Rotator cuff repair
Definition
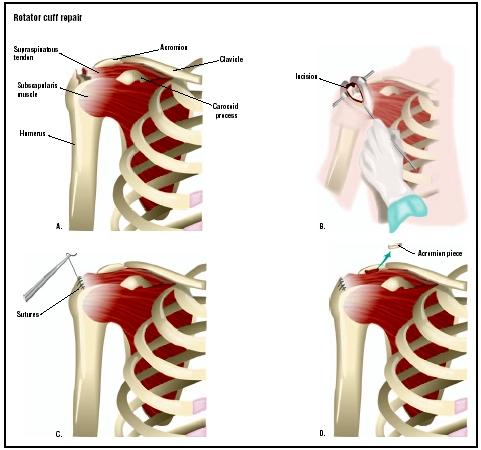
Rotator cuff surgery is the repair of inflammation or tears of the rotator cuff tendons in the shoulder. There are four tendons in the rotator cuff, and these tendons are attached individually to the following muscles: teres minor, subscapularis, infraspinatus, and the supraspinatus. The tears and inflammation associated with rotator cuff injury occur in the region near where these tendon/muscle complexes attach to the humerus (upper arm) bone.
Purpose
Rotator cuff surgery is necessary when chronic shoulder pain associated with rotator cuff injury does not respond to conservative therapy such as rest, heat/ice application, or the use of non-steroidal anti-inflammatory drugs (NSAIDs). Rotator cuff injuries are often lumped into the category referred to as rotator cuff syndrome. Rotator cuff syndrome describes a range of symptoms from basic sprains and tendon swelling (tendonitis) to total rupture or tearing of the tendon.
Demographics
Approximately 5–10% of the general population is believed to have rotator cuff syndrome at a given time. It is not commonly found in individuals under the age of 20 years, even though many in this population are athletically active. In general, males are more likely than females to develop rotator cuff syndrome and require surgery. Most rotator cuff injuries are associated with athletic activities such as baseball, tennis, weight lifting, and swimming, where the arms are repeatedly lifted over the head. Rotator cuff injuries can also occur in accidents involving falling to the ground or when the humerus is pushed into the shoulder socket. Rotator cuff injuries can also occur in older, active individuals because the rotator cuff tendons begin to deteriorate after age 40. Occupations that have been associated with rotator cuff injuries include nursing, painting, carpentry, tree pruning, fruit picking, and grocery clerking.
Description
For most patients, if the pain begins to subside, they are encouraged to undergo a period of physical therapy. If the pain does not subside after a few weeks, then the physician may suggest the use of cortisone injections into the shoulder region. Rotator cuff repair is then considered if the more conservative methods are not successful.
The primary aim of rotator cuff repair is to repair the connection between the damaged tendon and the bone. Once this bridge is re-established and the connection between the tendon and the bone has thoroughly healed, the corresponding muscles can once again move the arm in a normal fashion. The goal of the surgery is to ensure the smooth movement of the rotator cuff tendons and bursa under the upper part of the shoulder blade. The surgery is also performed to improve the comfort of the patient and to normalize the function of the shoulder and arm. There are a variety of surgical approaches that can be used to accomplish rotator cuff repair. The most common approach is called the anterior acromioplasty approach. This approach allows for excellent access to the most common sites of tears—the biceps groove, anterior cuff, and the undersurface of the joint.
Most rotator cuff repairs are accomplished using incisions that minimize cosmetic changes in the skin following healing. If possible, the surgery is performed with an arthroscope to minimize cosmetic damage to the skin. Typically, the incision made is about the size of a buttonhole. The arthroscope, a pencil-sized instrument, is then inserted into the joint. The surgeon usually accesses the rotator cuff by opening part of the deltoid muscle. If bone spurs, adhesions, and damaged bursa are present in the rotator cuff region, then the surgeon will generally remove these damaged structures to improve function in the joint. In cases where the arthroscopic technique is not advised or when it fails to achieve the desired results, a conversion to open surgery is made. This involves a larger incision and usually requires more extensive anesthesia and a longer recovery period.
