Spinal fusion
Definition
Spinal fusion is a procedure that promotes the fusing, or growing together, of two or more vertebrae in the spine.
Purpose
Spinal fusion is performed to:
- Straighten a spine deformed by scoliosis, neuromuscular disease, cerebral palsy, or other disorder.
- Prevent further deformation.
- Support a spine weakened by infection or tumor.
- Reduce or prevent pain from pinched or injured nerves.
- Compensate for injured vertebrae or disks.
The goal of spinal fusion is to unite two or more vertebrae to prevent them from moving independently of each other. This may be done to improve posture, increase ability to ventilate the lungs, prevent pain, or treat spinal instability and reduce the risk of nerve damage.
Demographics
According to the American Academy of Orthopaedic Surgeons, approximately a quarter-million spinal fusions are performed each year, half on the upper and half on the lower spine.
Description
Spinal anatomy
The spine is a series of individual bones called vertebrae, separated by cartilaginous disks. The spine is composed of seven cervical (neck) vertebrae, 12 thoracic (chest) vertebrae, five lumbar (lower back) vertebrae, and the fused vertebrae in the sacrum and coccyx that help to form the hip region.
While the shapes of individual vertebrae differ among these regions, each is essentially a short hollow tube containing the bundle of nerves known as the spinal cord. Individual nerves, such as those carrying messages to the arms or legs, enter and exit the spinal cord through gaps between vertebrae.
The spinal disks act as shock absorbers, cushioning the spine, and preventing individual bones from contacting each other. Disks also help to hold the vertebrae together.
The weight of the upper body is transferred through the spine to the hips and the legs. The spine is held upright through the work of the back muscles, which are attached to the vertebrae.
While the normal spine has no side-to-side curve, it does have a series of front-to-back curves, giving it a gentle "S" shape. The spine curves in at the lumbar region, back out at the thoracic region, and back in at the cervical region.
Surgery for scoliosis, neuromuscular disease, and cerebral palsy
Abnormal side-to-side curvature of the spine is termed scoliosis. An excessive lumbar curve is termed lordosis, and an excessive thoracic curve is kyphosis. "Idiopathic" scoliosis is the most common form of scoliosis; it has no known cause.
Scoliosis and other curves can be caused by neuromuscular disease, including Duchenne muscular dystrophy. Progressive and perhaps uneven weakening of the spinal muscles leads to gradual inability to support the spine in an upright position. The weight of the upper body then begins to collapse the spine, inducing a curve. In addition to pain and disfigurement, severe scoliosis prevents adequate movement of air into and out of the lungs. Scoliosis also occurs in cerebral palsy, due to excess and imbalanced muscle activity pulling on the spine unevenly.
Idiopathic scoliosis, which occurs most often in adolescent girls, is usually managed with a brace that wraps the abdomen and chest, allowing the spine to develop straight. Spinal fusion is indicated in patients whose curves are more severe or are progressing rapidly. The indication for surgery in cerebral palsy is similar to that for idiopathic scoliosis.
Spinal fusion in Duchenne muscular dystrophy is usually indicated earlier than in otherwise healthy adolescents. This is because these patients lose ventilatory function rapidly through adolescence, making the surgery more dangerous as time passes. Surgery should occur before excess ventilatory function is lost.
Surgery for herniated disks, disk degeneration, and pain
As people age, their disks become less supple and more prone to damage. A herniated disk is one that has developed a bulge. The bulge can press against nerves located in the spinal cord or exiting from it, causing pain. Disks can also degenerate, losing mass and thickness, allowing vertebrae to contact each other. This can pinch nerves and cause pain. Disk-related pain is very common in the neck, which is subject to constant twisting forces, and the lower back, which experiences large compressive forces. In these cases, spinal fusion is employed to prevent the nerves from being damaged. The offending disk is removed at the same time. A fractured vertebra may also be treated with fusion to prevent it from causing future problems.
Sometimes, spinal fusion is used to treat back pain even when the anatomical source of the problem cannot be located. This is usually viewed as a last resort for intractable and disabling pain.
