Coronary artery bypass graft surgery
Definition
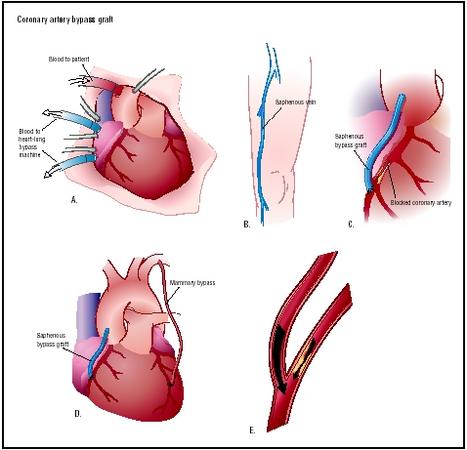
Coronary artery bypass graft surgery is a surgical procedure in which one or more blocked coronary arteries are bypassed by a blood vessel graft to restore normal blood flow to the heart. These grafts usually come from the patient's own arteries and veins located in the leg, arm, or chest.
Purpose
Coronary artery bypass graft surgery (also called coronary artery bypass surgery [CABG] and bypass operation) is performed to restore blood flow to the heart. This relieves chest pain and ischemia, improves the patient's quality of life, and, in some cases, prolongs the patient's life. The goals of the procedure are to relieve symptoms of coronary artery disease, enable the patient to resume a normal lifestyle, and to lower the risk of a heart attack or other heart problems.
According to the American Heart Association, appropriate candidates for coronary artery bypass graft surgery include patients who:
- have blockages in at least two to three major coronary arteries, especially if the blockages are in arteries that feed the heart's left ventricle or in the left anterior descending artery
- have angina so severe that even mild exertion causes chest pain
- have poor left ventricular function
- cannot tolerate percutaneous transluminal coronary angioplasty and do not respond well to drug therapy
Demographics
Coronary artery bypass graft surgery is widely performed in the United States. It is estimated that more than 800,000 coronary artery bypass graft surgeries are performed worldwide every year. The American Heart Association reports that 519,000 coronary artery bypass graft surgeries were performed in the United States in 2000, of which 371,000 were performed on men and 148,000 on women.
Description
Coronary artery bypass graft surgery builds a detour around one or more blocked coronary arteries with a graft from a healthy vein or artery. The graft goes around the clogged artery (or arteries) to create new pathways for oxygen-rich blood to flow to the heart.
Procedure
After general anesthesia is administered, the surgeon removes the veins or prepares the arteries for grafting. If the saphenous vein is to be used for the graft, a series of incisions are made in the patient's thigh or calf. If the radial artery is to be used for the graft, incisions are made in the patient's forearm. It is important to note that the removal of veins or arteries for grafting does not deprive the area of adequate blood flow.
More commonly, a segment of the internal mammary artery is used for the graft, and the incisions are made in the chest wall. The internal mammary arteries are most commonly used because they have shown the best long-term results. Because they have their own oxygen-rich blood supply, the internal mammary arteries can usually be kept intact at their origin, then sewn to the coronary artery below the site of blockage.
The surgeon decides which grafts to use, depending on the location of the blockage, the amount of the blockage, and the size of the patient's coronary arteries.
In traditional coronary artery bypass surgery, the surgeon makes an incision down the center of the patient's chest, cuts through the breastbone, and retracts the rib cage open to expose the heart. The patient is connected to a heart-lung bypass machine, also called a cardiopulmonary bypass pump, that takes over for the heart and lungs during the surgery. During this "on-pump" procedure, the heart-lung machine removes carbon dioxide from the blood and replaces it with oxygen. A tube is inserted into the aorta to carry the oxygenated blood from the bypass machine to the aorta for circulation to the body. The heart-lung machine allows the heart's beating to be stopped, so the surgeon can operate on a still heart. Aortic clamps are used to restrict blood flow to the area of the heart where grafts will be placed so the heart is blood-free during the surgery. The clamps remain until the grafts are in place.
Some patients may be candidates for minimally invasive coronary artery bypass surgery or for off-pump bypass surgery. During minimally invasive surgery, smaller chest and graft removal incisions are used, promoting a quicker recovery and less risk of infection. Off-pump bypass surgery, also called beating heart surgery, is a surgical technique performed while the heart is still beating. The surgeon uses advanced equipment to stabilize portions of the heart and bypass the blocked artery while the rest of the heart keeps pumping and circulating blood through the body.
