I can now see why it would have looked that way. I now have a thin layer of skin over the clot, not at my gum line but a little deeper in the socket. I also have pain around the edges of the socket and shards of bone sticking out. It worried me at first but after some research I realize it's pretty normal.
I also think compared to others I'm severely lucky to have been smoking this whole time and be healing so well, especially considering a drill was used to get pieces of tooth out of the socket. Sometimes there is foul odor accompanied by a foul taste, but considering the extraction site was abscessed I'm pretty sure that's normal too and am not worried, especially because I am on antibiotics.
I'm no professional, but my advice to everyone is give the socket a week to heal, and if you are still in a lot of pain, discomfort, have lots of swelling, etc, go see your dentist because only he/she can give your answers to why you're having so many problems. If you have bone shards and you can't keep yourself from running your tongue over them or they are extremely uncomfortable, your dentist can remove them for you. Otherwise they should come out on their own eventually.
And to anyone getting a tooth extraction, don't let this experience of mine worry you! This is a tooth that had been cracked and abscessed for nearly two years because I'm a college student with unemployed parents and everywhere I called was $1800 or more for a root canal, and an extraction was $500 or more. I finally found a walk in clinic last week and it was $30 to be examined and another $30 to have the tooth pulled. I'm very thankful that places like that exist, but sad they are so hard for people who need it to find.
Back in 2006 I had a wisdom tooth pulled. Not impacted or anything, Xrays just showed my dentist that it was coming and he asked if I would like to have it pulled or if I'd like to wait and I told him to go ahead and pull it. It wasn't even painful, no swelling, nothing. Just took some time for my gums to heal up after being cut. So it goes to show the more problems your tooth is having, the more likely complications are to occur.
I know dental care is expensive and sometimes you feel like you can put it off, but the faster you get into a dentist's chair after a tooth chips or you feel a wisdom tooth coming in, the more pleasant your experience will be.
From what you have said it sounds like blood poisioning. Without treatment this will result in a very high chance of a heart attack or stroke.
go to the doc asap.
1st dentist wanted to wait 6-8weeks before inserting dentures
2nd dentist said he could do immediate.
I went with the 2nd but am curious what amount of time is normal for the procedure?
I don't think this guy is normal and question his practicing.
How long from 1shot of Novocain before begin extracting?
How long should it be to extract approximately 16 teeth?
How long should you sit in the chair before you are sent home?
does the dentist normally call to check on you?
I ask because I was in and out in under 45minutes
15min for numbing
15-20 afterwards
under 15 minutes for actual extraction.
This isn't normal isn't it? This is only one of 10 things that were not normal.
I am suffering hard because of these mistakes.
Would like to know what you think..
Thanks Kelly
As an encouragement to others... I was about as scared as scared can be, but it really was okay. Find a dentist that you trust and have confidence in. And, just do it. From one who knows... don't put off the work. It will only get worse and worse and will require more and more work to be done. Don't wait.
Blessings!
have not had much sleep. The holes seem to be closing but the pain is unbearable
what can I take to eliminate the pain? I was prescribed
ibuprofen but it isn't working I am taking advil liquigels but it seems
to only last a couple hours please help I literally can't
take this pain anymore!
I had all of my teeth out last Monday the 19th of May and my mouth is hurting so much is this normal slso whst foods can i eat
My 11 year old son has been seeing a dentist and orthodontist about his teeth.
He has two teeth in grown on the roof of his mouth. If has been strongly
recommended they be removed. Saw the surgeon specialist
to make the appointment. He advised that they cut open the roof
of the mouth (top palette) like a big flap remove teeth then stitch it
up with stitches coming through front gum above teeth. These
stitches dissolve. He told me he does hundreds of these ops. Has
anyone heard of ingrowns in the roof of the mouth removed like this?
The surgeon is in a reputable clinic but am just naturally worried for
my son and his mouth. Would appreciate experience feedback.
Many thanks!
Two days later I was rushed not hospital with
Septacimia now suffer with very bad salt low levels
I have to have them all out soon , and am very frightened
Any advice
Thanks .
for how many days this pain will continue. is there any remedy for it. is the above medicine have any side effect if taken for a long.
Please advise.
Hello everyone, I have been through tooth extraction many times before and I have dealt with Infected teeth having to be extracted. Today I had an appointment for getting my upper left, Infected back tooth pulled out. When we did the procedure first she put this numbing jell on my gums and waited for that to settle in. Next she gave me a shot (Fairly big) But it wasn't enough. So she ended up giving me 4 shots (I do well with needles and shots) It wasn't so bad, You could feel the pressure and it pinched quit a bit. After the shot she let that settle in for a couple minutes then she cleaned my mouth with water and a vacuum type thing that sucks in all water and infection (My infection was very bad and it starting oozing out liquid type stuff). After that she grabbed a tooth puller and just started wiggling it around. It didn't hurt at all, You just felt a bit of pressure, And in the end you don't even notice it's over. It was really quick and an okay procedure. Now I can't feel my tongue, gum or lip. It takes a few hours to ware down. But anywho, I hope this helped :) And I wish the best for all of you!
Did not help still the pains now however getting worse more and more from all that touching about by dentists. Eventual I found a dentist who looked at the x-rays and showed me that actual there is a fracture and clearly to see. Again x-ray and tooth extraction charge. It is now 7 month in total I am with pain now no longer from tooth as it is gone BUT in the bone. For all the 7 month I been on 5 different antibiotics, and still at present. To this day I am in pain now as explained in the gum/bone. No one can give me an answer and seem to belittle my situation. SO MUCH for DENTAL. I wish someone in the field of dentistry would know WHY the pain now has located itself to bone after the tooth has been pulled. It seem to be an infection as my body does do all the infection signs. ANYONE knows or has suggestion?
pulled 4 days ago i am a diabetic so it takes longer to heal but now the site is burbning and painful [i do smoke] but is this normal? thank you