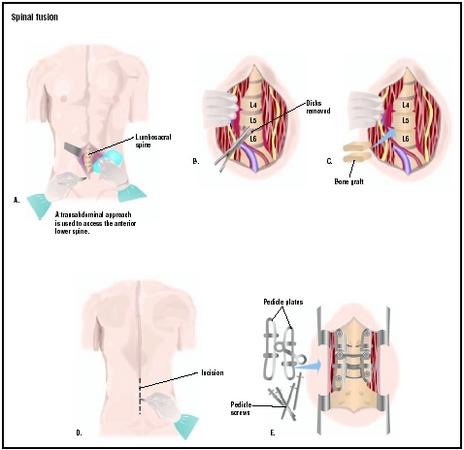
The spinal fusion operation
Spinal fusion is performed under general anesthesia. During the procedure, the target vertebrae are exposed. Protective tissue layers next to the bone are removed, and small chips of bone are placed next to the vertebrae. These bone chips can either be from the patient's hip or from a bone bank. The chips increase the rate of fusion. Using bone from the patient's hip (an autograft) is more successful than banked bone (an allograft), but it increases the stresses of surgery and loss of blood.
Fusion of the lumbar and thoracic vertebrae is done by approaching from the rear, with the patient lying face down. Cervical fusion is typically performed from the front, with the patient lying on his or her back.
Many spinal fusion patients also receive spinal instrumentation . During the fusion operation, a set of rods, wires, or screws will be attached to the spine. This instrumentation allows the spine to be held in place while the bones fuse. The alternative is an external brace applied after the operation.
An experimental treatment, called human recombinant bone morphogenetic protein-2, has shown promise for its ability to accelerate fusion rates without bone chips and instrumentation. This technique is only available through clinical trials at a few medical centers.
Spinal fusion surgery takes approximately four hours. The patient is intubated (tube placed in the trachea), and has an IV line and Foley (urinary) catheter in place. At the end of the operation, a drain is placed in the incision site to help withdraw fluids over the next several days. The fusion process is gradual and may not be completed for months after the operation.
Diagnosis/Preparation
A potential candidate for spinal fusion undergoes a long series of medical tests. In patients with scoliosis, x rays are taken over many months or years to track progress of the curve. Patients with disk herniation or degeneration may receive x rays, MRI studies, or other tests to determine the location and extent of injury.
Patients in good health may donate several units of their own blood in preparation for surgery. This may be done between six weeks and one week prior to the operation. The patient will probably be advised to take iron supplements to help replace lost iron in the donated blood. Sunburn or sores on the back should be avoided prior to surgery because they increase the risk of infection.
A variety of medical tests will be done shortly before surgery to ensure that the patient is in good health and prepared for the rigors of surgery. Blood and urine tests, x rays, and possibly photographs documenting the curvature will be done. An electroencephalogram (EEG) may be performed to test nerve function along the spine.
The patient will be admitted to the hospital the evening before surgery. No food is allowed after midnight, in order to clear the gastrointestinal tract, which will be immobilized by anesthesia.
Aftercare
The patient will stay in the hospital for four to six days after the operation.
Post-operative pain is managed by intravenous pain medication. Many centers use patient-controlled analgesia (PCA) pumps, which allow patients to control the timing of pain medication.
For several days after the operation, the patient is unable to eat or drink because of the lasting effects of the anesthesia on the bowels. Fluids and nutrition are delivered via the IV line.
The nurse helps the patient sit up several times per day, and assists with other needs as well. Physical therapy begins several days after the operation.
Most activities are restricted for several weeks. Strenuous activities such as bike riding or running are usually resumed after six to eight months. The surgical incision should be protected from sunburn for approximately one year to promote healing of the scar.
Risks
Spinal fusion carries a risk of nerve damage. Rarely, delayed paralysis can occur, probably from loss of oxygen to the spine during surgery. Infection may occur. Bone from the bone bank carries a small risk of infection with transmissible diseases from the bone donor. Anesthesia also poses risks. Unsuccessful fusion (pseudoarthrosis) may occur, leaving the patient with the same problem after the operation.