After the grafts are prepared, a small opening is made just below the blockage in the diseased coronary artery. Blood will be redirected through this opening once the graft is sewn in place. If a leg or arm vein is used, one end is connected to the coronary artery and the other to the aorta; if a mammary artery is used, one end is connected to the coronary artery while the other remains attached to the aorta. The procedure is repeated on as many coronary arteries as necessary. On average, three or four coronary arteries are bypassed during surgery. Blood flow is checked to assure the graft supplies adequate blood to the heart.
If the procedure was done "on-pump," electric shocks start the heart pumping again after the grafts have been completed. The heart-lung machine is turned off and the blood slowly returns to normal body temperature. After implanting pacing wires and inserting a chest tube to drain fluid, the surgeon closes the chest cavity. Sometimes a temporary pacemaker is attached to the pacing wires to regulate the heart rhythm until the patient's condition improves. After surgery, the patient is transferred to an intensive care unit for close monitoring.
Diagnosis/Preparation
Diagnosis
The diagnosis of coronary artery disease is made after the patient's medical history is carefully reviewed, a physical exam is performed, and the patient's symptoms are evaluated. Tests used to diagnose coronary artery disease include:
- electrocardiogram
- stress tests
- cardiac catheterization
- imaging tests such as a chest x ray , echocardiography , or computed tomography (CT)
- blood tests to measure blood cholesterol, triglycerides, and other substances
Preparation
The individual should quit smoking or using tobacco products before the surgery. The individual needs to make the commitment to be a nonsmoker after the surgery. There are several smoking cessation programs available in the community. The individual can ask a health care provider for more information about quitting smoking.
Coronary artery bypass graft surgery should ideally be postponed for three months after a heart attack. Patients should be medically stable before the surgery, if possible.
During a preoperative appointment, usually scheduled within one to two weeks before surgery, the patient will receive information about what to expect during the surgery and the recovery period. The patient will usually meet the cardiologist, anesthesiologist, nurse clinicians, and surgeon during this appointment or just before the procedure.
If the patient develops a cold, fever, or sore throat within a few days before the surgery, he or she should notify the surgeon's office.
The evening before the surgery, the patient showers with antiseptic soap provided by the surgeon's office. After midnight, the patient should not eat or drink anything.
The patient is usually admitted to the hospital the same day the surgery is scheduled. The patient should bring a list of current medications, allergies, and appropriate medical records upon admission to the hospital .
Before the surgery, the patient is given a blood-thinning drug—usually heparin—that helps to prevent blood clots. A sedative is given the morning of surgery. The chest and the area from where the graft will be taken are shaved.
Coronary angiography will have been previously performed to show the surgeon where the arteries are blocked and where the grafts might best be positioned. Heart monitoring is initiated. The patient is given general anesthesia before the procedure.
The length of the procedure depends upon the number of arteries being bypassed, but it generally takes from three to five hours—sometimes longer.
Aftercare
Recovery in the hospital
The patient recovers in a surgical intensive care unit for one to two days after the surgery. The patient will be connected to chest and breathing tubes, a mechanical ventilator, a heart monitor, and other monitoring equipment. A urinary catheter will be in place to drain urine. The breathing tube and ventilator are usually removed about six hours after surgery, but the other tubes usually remain in place as long as the patient is in the intensive care unit.
Drugs are prescribed to control pain and to prevent unwanted blood clotting. Daily doses of aspirin are started within six to 24 hours after the procedure.
The patient is closely monitored during the recovery period. Vital signs and other parameters such as heart sounds, oxygen, and carbon dioxide levels in arterial blood are checked frequently. The chest tube is checked to ensure that it is draining properly. The patient may be fed intravenously for the first day or two.
Chest physiotherapy is started after the ventilator and breathing tubes are removed. The therapy includes coughing, turning frequently, and taking deep breaths. Sometimes oxygen is delivered via a mask to help loosen and clear secretions from the lungs. Other exercises will be encouraged to improve the patient's circulation and prevent complications due to prolonged bed rest.
