Bone grafting
Definition
Bone grafting is a surgical procedure that places new bone or a replacement material into spaces between or around broken bone (fractures) or in holes in bone (defects) to aid in healing.
Purpose
Bone grafting is used to repair bone fractures that are extremely complex, pose a significant risk to the patient, or fail to heal properly. Bone grafting is also used to help fusion between vertebrae, correct deformities, or provide structural support for fractures of the spine. In addition to fracture repair , bone grafting is used to repair defects in bone caused by congenital disorders, traumatic injury, or surgery for bone cancer. Bone grafts are also used for facial or cranial reconstruction.
Demographics
Degenerative diseases of the spine increase with age. People over age 50 are more likely to need a bone graft if their condition requires surgery. Traumatic injuries occur most often in people 18–44 years.
Description
Bone tissue is a matrix-like structure primarily composed of a protein called collagen. It is strengthened by hydroxyapatite, deposits of calcium and phosphate salts. Four types of bone cells are located within and around this matrix. Together, these four types of cells are responsible for building the bone matrix, maintaining it, and remodeling the bone as needed. The four types of bone cells are:
- Osteoblasts, which produce the bone matrix.
- Osteocytes, mature osteoblasts that maintain the bone.
- Osteoclasts, which break down and remove bone tissue.
- Bone lining cells, which cover bone surfaces.
There are three ways that a bone graft can help repair a defect.
- Osteogenesis, the formation of new bone by the cells contained within the graft.
- Osteoinduction, a chemical process in which molecules contained within the graft (bone morphogenetic proteins, abbreviated as BMP) convert the patient's cells into cells capable of forming bone.
- Osteoconduction, a physical effect whereby the graft matrix configures a scaffold on which cells in the recipient form new bone.
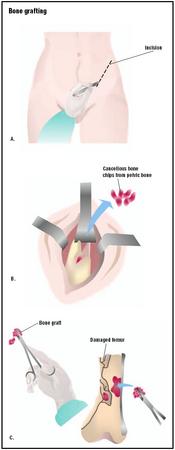
The term "graft" commonly refers to an autograft or allograft. A graft made of bone from the patient's own body (e.g., hip bones or ribs) is an autograft. To obtain a piece of bone for an autograft, the patient undergoes surgery under general anesthesia. An incision is made over the crest of the hip bone, a piece of bone is removed, and the incision is stitched closed.
An allograft uses bone from a cadaver, which has been frozen and stored in a tissue bank. Allografts are used because of the inadequate amount of available autograft material, and the limited size and shape of a person's own bone. Bones for allografts are usually available from organ and tissues donated by healthy people who die unexpectedly. Occasionally, allograft bone may be provided by a living donor. Allograft bone is commonly used in reconstructive surgery of the hip, knee, and long bones, as well as cases of bone loss due to trauma or tumors. Using allograft tissue from another person eliminates the need for a second operation to remove autograft bone or tendon. It also reduces the risk of infection, and safeguards against temporary pain and loss of function at or near the secondary site.
To place an autograft or allograft, the surgeon makes an incision in the skin over the bone defect, and shapes the bone graft or replacement material to fit into it. After the graft is placed into the defect, it is held in place with pins, plates, or screws. The incision is stitched closed, and a splint or cast is often used to prevent movement of the bones while healing.
After the bone graft has been accepted by the body, the transplanted bone is slowly converted into new living bone or soft tissue, and incorporated into the body as a functional unit.
Bone grafts for spinal fusion
In surgery of the spine, especially spinal fusion , (also called arthrodesis), surgeons may decide to use bone grafts to assist in the healing and remodeling of the spine after surgery. Normally, small pieces of bone are placed into the space between the vertebrae to be fused, and sometimes larger solid pieces of bone provide immediate structural support. Spinal fusion involves the surgical treatment of abnormalities in the vertebrae, such as curvatures, scoliosis or kyphosis, or injuries (fractures). Bone grafts may be used in spinal fusion surgery involving the lower (lumbar) or upper (cervical) spine. Cervical spinal fusion joins selected bones in the neck.
Diagnosis/Preparation
The surgeon does a clinical examination, and conducts tests to determine the necessity of a bone graft. Diagnostic tests determine the precise location of damage. These tests include x rays, magnetic resonance imaging (MRI), and computed tomography (CT) scan. They provide an image of the affected area, and indicate the exact amount of damage that has occurred due to the fracture or defect.
Orthopedic surgeries pose varying degrees of difficulty. The patient is instructed on what will take place during the procedure, as well as risks involved. A consent form is obtained before surgery.
The following activities will help the patient prepare for surgery.
- thorough physician consult before surgery
- banking some of his or her own blood in case a transfusion is needed
- eating well to achieve good nutritional status before and after surgery
- following a recommended exercise program before and after surgery.