Normal results
Spinal fusion for scoliosis is usually very successful in partially or completely correcting the deformity. Spinal fusion for pain is less uniformly successful because the cause of the pain cannot always be completely identified.
Morbidity and mortality rates
Unsuccessful fusion may occur in 5–25% of patients. Neurologic injury occurs in less than 1–5% of patients. Infection occurs in 1–8%. Death occurs in less than 1% of patients.
Alternatives
Bracing and "watchful waiting" is the alternative to scoliosis surgery. Disk surgery without fusion is possible for some patients. Strengthening exercises and physical therapy may help some back pain patients avoid back surgery.
See also Bone grafting ; Disk removal .
Resources
books
Neuwirth, M.D., Michael. The Scoliosis Sourcebook. New York: McGraw-Hill, 2001.
periodicals
Robinson, Richard. "Setting the Record Straight." Quest Magazine 4, no.1 (1997). http://www.mdausa.org/publications/Quest/q41scoliosis.html
organizations
National Scoliosis Foundation. (800) NSF-MYBACK (673-6922). http://www.scoliosis.org .
Richard Robinson
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Spinal fusion is performed by an orthopedic surgeon or neurosurgeon in a hospital setting.
QUESTIONS TO ASK THE DOCTOR
- How long will hospitalization be necessary?
- Will patient-controlled analgesia (PCA) be used for pain?
- How soon can the normal regime of school or work be resumed?
- What outcome is expected?
- Is there an alternative to surgery?
I had an MRI done recently and it showed that two of my disc's were bulged. My doctor says I could have nerve damage.
will my pain get any better. Should I get the two other bulged disc's taken out. Please help.
Has the FDA approved its use?
Thank you...Roxanne
a article about Oklahoma Spine Hospital in Oklahoma City, Ok.
Speciality Hospitals rock, Steven Cagle surgeon at Olkahoma Spine
had enough balls to call Doc Sullivan a Corporate Prostitute after
hearing him attack speciality hospitals. Speciality Hospital
specialize I have Scheurman Syndrom, idiopathic scoliosis my back
is at 68% my lungs are being crushed, my legs hurt at times when
I want to scream. I'm a veteran from Desert Storm and always helped other people, live in Utah hope to go to OK soon Cheryl.
realities of successful surgery. I am an adult with scolios
at 50 degrees but otherwise in good systemic health. I have been
advised that minimially invasive will not work for me that
I need the full fusion from T10 to S1. The plan is to use the
XLIF for the cages from the side and the TLIF plus full fusion
in posterior.
Can you give me an idea of the amount of blood that would be lost
during surgery in terms of units??
Thank you.
q.is there any specalist therapy i should seek.
can i expecpt any improvement after so long without any
should i push myself and bear the pain for days aferwards.
i need the chair for mobility so that i can keep busy and contribute to the household chores like cooing and cleaning etc.please reply aqs i am desperate i look and feel very well and feel this detracts my medical overseerers from doing anything other than pain killers
regards major
let me explain to you my son situation my son with 6 years old he has scoliosis so this case need for many surgeries to recovery so that he has been done 6 surgeries till now (6_8 months between one surgery and another) and this case depend on the growing of the spine also I would like you to be informed that he has been done this surgeries out of Iraq in Arabic country they sponsors his case and suddenly they stop the treatment according to unknown reasons & for now we are in Iraq with the hard situation .so that we can't do the surgery to him In iRAQ , the last surgery to him was at :20 th _ dec_ 2009 so for the current time he so need to do the process therefore I need to your cooperation with me and provided me about the detail of the surgery included the total cost in dollar .and i have on other question if you could answer me about it
could he has one process to make his spine straight without needing to surgery every (6_8) months?
please found attached the reports and x_ray photos .