If there are no complications, the patient begins to resume a normal routine on the second day, including eating regular food, sitting up, and walking around a bit. Before being discharged from the hospital, the patient usually spends a few days under observation in a nonsurgical unit. During this time, counseling is usually provided on eating right and starting a light exercise program to keep the heart healthy.
The average hospital stay after coronary artery bypass graft surgery is five to seven days.
Recovery at home
INCISION AND SKIN CARE. The incision should be kept clean and dry. When the skin is healed, the incision should be washed with soapy water. The scar should not be bumped, scratched, or otherwise disturbed. Ointments, lotions, and dressings should not be applied to the incision unless specific instructions have been given.
DISCOMFORT. While the incision scar heals, which takes one to two months, it may be sore. Itching, tightness, or numbness along the incision are common. Muscle or incision discomfort may occur in the chest during activity.
Swelling or aching may occur in the legs if the saphenous vein was used for the graft. Special support stockings may be needed to decrease leg swelling after surgery. While sitting, the patient should not cross the legs and the feet should be elevated. Walking daily, even if the legs are swollen, will help improve circulation and reduce swelling.
LIFESTYLE CHANGES. The patient needs to make several lifestyle changes after surgery, including:
- Quitting smoking. Smoking causes damage to the bypass grafts and other blood vessels, increases the patient's blood pressure and heart rate, and decreases the amount of oxygen available in the blood.
- Managing weight. Maintaining a healthy weight, by watching portion sizes and exercising, is important. Being overweight increases the work of the heart.
- Participating in an exercise program. The exercise program is usually tailored for the patient, who will be encouraged to participate in a cardiac rehabilitation program supervised by exercise professionals.
- Making dietary changes. Patients should eat a lot of fruits, vegetables, grains, and non-fat or low-fat dairy products, and reduce fats to less than 30% of all calories.
- Taking medications as prescribed. Aspirin and other heart medications may be prescribed, and the patient may need to take these medications for life.
- Following up with health care providers. The patient must schedule follow-up visits to determine how effective the surgery was, to confirm that progressive exercise is safe, and to monitor his or her recovery and control risk factors.
Risks
Coronary artery bypass graft surgery is major surgery and patients may experience any of the normal complications associated with major surgery and anesthesia, such as the risk of bleeding, pneumonia, or infection. Possible complications include:
- graft closure or blockage
- development of blockages in other arteries
- damage to the aorta
- long-term development of atherosclerotic disease of saphenous vein grafts
- abnormal heart rhythms
- high or low blood pressure
- recurrence of angina
- blood clots that can lead to a stroke or heart attack
- kidney failure
- depression or severe mood swings
- possible short-term memory loss, difficulty thinking clearly, and problems concentrating for long periods (These effects generally subside within six months after surgery.)
There is a higher risk for complications in patients who:
- are heavy smokers
- have a history of lung, kidney, or metabolic diseases
- have diabetes
- have had a recent heart attack
- have a history of angina, ventricular arrhythmias, congestive heart failure, cerebrovascular disease, or mitral regurgitation
Normal results
Full recovery from coronary artery bypass graft surgery takes two to three months and is a gradual process. Upon release from the hospital, the patient will feel weak because of the extended bed rest in the hospital. Within a few weeks, the patient should begin to feel stronger.
Most patients are able to drive in about three to eight weeks, after receiving approval from their physician. Sexual activity can generally be resumed in three to four weeks, depending on the patient's rate of recovery.
It takes about six to eight weeks for the sternum to heal. During this time, the patient should not perform activities that cause pressure or weight on the breastbone or tension on the arms and chest. Pushing and pulling heavy objects (as in mowing the lawn) should be avoided and lifting objects more than 20 lbs (9 kg) is not permitted. The patient should not hold his or her arms above shoulder level for a long period of time, such as when doing household chores. The patient should try not to stand in one place for longer than 15 minutes. Stair climbing is permitted unless other instructions have been given.
Within four to six weeks, people with sedentary office jobs can return to work; people with physical jobs such as construction work or jobs requiring heavy lifting must wait longer (up to 12 weeks) or may have to change careers.
About 90% of patients experience significant improvements after coronary artery bypass graft surgery. Patients experience full relief from chest pain and resume their normal activities in about 70% of the cases; the remaining 20% experience partial relief.
For most people, the graft remains open for about 10–15 years.