The success of the rotator cuff repair is dependent on the following factors:
- age of the patient
- type of surgical technique employed
- degree of damage present
- patient's recovery goals
- patient's ability to follow a physical therapy program following surgery
- smoking status
- number of previous cortisone injections
Diagnosis/Preparation
The diagnosis of rotator cuff injury is based on a combination of clinical signs and symptoms, coupled with diagnostic testing. The most common clinical signs and symptoms include:
- tenderness in the rotator cuff
- pain associated with the movement of the arm above the head
- pain that is fairly constant but more intense at night
- weakness or pain with the forward movement of the arm
- muscle atrophy in long-term injuries that involve a complete tendon tear
X rays are used to rule out other types of injuries or abnormalities present in the shoulder region. While x rays are often used to help solidify the diagnosis, arthrography , ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) are the definitive tests in the diagnosis of rotator cuff injury. Arthography and ultrasonography of the shoulder can help determine whether or not there is a full tear in the rotator cuff. A MRI can help determine whether there is a full tear, partial tear, chronic tendonitis, or other cause of the shoulder pain. The final decision to repair the tear ultimately rests on the amount of pain and restriction suffered by the patient.
Aftercare
Following the procedure, the patient will typically spend several hours in the recovery room . Generally, an ice pack will be applied to the affected shoulder joint for a period up to 48 hours. The patient will usually be given either prescription or non-prescription pain medication. The dressing is usually removed the day after surgery and is replaced by adhesive strips. The patient should contact a physician if there are any significant changes in the affected area once the patient goes home. These changes can include increased swelling, pain, bleeding, drainage in the affected area, nausea, vomiting, or signs of infection. Signs of infection include fever, dizziness, headache, and muscle aches.
It often takes several days for the arthroscopic puncture wounds to heal, and the joint usually takes several weeks to recover. Most patients can resume normal daily activities, with the permission of a physician, within a few days following the procedure. Most patients are advised to undergo a rehabilitation program that includes physical therapy. Such a program can facilitate recovery and improve the functioning of the joint in the future.
Risks
Complications following arthroscopic rotator cuff surgery are very rare. Such complications occur in less than 1% of cases. These complications include instrument breakage, blood vessel or nerve damage, blood vessel clots, infection, and inflammation. Complications, though still rare, are more common following open surgery. This is due to the larger incisions and more complicated anesthesia that is often necessary.
Normal results
The prognosis for the long-term relief from rotator cuff syndrome is good, especially when both conservative and surgical therapeutic approaches are used. In those patients who do require surgery, six weeks of physical therapy is typically instituted following surgery. Complete recovery following surgery may take several months. In rare cases, the rotator cuff injury is so severe that the patient may require muscle transfers and tendon grafts. Even more rarely, the injury can be so severe that the tendons are not repairable. This typically occurs when a severe rotator cuff injury is neglected for a long period of time.
Morbidity and mortality rates
Morbidity is rare in both the arthroscopic and open procedures. Mortality is exceedingly rare in patients undergoing rotator cuff repair.
Alternatives
Conservative approaches are typically used before surgery is considered in patients with rotator cuff injury. This is true even in cases where there is evidence of a full tendon tear. Some patients with a full or partial tear do not suffer a significant amount of pain and retain normal or nearly normal range of motion in shoulder movement. A majority of those with rotator cuff syndrome respond to conservative non-surgical approaches. Conservative therapies include the following:
- heat or ice to reduce pain and swelling
- cessation or reduction of activities that involve the movement of the arms overhead
- medication such as non-steroidal anti-inflammatory agents to reduce pain and inflammation
- cortisone injections to reduce pain and inflammation
- rest
Once the pain begins to subside, the patient usually is encouraged to begin a program of physical therapy to help re-institute normal motion and function to the shoulder.
Resources
books
Current Medical Diagnosis & Treatment. New York: McGraw-Hill, 2003.
"Rotator Cuff Tendinitis." In The Merck Manual, edited by Keryn A. G. Lane. West Point, PA: Merck & Co., 1999.
"Rotator Cuff Syndrome." In Ferri's Clinical Advisor, edited by Fred F. Ferri. St. Louis: Mosby, 2001.
Schwartz, Seymour I., ed. Principles of Surgery. New York: McGraw-Hill 1999.
Shannon, Joyce Brennfleck. Sports Injuries Sourcebook. Detroit: Omnigraphics, Inc., 2002.
periodicals
Welling, Ken R. "Rotator Cuff Surgery." Surgical Technologist 31 (1999): 4.
Mark Mitchell
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Rotator cuff repair is generally performed by a specialist known as an orthopedic surgeon, who has received specialized training in the diseases and injuries of the musculoskeletal system. Orthopedic surgeons who perform rotator cuff repair receive extensive training in general surgery and in the specific techniques involving the musculoskeletal system. Rotator cuff repairs are often performed in the specialized department of a general hospital, but they are also performed in specialized orthopedic surgery clinics or institutes for orthopedic conditions.
QUESTIONS TO ASK THE DOCTOR
- What are my alternatives?
- Is surgery the answer for me?
- Can you recommend a surgeon who performs rotator cuff repairs?