I am waiting for your answer to my mail
thanks ®ards
I am reaching out to you in hopes that someone out there may have gone through a spinal fusion then had the hardware taken out to help the pain from after the fusion. My fusion was done in November 2007 to correct Kyphosis. I now have two rods, 23 screws, and two hooks from under my shoulder blades pretty much throughout my entire spine. The pain since surgery is much better than the pain I had before surgery. However, I still have a lot of pain. My surgeon basically told me that he thinks the option to help would be to have the hardware removed. They are trying to pinpoint the pain areas and it's all pointing to the hardware. I've tried physical therapy, exercise, etc., and it doesn't seem to make a difference. I am 32 and the surgery was done long enough ago that the doctor said that having the hardware taken out won't affect anything and that it's been long enough where the spine should be fused (therefore making the hardware useless at this point). I am just afraid of my spine curve coming back down the road. I am also afraid that taking out the hardware will be like having the surgery all over again. Any advice? THANK YOU!
I had injuried my back in 2006 and I broke 4 vertebrals. Two in my neck and two in my back. They did operate on T-9 AND T-10 . What happen was that on one of my vertabrals they did a vertaplasy and on the other one they were only able to take out the pieces. So here is my question are they able to stop all of the pain that I'm dealing with. Right now I have to take 4 different types of pain medications a total of about 12 pills everyday now. Oh also do to operating on my back they did something to cause me to have pain in my legs also . If there is a operation that will take away the pain and give me back my life what will it cost? And can it be done on Medicare?
I have seen lots of doctors but half say I need another surgery and the other alf say I dont. What shoul I do?
This is the information on the surgery I will be having. My only concern is the bone needed. It says that they can use a bone from a cadaver. Any thoughts???
MY ADVICE: PHYSICAL THERAPY!!! STAY WITH IT
My thumb now seems to move all night which is making it worse any idea why?
Looking for advice. I am very busty on top and I am sure that doesnt help either. Please help me with what to do I am sometimes afraid to move. I am not in pain when I sit which is making me lazy. Cant walk very far at all. Help
Now 2012 and i'm scheduling fusion to have remainder of lumbar fused with instrumentation. It is a relief to be getting the rest of the lumbar fused am willing to go through the post-op pain to get to a point in life that will need no pain meds and hope of going thru life without pain. Having had very successful fusions i am very fortunate to have had success.
I'd spent three years on disability with agonizing pain after two failed laminectomies, by doctors who could only be described as hacks who barely get thru the day without crippling someone.
I went to a spinal surgeon on a Friday and had a discectomy and spinal fusion on the next Monday. The fusion is at L3-4.I have a few questions that I am curious about. My surgeon told me that doing a bone implant is old school and he uses a cement like substance where the disc was removed. I researched this and couldn't find any information about this. The numbness in my knee and leg is still there six weeks after surgery. The doctor told me that it will take about two months for the nerve to regenerate and it should go away. I'm skeptical about this and have heard stories that it may never stop being numb. Can anyone provide some insight concerning my questions. Aside from the numbness, I still have the grion pain which on occassion feels like a hernia ( had left and right ilioinguinal hernia sugery) in 2005.Other than that, I can walk and have no other pain which I feel lucky about.
Thank you for all your help
Allan
I have a request.
Our lab works on technology that allows, among other things, to reduce Ti spinal rod diameter by 0.5 to 1 mm. There are some benefits on personal and industrial levels. My request pertains to industrial level: could somebody suggest how I can get an estimate on savings in material?
Thank you.
Any advice appreciated.
PROBLEM I HAVE IS PAIN IN THE LEFT LEG WHEN STANDING. ANY ADVICE. THANK YOU.RUBY SOUWITZSKY.
For everyone else reading here : FUSION SHOULD BE THE VERY LAST THING YOU TRY!! I can't stress this enough! I've been extraordinarily lucky with my fusion, but then I had a fantastic neurosurgeon (Prof Graeme Brazenor, Epworth Hospital, Melbourne) and a wonderful pain management team. However, because of the stress fusion places on the joints above and below the fused area, you WILL need to manage your health, and you MUST strike up a good relationship with your surgeon, your doctor, and your radiologist. It's difficult to do this in Australia, but it's possible.