Coronary artery bypass surgery does not prevent coronary artery disease from recurring. Therefore, lifestyle changes are strongly recommended and medications are prescribed to reduce this risk. About 40% of patients have a new blockage within 10 years after surgery and require a second bypass, change in medication, or an interventional procedure.
Morbidity and mortality rates
The risk of death during coronary artery bypass graft surgery is 2–3%.
In 5–10% of coronary artery bypass graft surgeries, the bypass graft stops supplying blood to the bypassed artery within one year. Younger people who are healthy except for the heart disease achieve good results with bypass surgery. Patients who have poorer results from coronary artery bypass graft surgery include those over the age of 70, those who have poor left ventricular function, are undergoing a repeat surgery or other procedures concurrently, and those who continue smoking, do not treat high cholesterol or other coronary risk factors, or have another debilitating disease.
Over the long term, symptoms recur in only about 3–4% of patients per year. Five years after coronary artery bypass graft surgery, survival expectancy is 90%, at 10 years it is about 85%, at 15 years it is about 55%, and at 20 years it is about 40%.
Angina recurs in about 40% of patients after 10 years. In most cases, it is less severe than before the surgery and can be controlled with drug therapy. In patients who have had vein grafts, 40% of the grafts are severely obstructed 10 years after the procedure. Repeat coronary artery bypass graft surgery may be necessary, and is usually less successful than the first surgery.
Alternatives
All patients with coronary artery disease can help improve their condition by making lifestyle changes such as quitting smoking, losing weight if they are overweight, eating healthy foods, reducing blood cholesterol, exercising regularly, and controlling diabetes and high blood pressure.
All patients with coronary artery disease should be prescribed medications to treat their condition. Antiplatelet medications such as aspirin or clopidogrel (Plavix) are usually recommended. Other medications used to treat angina may include beta blockers, nitrates, and angiotensin-converting enzyme (ACE) inhibitors. Medications may also be prescribed to lower lipoprotein levels, since elevated lipoprotein levels have been associated with an increased risk of cardiovascular problems.
Treatment with vitamin E is not recommended because it does not lower the rate of cardiovascular events in people with coronary artery disease. Although antioxidants such as vitamin C, beta-carotene, and probucol show promising results, they are not recommended for routine use. Treatment with folic acid and vitamins B 6 and B 12 lowers homocysteine levels (reducing the risk for cardiovascular problems), but more studies are needed to determine if lowered homocysteine levels correlate with a reduced rate of cardiovascular problems in treated patients.
Less invasive, nonsurgical interventional procedures—such as balloon angioplasty, stent placement, rotoblation, atherectomy, or brachytherapy—can be performed to open a blocked artery. These procedures may be the appropriate treatment for some patients before coronary artery bypass graft surgery is considered.
Enhanced external counterpulsation (EECP) may be a treatment option for patients who are not candidates for interventional procedures or coronary artery bypass graft surgery. During EECP, a set of cuffs is wrapped around the patient's calves, thighs, and buttocks. These cuffs gently but firmly compress the blood vessels in the lower limbs to increase blood flow to the heart. The inflation and deflation of the cuffs are electronically synchronized with the heartbeat and blood pressure using electrocardiography and blood pressure monitors. EECP may encourage blood vessels to open small channels to eventually bypass blocked vessels and improve blood flow to the heart. Not all patients are candidates for this procedure, and treatments, lasting one to two hours, must be repeated about five times a week for up to seven weeks.
Resources
books
American Heart Association. "Considering Surgery or Other Interventions." In Guide to Heart Attack Treatment, Recovery, Prevention. New York: Time Books, 1996.
Barry, Frank. The Healthy Heart Formula: The Powerful, New, Commonsense Approach to Preventing and Reversing Heart Disease. New York: John Wiley & Sons, 1998.
DeBakey, Michael E., and Antonio M. Gotto Jr. "Surgical Treatment of Coronary Artery Disease." In The New Living Heart. Holbrook, MA: Adams Media Corporation, 1997.
McGoon, Michael D., and Bernard J. Gersh. Mayo Clinic Heart Book: The Ultimate Guide to Heart Health, Second Edition. New York: William Morrow and Co., Inc., 2000.
Texas Heart Institute. "Heart Surgery." In Texas Heart Institute Heart Owner's Handbook. New York: John Wiley & Sons, 1995.