- If surgery is appropriate for me, what are the next steps?
QUESTIONS TO ASK THE SURGEON
- How many times have you performed rotator cuff repair?
- Are you a board-certified surgeon?
- What type of outcomes have you had?
- What are the most common side effects or complications?
- What should I do to prepare for surgery?
- What should I expect following the surgery?
- Can you refer me to one of your patients who has had this procedure?
- What type of diagnostic procedures are performed to determine if patients require surgery?
- Will I need to see another specialist for the diagnostic procedures?
I'm not sure if I'm suffering from Rotator Cuff Injury, but I have been having similar symptoms to what I have been reading through this article. But I also have a stabbing, sharp pain in my forearm / palm (this is all in my right hand and arm). This is constant and is very painful and uncomfortable while using my laptop. My GP has put me on a course of 800mg paracetamol and to undergo 10 courses of physiotherapy, neither unfortunately have worked.
38yr CAD Draughtsman
I do hope you can advise.
Thank you very much,
David
I am now suffering from NERVE PAIN in my arm shoulder and wrist this keeps me awake at night nerve pain is unbearable. can you help me? emlekerman@aol.com
should mention that from the 3rd of Nov 08 untilApril23 while in therapy they were treating it as a soft tissue injury and the more I complained about the pain getting worse and movement decreasing the more they increased the therapy longer times and more exercises they kept insisting it was phantom pain all in my head but after having the operation they didn't say a word so waiting on results of MRI to see whats wrong
I am lucky to be Canadian I paid 0 $ for the visits /surgery/ MRI's/ xrays and home nurses after the surgery at which time I was also supplied with all the pain medication I could possibily require even morphine and gravol, which I still have some left over I have paid for some water proof bandages so I could shower after physio which is also covered by my government health plan.
DON"T wait if it needs repair find a good surgeon the loss of full use of your arms is far more costly!!
Because of anchors there is continuous pain, also because I am required to stretch the shoulder
area with the aid ofy right arm. Doc says I should be surfing again by November.
From these posts, surgery doesn't sound like any fun at all. How is your recovery going?
I'm interested because it looks like i need surgery. An MRI of my left shoulder revealed 'subacromial spurring; supraspinatus tendinopathy; a tear in my subscapularis and AC joint degeneration'. Brilliant!
I am a keen surfer and swimmer, but haven't surfed at all for 9 months. I know i'll be out of action for a long time to come with or without surgery but, will the surgery even enable me to surf properly again?
Thanks to everyone on this site for sharing their experiences!
Was almost healed and had a freak accident and ripped it apart again. Can I just yell you the pain with surgery.Open invasive surgery twice. I have been on pain medd since the 1st surgery on July 7th. My last surgery was Sept. 7th. I went to a pain specialist to help me with the pain because Ortho Dr. only covered my pain for 1 week. Anyway, then ask Pain Specialist to help wean me off these pain meds when the pain was tolerable. He said he applauded me. It only takes 3 weeks to become addicted. So, can't sleep, or get comfortable, and no appetite. Wondering if anyone else has a similar story to share.
Regards-Jicky
can force that shoulder to move and it will take you to your knees. Ice and meds are my friend .
Thank you
Dana Weston
cuff
Surgery third time.i am nervous.
I had major RC surgery 13 weeks ago,(3 complete tears) and physio is only now starting to get me to move my arm unaided and still barely backwards.Premature use could be what is part of your spasm (nerve) problems. Lifting anything much heavier than a cup of coffee is still painful, but apparently is quite normal at this stage.
Thank you,
Deborah
At this point, there were never any tests that were positive. So they diagnosed me as having Rotator cuff Syndrome. When I saw the surgeon Pre-Op, she concluded that this would most likely be a cleanup, go in get out surgery. Most likely 2, maybe 3 weeks max in a sling. I was all settled with that, for once, a very pessimistic me, overcame and told myself it'd be nothing so don't fuss to worry about what-if. Knowing that 3 ortho Drs and radiologist techs never saw "anything wrong", I was convinced easier. Last week, June 21, 2018, I went in for a diagnostic Arthroscopy. When I woke up, I found out that the surgeon "was shocked" to find a "very large tear". She ended up having to perform rotator cuff repair and bicep Tenodesis. That was way more than I even thought of. I thought rotator cuff those 2 years. I had never in my life even heard of the words tenotomy or tenodesis. Well, I am glad they found and repaired what was needed but I am very discouraged... and actually scared now. I see my surgeons assistant for my initial Post-op appt in 3 days. Then, I hope to find out what this entails. I now, most definitely know this won't be only a 2-3 week process, as previously thought. Here goes.