Finger reattachment
Definition
Finger reattachment (or replacement) is defined as reattachment of the part that has been completely amputated.
Purpose
Replantation refers to reattachment of a completely severed part, meaning there is no physical connection between the part that has been cut off and the person. Reattachment can be surgically performed for the finger and such other detached body parts, as the hand or arm.
Demographics
Good candidates for this procedure include persons with thumb or multiple digit amputation . Injury to multiple digits is an important patient selection criterion, since in some cases the least damaged digits may be shifted to the least injured or most useful stump. Patient exclusion is neither clear-cut nor absolute. Generally, severe crushing or avulsing (tearing away) injuries to the fingers may make replantation difficult, but venous grafts may help replace injured blood vessels. Additionally, older persons may have arteriosclerosis that frequently impairs function in blood vessels, especially in small vessels. Special efforts may be made to replant fingers if the person's livelihood (such as professional musical performance) depends on absolute finger control.
Description
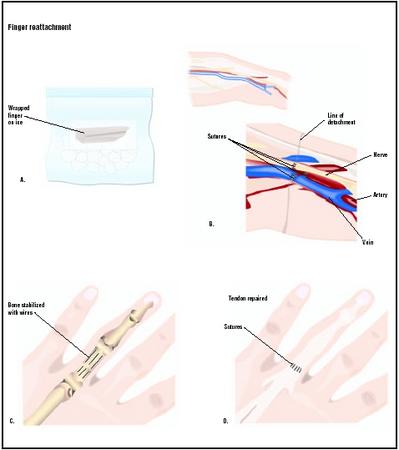
To increase efficiency, the replantation team splits into two sub-teams. One sub-team in the operating room cleans the amputated finger with sterile solutions, places it on ice, and identifies and tags (with special surgical clips) nerves and blood vessels. Dead or damaged tissue is surgically removed with a procedure called debridement . The emergency room (ER) sub-team will assess the patient during a physical exam with x rays of the injured area, blood analysis, and cardiac (heart) monitoring. The patient is given fluids intravenously (IV), a tetanus injection, and antibiotics . Usually, most finger reattachments are performed with a local anesthetic such as bupivacaine and a nerve block to numb the affected arm. Maintaining a warm body temperature can enhance blood flow to the affected limb.
The surgical procedure consists of several stages. The bone in the amputated finger must be shortened and fixed, which means that the bone end is trimmed. After this process, the bone is stabilized with special sutures called K-wires, and fixed pins are placed in the bone after drilling a space to insert them. This process connects the two amputated bone fragments. After bone stabilization and fixation, the extensor and flexor tendons are repaired. This step is vital, since arteries, veins, and nerves should never be surgically connected under tension. Next, the surgeon must repair (suture) cut-off tendons, arteries, veins, and nerves. Healthy arteries and veins are sutured together without tension. A vein graft is used for blood vessels that cannot be reattached.
Nerve repair for finger reattachment is not difficult. Since the reattached bone parts are shorter than the original length, nerves can be reattached without tension. A microscope is used for magnified visualization of finger nerves during reattachment. When the severed ends of the nerve cannot be reattached, a primary nerve graft is performed. Finally, it is vital superficial veins on the affected finger (dorsal veins) to cover with a skin flap to prevent death of the venous vessels. The skin over the surgical field is loosely sutured with a few sutures. Any damaged tissue that may die (necrotic tissue) is removed. No tension should be placed on the skin fields during closure of the wound. Wounds are covered with small strips of gauze impregnated with petrolatum. The upper extremity is immobilized, and compression hand dressing and plaster splints are arranged to prevent slipping and movement of the affected arm.
Diagnosis/Preparation
The diagnosis is easily made by visual inspection since the finger(s) must be completely detached from the hand. The reattachment procedure is complex and involves the expertise and skill of a highly trained surgeon. There are several important factors necessary to successful replantation, including special instrumentation and transportation of the amputated finger. Surgical loupes (binocular-type eyepieces used by surgeons to magnify small structures during surgery) are necessary for this procedure. Instruments should be at least 3.9 in (10 cm) long to allow for proper positioning in the surgeon's hands. Special clips are used to help suture blood vessels together. The best method of saving and transporting the amputated finger is to wrap it with moistened cloth (Ringer's lactate solution or saline solution) and place it on ice. Generally, the tissues will survive for about six hours without cooling. If the part is cooled, tissue survival time is approximately 12 hours. Fingers have the best outcome for transportation survival, since digits (fingers) do not have a large percentage of muscle tissue.