Topol, Eric J. Cleveland Clinic Heart Book: The Definitive Guide for the Entire Family from the Nation's Leading Heart Center. New York: Hyperion, 2000.
Trout, Darrell, and Ellen Welch. Surviving with Heart: Taking Charge of Your Heart Care. Golden, CO: Fulcrum Publishing, 2002.
periodicals
Eagle, K. A., et al. "ACC/AHA Guidelines for Coronary Artery Bypass Graft Surgery: Executive Summary and Recommendations: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1991 Guidelines for Coronary Artery Bypass Graft Surgery)." Circulation 100 (1999): 1464–1480.
Mullany, Charles J. "Coronary Artery Bypass Surgery." Circulation 107 (2003): e21–e22.
Sabik, Joseph. Off-Pump Bypass Surgery: Improving Outcomes for Coronary Artery Bypass Surgery. Cleveland Clinic Heart Center, The Cleveland Clinic Foundation. November 2001.
organizations
American College of Cardiology. Heart House. 9111 Old Georgetown Rd., Bethesda, MD 20814-1699. (800) 253-4636, ext. 694, or (301) 897-5400. http://www.acc.org .
American Heart Association. 7272 Greenville Ave., Dallas, TX 75231. (800) 242-8721 or (214) 373-6300. http://www.americanheart.org .
The Cleveland Clinic Heart Center, The Cleveland Clinic Foundation. 9500 Euclid Avenue, F25, Cleveland, Ohio, 44195. (800) 223-2273, ext. 46697, or (216) 444-6697. http://www.clevelandclinic.org/heartcenter .
National Heart, Lung, and Blood Institute. National Institutes of Health. Building 1. 1 Center Dr., Bethesda, MD 20892. E-mail: NHLBIinfo@rover.nhlbi. http://www.nhlbi.nih.gov .
Texas Heart Institute. Heart Information Service. P.O. Box 20345, Houston, TX 77225-0345. http://www.tmc.edu/thi .
other
The Heart: An Online Exploration. The Franklin Institute Science Museum. 222 North 20th Street, Philadelphia, PA, 19103. (215) 448-1200. http://sln2.fi.edu/biosci/heart.html .
HeartCenterOnline. http://www.heartcenteronline.com .
Heart Information Network. http://www.heartinfo.org . HeartSurgeon.com . http://www.heartsurgeon.com .
Lori De Milto Angela M. Costello
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
The surgery team for coronary artery bypass graft surgery includes the cardiovascular surgeon, assisting surgeons, a cardiovascular anesthesiologist, a perfusion technologist (who operates the heart-lung machine), and specially trained nurses. The surgery is performed in a hospital.
QUESTIONS TO ASK THE DOCTOR
- Why is this surgery being performed?
- Am I a candidate for minimally invasive coronary artery bypass surgery?
- Which technique will be used during the surgery, the "on-pump" or "off-pump" technique?
- Who will be performing the surgery? How many years of experience does this surgeon have? How many other coronary artery bypass graft surgeries has this surgeon performed?
- Should I take my medications the day of the surgery?
- How long will I have to stay in the hospital after the surgery?
- After I go home from the hospital, how long will it take me to recover from surgery?
- What should I do if I experience chest discomfort or other symptoms similar to those I felt before surgery?
- What types of symptoms should I report to my doctor?
- How should I care for my incision?
- What types of medications will I have to take after surgery?
- When will I be able to resume my normal activities?
- If I have had the surgery once, can I have it again to correct future blockages?
- Are there any medications, foods, or activities I should avoid to prevent my symptoms from recurring?
- What lifestyle changes (including diet, weight management , exercise, and activity changes) are recommended after the procedure to improve my heart health?
- How often do I need to see my doctor for follow-up visits after the surgery?
ROSARIO
My father had heart bypass surgery last December. He's already in his 8th week of recovery. Last week he carried a heavy load, (more than what is allowed I think) and his wound start to feel painful again...no difficulty in breathing though.Are there any complications that we should be concerned about?Thanks...
i am 90 next april
left leg full of water
wat to do
waterpill does not work verry well
also one heartvalve leaking
514 738 5904
and daily intake is a problem any other alternate or procedure to get rid of life long medication?
plse give me answer this would help millions of people like me any consequence if other cardiologist prescribe alternate indigenous available drug of lessor low in place of costlier one of other country