Keep aware of your limitations, don't think that the fusion will fix everything, and let your doctor know when you're having trouble with pain. It's far better to have a hundred X-rays or MRIs than to just put up with the pain. Get involved - learn about the spine, learn about pain and pain management, and if you can, get your GP or doctor to recommend a multi-disciplinary team to work with you.
You might also like to consider hypnosis, and I'm also working on some other therapies, but because I"m not a doctor, I'm having trouble getting medical specialists on board (old boys syndrome, unfortunately). I'll try posting back here when I have more info. In the meantime, check out my blog - cephasatheos.wordpress.com, and feel free to discuss, comment, and I'll do my best to offer suggestions and advice. Stay positive if you can, and lean on your friends.
pluresey, which is the fluid between your ribs and the lining of your rib cage. Mine is GONE from the lung surgery . So the best way to describe that pain is *wicked*. Does anyone have any advice for me?
I do not understand all the terms that are being used on here I just know that she has a 60% top and 55% lower.
But this may be more when we see him this week coming.
The surgeon has said he will save the bottom 3 discs does anybody know what this means in terms of T1 - T5 he said just below the bra line I am so confused.
She was at a full time theatre school and just finished her GCSE now due to start college to do Art A level as no drama
college will touch her now.
I am worried sick about this as she is a very young 16 year old and I do not think she has a clue about the hole entire thing.
Can anybody please maybe explain what some of the terms mean and is there anybody about the same age on this forum that is
in a similar position.
Thank you
Jane
Regards
Jane
Has anyone else out there had these type of problems after a spinal fusion - or is it just coincidence? I was fit and healthy before my fusion in 2005.
It's traction, for separation of vertebrae to decompress disc, to regenerate it. Make the disc reshape itself.
Learn about "Lateral Raphe" (L2-L5) in the Thoracolumbar Fascia Lumbar Spine. This is part of your "Internal weight belt". The other part is "Transverse abdominal" which is fascia connection under your 6-pack of muscle. When you pick up weight, Lateral Raphe, starts working to stabilize your core. It tightens & pulls on your lumbar spine(spinous process), squeezing your disc. Overtime our disc wear out and start to bulge. You know what happens after that.
...new Fascia bio-science and Thoracolumbar Fascia based bio-mechanics are being tested to understand causes and bio-mechanics to abolish low back, sciatica symptoms, subluxation, reshape a bulging disc by regeneration of IVD.
Google Dr. Robert Schleip, PhD fascia researcher.
Twitter @SelfDecompress for Lx fascia based bio-mechanics
There seems to be real hope in reducing our LBP, with or w/out failed fusion surgery.
I have read/listened to you over the years about your past & present pain. From what I know now. Avoid spine surgery by educating yourself about spinal decompression. Then catch up on Fascia & Thoracolumbar fascia and what it does and learn how to relax & release it!!
Hope & a leap of faith in mind body bio-mechanics,
d.
Sincerely Fidencio A. Perez
Due to the surgery, my left leg has had a cramp. Imagine living 14 years with a "Charlie Horse" in your leg 24/7. My back pain is much worse than before the operation, and now I am being told that due to so many meds for so long, it is now effecting my liver. At last count, they told me I have been on over 139 different types of pain meds.
I did not know there were that many to tell the truth. I would Never go through that again, and would only advise having that surgery only if it were a life and death situation.
Also, after my surgery, I had cancer surgery, lung surgery, and three years ago a stroke, which made my walking even more difficult
is almost like where my stomachs is yuke! Makes it look fat. What can I do about it?
All surgery does not turn out poorly and if you need it get it.
My mother had spine fusion surgery 4 days back and it was supposed to be L5-S1 fusion, but it seems they did L4-L5 and L5-S1 fusion and surgery took about 8 hours. What is bothering me is that they have used 3 screws on side and 2 screws on one side (Total 5 screws) and when I asked surgeon, he said yes that they have used 5 screws, is it correct to have unequal number of screws on two side, please reply ASAP