- maintaining a positive attitude
- smoking cessation
Aftercare
Pain is normal for a few days following surgery, and medication is given regularly to alleviate this problem. The patient will likely have a urinary catheter.
The time required for convalescence after bone grafts due to fractures or spinal fusion varies from one to 10 days. Vigorous exercise may be limited for up to three months. Children heal faster than adults.
If a spinal fusion was performed, the patient may be discharged from the hospital with a back brace or cast. The family will be taught how to provide home care for the patient. A splint or cast prevents injury or movement while healing.
Risks
The risks for any surgical procedure requiring anesthesia include reactions to the medications and breathing problems. Bleeding and infection are also risks of surgery.
There is little risk of graft rejection for autografts, but there are drawbacks:
- additional surgical and anesthesia time (typically 30 minutes per procedure) to obtain or harvest the bone for grafting
- added costs for the additional surgery
- pain and infection at the site from which the graft is taken
- the relatively small amount of bone available for grafting
- surgical complications, such as infection and pain that sometimes last a longer period of time than the primary surgery (up to two years)
Allografts also have drawbacks:
- Bone variability because it is harvested from a variety of donors.
- Grafted bone may take longer to incorporate with the host bone (than in an autograft).
- Graft may be less effective than an autograft.
- Possibility of transferring diseases to the patient.
- Potential immune response complications (patient's immune system fighting against the grafted bone tissue). This problem is lessened through the use of anti-rejection drugs.
Normal results
Most bone grafts are successful in helping the bone defect to heal. The extent of recovery depends on the size of the defect and the condition of the bone surrounding the graft at the time of surgery. Severe defects take some time to heal, and may require further attention after the initial graft. Less severe bone defects should heal completely without serious complications. Repeat surgery is sometimes required if the condition recurs or complications develop.
If the bone graft is done on the face or head, the surgeries usually result in a more normal appearance.
Morbidity and mortality rates
Although bone harvested from the patient is ideal, postoperative morbidity is sometimes associated with hip bone or fibula (part of the knee) autografts. Morbidity of allografts is usually related to the graft incorporating more slowly, and less completely, into the body.
In one study of over 1,000 patients who received very large allografts after bone cancer surgery, researchers found that approximately 85% were able to return to work or normal physical activities without crutches. However, approximately 25% required a second operation because the first graft did not heal properly.
Infections associated with bacterial contamination of allografts are rare. However, they can result in serious illness and death.
Alternatives
Despite the increase in the number of procedures requiring bone grafts, there is no ideal bone graft substitute. However, there are a variety of natural and synthetic replacement materials used instead of bone, including collagen (the protein substance of the white fibers of the skin, bone, and connective tissue); polymers, such as silicone and some acrylics; hydroxyapatite; calcium sulfate; and ceramics. Several new products are available or in development. They function as bone graft substitutes or extenders. Demineralized bone matrix (bone that has had its calcium removed) possesses some of the properties that the body uses to induce bone formation. Calcium hydroxyappetite products or coral have structures similar to bone, and act as scaffolding for new bone.
New BMP products are expected to be strong inducers of bone growth (osteoinductive). These new products will be relatively expensive, but will grow bone better than the patient's own bone, eliminating the need for bone graft harvesting. Bone morphogenetic proteins have been extracted from natural tissues and produced in the laboratory to stimulate bone production in animals and humans. Because they do not have the same drawbacks as grafts, surgeons are hopeful that they will soon be able to use BMP and laboratory produced BMP to aid in the generation and repair of bone.
The INFUSE Bone Graft (rhBMP-2) has received Food and Drug Administration approval, and has demonstrated better patient outcomes than hip autografts with regard to length of surgery, blood loss, hospital stay, reoperation rate, median time to return to work, and fusion rates at six, 12, and 24 months following surgery.
Advances in tissue engineering have provided polymer based graft substitutes with degradable, porous, three-dimensional structure. New bone may be grown on these products; the grafts then slowly dissolve, leaving only the new bone behind.
See also Disk removal .
Resources
books
Beauchamp, Daniel R., M.D., Mark B. Evers, M.D., Kenneth L. Mattox, M.D., Courtney M. Townsend, and David C. Sabiston, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 16th edition. London: W B Saunders Co., 2001.
Branemark, Per-Ingvar, Philip Worthington, Kerstin Grondahl, and Christina Darle, eds. Osseointegration and Autogenous Onlay Bone Grafts: Reconstruction of the Edentulous Atrophic Maxilla. Chicago, IL: Quintessence Pub Co., 2001.
Laurencin, Cato T., ed. Bone Graft Substitutes. West Conshohocken, PA: American Society for Testing and Materials, 2003.
Lawrence, Peter F., Richard M. Bell, and Merril T. Dayton (Editors). Essentials of General Surgery. 2nd edition. Philadelphia, PA: Lippincott, Williams & Wilkins, 2000.