Aftercare
Postoperative care is vital for successful finger reattachment. The hand is wrapped in a bulky compression dressing and usually elevated. If arterial flow is impaired, then the hand should be lowered, since this maneuver will promote blood flow from the heart to the reattached finger. If venous outflow is slow, the hand must be elevated. Medications to increase blood flow (peripheral vasodilators) and an anticoagulant (heparin) are used. A tranquilizer may be given to reduce unnecessary blood vessel movement (vasospasm) that can occur due to anxiety. Careful examination of the reattached digit(s) is necessary. The surgeon frequently monitors color, the capacity of blood vessels, capillary refill, and warmth to monitor replant progress. The YSI telethermometer monitors the digital (finger) temperature with small surface probes. Skin temperature falling below 86°F (30°C) indicates poor blood perfusion
(poor blood and oxygen delivery to the affected area) of the replant. The cause of poor blood circulation must be investigated and corrected, if possible. The patient's room should be warm, and bed rest for two to three days is recommended. Patients must refrain from smoking and take antibiotics for one week after surgery. Follow-up consultations are necessary for continued wound care and rehabilitation.
Risks
The experienced surgeon can estimate the likelihood complications based on the nature of the injury. Replantations that are risky, such as those with circulatory perfusion problems, have lower success rates. Generally, the most difficult replantations are those that involve children under 10, injuries caused by a ring catching in machinery, and crush-and-tear injuries. Management of the difficult replant typically includes intravenous heparin to prevent clotting of the blood, and providing a continuous nerve block in either the median or ulnar nerve (depending on which fingers are reattached). A nerve block will cause vasodilatation, or expansion of the blood vessel. Vasodilatation will increase blood flow, bringing with it fresh oxygenated blood. Further evaluation should include checking the patient's dressing for constriction (i.e., if the dressing was placed too snugly and is constricting local blood vessels).
Normal results
Normal results may not seem encouraging. It must be considered that this is a major trauma and a highly complicated and intricate surgical repair. Generally, a normal result usually includes good nerve recovery; approximately 50% of normal for active range of joint motion; cold intolerance (usually reversed in about two years); and acceptable cosmetic results.
Morbidity and mortality rates
There are about 10,000 cases of job-related amputations in the United States each year; 94% of these involve fingers. Few statistics are available for the out-come of replantations.
Alternatives
The only alternative to this procedure is to lose the finger(s) entirely and manage the remaining hand injury.
Resources
books
American Society for Surgery of the Hand. The Hand: Primary Care of Common Problems. New York: Churchill Livingstone, 1990.
Green, David P. Operative Hand Surgery, Volume 1, 3rd Edition. New York: Churchill Livingstone, Inc., 1993.
Green, David P. Operative Hand Surgery, Volume 2, 3rd Edition. New York: Churchill Livingstone, Inc., 1993.
organizations
American Association for Hand Surgery. 20 North Michigan Avenue, Suite 700, Chicago, Il 60602. (321) 236-3307; Fax: (312) 782-0553. E-mail: contact@handssurgery.org. http://www.handsurgery.org .
other
"Superficial Fingertip Avulsion." National Center for Emergency Medicine Informatics. [cited June 2003] http://www.ncemi.org/cse/cse1002.htm .
"The V-Y Plasty in the Treatment of Fingertip Amputations." American Academy of Family Physicians. [cited June 2003] http://www.aafp.org/afp/20010801/455.html .
Laith Farid Gulli, MD, MS
Bilal Nasser, MD, MS
Robert Ramirez, BS
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
The procedure is usually performed in a hospital operating room by a microsurgeon, who may be a plastic surgeon with five years of general surgery training, plus two years of plastic surgery training and another one or two years of training in microneurovascular surgery; or an orthopedic surgeon with one year of general surgery training, five years of orthopedic surgery training, and additional years in micro-surgery training.
QUESTIONS TO ASK THE DOCTOR
- Are there any special precautions I should take with my pain medication?
- How should I care for the wound?
- When will I regain feeling and function in the affected finger(s)?