Lindholm, T. Sam, ed. Advances in Skeletal Reconstruction Using Bone Morphogenetic Proteins. River Edge, NJ: World Scientific Publishing Co., Inc., 2002.
periodicals
Berg-Johnsen, J., and B. Magnaes. "Rib Bone Graft for Posterior Spinal Fusion in Children." Acta Orthopaedica Scandinavic 73, no.9 (December 2002): 260-7.
Cowan, N., J. Young, D. Murphy, and C. Bladen. "Double-blind, Randomized, Controlled Trial of Local Anesthetic Use for Iliac Crest Donor Site Pain." Journal of Neuroscience Nursing 34, no.4 (August, 2002): 205-10.
Kakibuchi, M., K. Fukuda, N. Yamada, K. Matsuda, K. Kawai, T. Kubo, et al. "A Simple Method of Harvesting a Thin Iliac Bone Graft for Reconstruction of the Orbital Wall." Plastic Reconstruction Surgery 111, no.2 (February 2003): 961-2.
Nelson C. L., J. H. Lonner, J. A. Rand, and P.A. Lotke. "Strategies of Stem Fixation and the Role of Supplemental Bone Graft in Revision Total Knee Arthroplasty." Journal of Bone and Joint Surgery American volume. 85-A Suppl 1 (2003): S52-7.
organizations
American Association of Tissue Banks. 1350 Beverly Road, Suite 220-A, McLean, VA. 22101. (703) 827-9582, fax: (703) 356-2198. E-mail: aatb@aatb.org. http://www.aatb.org/menu.htm .
National Institutes of Health. 9000 Rockville Pike, Bethesda, MD. 20892. (301) 496-4000. Email: NIHInfo@OD. NIH.GOV. http://www.nih.gov/ .
North American Spine Society. 22 Calendar Court, 2nd Floor, LaGrange, IL 60525. (877) Spine-Dr. E-mail: info@ spine.org. http://www.spine.org .
other
American Academy of Orthopaedic Surgeons (AAOS) and American Association of Tissue Banks (AATB). "What Can You Tell Me About Bone and Tissue Transplantation?" 2001. [cited March 19, 2003]. http://orthoinfo.aaos.org/brochure/thr_report.cfm?Thread_ID=53&topcategory=About%20Orthopaedics&all=all .
U.S. National Library of Medicine and the National Institutes of Health. MEDLINE plus Health Information. 2003 [cited March 13, 2003]. http://www.nlm.nih.gov/medlineplus/html .
Lisa Christenson, Ph.D. Crystal H. Kaczkowski, M.Sc.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Bone grafts are performed by orthopedic surgeons, neurosurgeons, craniofacial surgeons, and periodontists. These physicians have specialized training in their field of expertise. They have completed additional education beyond a general medical residency. A physician becomes board certified after completing training in a specialty area, passing examinations, and meeting certification requirements. To become certified, the physician must:
- Complete the education required for a medical doctor or doctor of neurosurgery.
- Complete three to seven years of training in a residency program in the specialty field.
- Pass a written, and sometimes an oral, test given by the specialty board.
- Prepare for periodic recertification (required in most fields).
Specialty boards certify that physicians have met certain standards. Not all specialists are certified; certification is voluntary.
The surgeon and his or her surgical team will perform the surgery in a hospital on an inpatient basis.
QUESTIONS TO ASK THE DOCTOR
- What should be done prepare for the graft?
- Who will provide education about the grafting process?
- How many attending surgeons are available to do this type of surgery?
- How long is hospitalization necessary?
- How long will recovery take?
- When will it be safe to resume normal activities?
thanks ...
I have had a radial osteotomy with an allograft 6 weeks ago, and have been running a low grade fever for at least the last month. Radiograft taken today showed graft appears to be gone and a large black space has appeared since radiograph taken a month ago. The doc didn't mention it, or the fever I reported by phone two weeks ago. Operated area is one degree over other side when taking temp of skin.
Where do I go from here?? Where are the specialist that deal with bone graphs gone bad?
Since then he has had severe rash like welts on his back, legs, head, lips, face, genitals, And the list goes on and on. Several trips to ER to no avail.
His Dr. has diagnosed it as an allergic reaction to the Titanium hardware, and that after 6 mos
the hardware can be removed. WTF! I know that it has to be from the cadaver bone graft. Who in their right mind would consider putting cadaver parts into an alive and healthy person? Totally MORBID! Hopefully your husband doesn't have the same problems as mine.
I had a l-4-S1 lumbar fusion w/ titanium and cadaver bone. The site where they placed the cadaver bone actually fused faster than the titanium. Many people in the medical field use cadaver bones and it is standard practice if one can not get enough bone from the pt. I am thankful to the person who donated their bones to help my unhealthy ones. I am in the medical field and have never heard of a complication directly related to the placement of a cadaver bone.