- Will I need physical therapy for the injury?
- How much function can I expect to regain?
Ben
I was wondering about my grandson.(11 Months old.) He had to have two of his little fingers attached agan after an accident at home. since then the drs. says that he will have to have his little fingers buried inside the palm of his hand in order for his nails to grow back . is this a succeesful surgury. have this kind of surgury been done before? I would like to know more about this. thank so much. his mom and Dad are very concerned about this. the surgury is supposed to take place in REd Deer AB.how is this all done?
A CHILD WITH ARTIFICIAL FINGERS OR TRANSPLANTING TISSUE ETC ETC
You really should contact him and let him know how he impacted your life..we certainly have!
For My project I need the following Clarification
Can we transplant Finger vein from one person to another person?
And also i need know the unique feature about the Veins.
Is there my fingers can reattach or replant?
My right hand 2nd finger have cut,plz advise how will attached my finger in BD.
Thanks/Hasan
Thanks & Regards
My top portion of fore finger (less then a third of it) got amputed doctors
said that reattachement is not possible.
What are the ways to get complete finger by attaching artificial part to it ,so that it is permenent?
Thanks
Sasha
My ring finger of the left hand was cut-off from the nail area upwards in a bus accident. I am wondering if it is possible to get a replant of the same and where. If not is it possible to get a plastic extension of the same to enable me resume playing the keyboard and guitar?
Please let me know.
Thank you and regards,
Cathy.
My father had met with an accident 2 months back and lost his left hands fingers which were badly crushed by bus. Now he is recovering his hand after the skin grafting.
kindly let me know any options of reattachment of artificial fingers possible in india.
i got injured in my small finger yesterday doctor has done a plastic surgery and told me that they have to stitch my vein for my small finger my question is will they remove the stitch from my vein or not coz they said that it will be there for life time, is there any kind of side effect or the stitch will be dissolved as it heels please tell me what should i do
my left hand middle finger top nail point is cutted in cutter machine ..before 15 year now m 20 years old. so can i get my full finger...n how can i get it..plz tell me.. thanks
SEEN BY PLASTIC SURGEON HE WAS'T ENCOURIG WITH PHYGIO AND ECERCISE THUMB BONE INCRESEDIN LENGTH AND HALF NAIL STILL MUCLES IS AWAY FROM THUMB.THERE IS ANY MICRO SURGERY THAT MAKE VEDGE LIKE V TO BRING THE MUSCELS CLOSE TO NAIL TO NAIL WHICH LETHE NAIL INCREASE IN SIZE TO MAKE NORMAL AND FUNCTIONAL. I AM HER SISTER PODIATRIST PLEASE DOCTOR HELP US'
Thank you
HELEN PETER
If possible suggest me an option
my left hand middle finger top nail point is cutted in cutter machine ..before 15 year now m 21 years old. so can i get my full finger...n how can i get it..plz tell me.. thanks
My little daughter has cut and removed her Interphalangeal from her left hand and it doesn't looking good. at yet she is 6year of age kindly suggest me what is the solution for her can i transplant and is there any other solution.
I play guitar, and I'd like to think I play guitar really well. I am near f***ing petrified that I'll never be able to play again. I have no question or anything, I just need to get out my feelings. The pain was nothing, I don't care what it looks like, and if I never feel with the top of my finger again, I don't care. The only that scares me, that truly, truly scares me, to f***ing tears is that I'll never be able to play guitar again, that I won't be able to do what I love to do. I played just about every day, and I took that for granted. I haven't played guitar in 4 days now and I'm crying my eyes out because I'm so scared I'll never play again. I don't even know if the top of my finger will stay at this point. I just want to play guitar again. All I want is to play guitar again.
My son is 2 month old. He was born without finger on the left leg. We did scan and found all five fingers and toe have only one-one bone. The baby is normal and hands and right leg are good. Only left leg fingers could not be grown. The Foot soles of left leg is in good condition. Could you please advise me what to do.
Is there any possibility for transplant or reconstructive surgery is enough.
This Muhammad Riaz from Kabul Afghanistan,
Actually My Cousin Hijrat Shinwari lost Right hand thumb a few days ago would please give information about thumb finger re attachments plastic surgery or donate from other ways.
Waiting for your kind reply
Faithfully Muhammad Riaz