I am 14 month out of my surgery and i am worse then i was before. I still cannot sit back in chairs, sofas hard to drive it hurts terribly. I cannot stand straight nor can i walk well without pain going thru my lower back hips and down both legs. As far as the bone graph i have alot of pain from it not even my pain pills help. They say everyone goes thru it different but i would research it more before you have it done. It is such a risk.
I design knee joint
KENT PARIS
Jenny
rgds
Please read article about bone graft, especially, the BMP at the bottom of the first article.
P.S. My uncle had the surgery before he had kids.
you have the right to a second, 3rd opinion life is nothing without your health, stop worrying about work and take your time oir Father in Heaven haven't forsaking me I was getting a divorce at the same time all this happen and living with less than $1000 with my 2 year boy and until now we had food a roof over our heaf and just as I was working, we take our life for granted we trust more in men which are not perfect than our own creator who feeds the birds and the beast in the fielfd, tell your husband to take his time and not rush, I wish I can go nack on time, but is late for me, life is much more than a job, blessings.
to go for the entire sciatica and up, how far I'm not even sure. Only for the fact I feel I'm going to wait till I DROP
before I let them touch me any more! Reading everyones posts is so sad, we are all connected by the pain that we are left in
by the very people who promise "DO NO HARM", but it must be ok to leave us in unexplained pain forever. If you do seek some
kind of solace in treatment (meds) oh, my God, you're an addict! Well, I didn't to this to myself, some highly educated, highly payed, Dr. told me he could make me better, that he did these surgeries all the time, well maybe he just had his first bad day when they gurnied me into the OR that morning,I'll never know but my life is focused on dealing with pain,
the hip which alot of you talk about, but no Dr. I found acknowledges unles it's the ball and socket.My iliac crest, the
harvest place of choice just fell completely apart, and left a gaping visable through the flesh hole. No one feels responsible so now what? Another lawyer, another opinion, another fight for something someone else did to me.. I believe your own bone is the best to use, after that who knows pick you poisin
Work for me or that bpm
a bone graft. My anklefeels bowling ball is resting
On my foot.why would my ankle feel so bad
Top of the knee pain!! Can someone help is this normal??
1.what is good thing or exercise to me after bone grafting.
2.how much time period required when I'll walked.
3.how much time required to heal.
4.can you give diet chart.
Note: i m smoker and 6 to 10 cigrate is my habit in a day.
I am in misery.
NOONE wILL intervene because NO ONE knows what to do if they run into hydroxyappetite while repeating a root canal or even trying to get tooth number out. I have suffered for 4 yearsbecssue no one agrees and they are all in political compteiton.
After 4 years of unhelped mouth infection I just got DIABETES.
Now my surgeon at Richmond Dental School and Blacksburg vA said he never operated on me though I have a letter to a lawyer sayig he did and all his hand written surgical note.
Who could I see anywhere in the uSA who could clean up my hydroxyappetite and repeat root canal that is leaking. Even taking tooth out. I have been told I am "a crock" more than once. How can I findout if my surgeon is certified in bone graftig which
ruined my life since 1989, I cannotkiss or bite a bagel.Worse they stick togeter circing their wagons and won't even see me orreturn my calls. Carol Munschauer PHD Buffaalo Ny
I have had an Osteotomy, bone graft surgery in Germany back in 1981 after a severe car accident, to correct the movement of the right hand. After all the pain and suffering, there was ZERO success. But the pains continue until today. The surgeon told me that pains will continue for the rest of life. I find this bizarre and difficult to understand.
Any one knows about ways to reduce or eliminate the continuous pains, apart from pain killers? I am 70 years old.
Thanks
Ed
Berlin
Germany
Now my question is now 7 1/2 months has been over if I walk along with nail without reunion of the bone whether it will break or not. and another question is the only remedy available with me is bone craft or some other remedy.
Third question is what are problem I have to face after bone craft and how many days i have to take rest.
Could you please clarify on my below query,
For a Right forntal bone skull tuberculosis patient, whether a surgery is must inorder to remove the Tuberculosis bone lesion existing in skull? or Anti Tuberculosis Medicine treatment/chemotheraphy would be sufficient in-order to clear the lesion existing in the skull?
A surgery is required or not in this case,Kindly please confirm?
BEFORE I HAD THE SURGERY I REALLY WAS'NT SURE WHAT WAS GOING TO DONE, BUT YOUR SITE HELPED ME UNDERSTAND IT,THANK YOU.
SINCERELY.
Is Bone graft better off for younger people? True??
Which one should be done, bone graft or knee replacement?
I am a bit confused with two different recommendations, but I am leaning on knee replacement surgery due to my age of 70.
Any advices would help. Thanks
My question is do i need a physical therapy after few months? Thanks in advance.