Thyroidectomy
Definition
Thyroidectomy is a surgical procedure in which all or part of the thyroid gland is removed. The thyroid gland is located in the forward (anterior) part of the neck just under the skin and in front of the Adam's apple. The thyroid is one of the body's endocrine glands, which means that it secretes its products inside the body, into the blood or lymph. The thyroid produces several hormones that have two primary functions: they increase the synthesis of proteins in most of the body's tissues, and they raise the level of the body's oxygen consumption.
Purpose
All or part of the thyroid gland may be removed to correct a variety of abnormalities. If a person has a goiter, which is an enlargement of the thyroid gland that causes swelling in the front of the neck, the swollen gland may cause difficulties with swallowing or breathing. Hyperthyroidism (overactivity of the thyroid gland) produces hypermetabolism, a condition in which the body uses abnormal amounts of oxygen, nutrients, and other materials. A thyroidectomy may be performed if the hypermetabolism cannot be adequately controlled by medication, or if the condition occurs in a child or pregnant woman. Both cancerous and noncancerous tumors (frequently called nodules) may develop in the thyroid gland. These growths must be removed, in addition to some or all of the gland itself.
Demographics
Screening tests indicate that about 6% of the United States population has some disturbance of thyroid function, but many people with mildly abnormal levels of thyroid hormone do not have any disease symptoms. It is estimated that between 12 and 15 million people in the United States and Canada are receiving treatment for thyroid disorders as of 2002. In 2001, there were approximately 34,500 thyroidectomies performed in the United States. Females are somewhat more likely than males to require a thyroidectomy.
Description
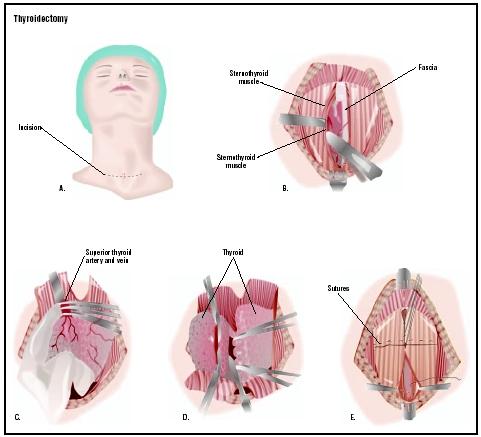
A thyroidectomy begins with general anesthesia administered by an anesthesiologist. The anesthesiologist injects drugs into the patient's veins and then places an airway tube in the windpipe to ventilate (provide air for) the person during the operation. After the patient has been anesthetized, the surgeon makes an incision in the front of the neck at the level where a tight-fitting necklace would rest. The surgeon locates and takes care not to injure the parathyroid glands and the recurrent laryngeal nerves, while freeing the thyroid gland from these surrounding structures. The next step is clamping off the blood supply to the portion of the thyroid gland that is to be removed. Next, the surgeon removes all or part of the gland. If cancer has been diagnosed, all or most of the gland is removed. If other diseases or nodules are present, the surgeon may remove only part of the gland. The total amount of glandular tissue removed depends on the condition being treated. The surgeon may place a drain, which is a soft plastic tube that allows tissue fluids to flow out of an area, before closing the incision. The incision is closed with either sutures (stitches) or metal clips. A dressing is placed over the incision and the drain, if one has been placed.
People generally stay in the hospital one to four days after a thyroidectomy.
Diagnosis/Preparation
Thyroid disorders do not always develop rapidly; in some cases, the patient's symptoms may be subtle or difficult to distinguish from the symptoms of other disorders. Patients suffering from hypothyroidism are sometimes misdiagnosed as having a psychiatric depression. Before a thyroidectomy is performed, a variety of tests and studies are usually required to determine the nature of the thyroid disease. Laboratory analysis of blood determines the levels of active thyroid hormones circulating in the body. The most common test is a blood test that measures the level of thyroid-stimulating hormone (TSH) in the bloodstream. Sonograms and computed tomography scans ( CT scans ) help to determine the size of the thyroid gland and location of abnormalities. A nuclear medicine scan may be used to assess thyroid function or to evaluate the condition of a thyroid nodule, but it is not considered a routine test. A needle biopsy of an abnormality or aspiration (removal by suction) of fluid from the thyroid gland may also be performed to help determine the diagnosis.
If the diagnosis is hyperthyroidism, a person may be asked to take antithyroid medication or iodides before the operation. Continued treatment with antithyroid drugs may be the treatment of choice. Otherwise, no other special procedure must be followed prior to the operation.
Aftercare
A thyroidectomy incision requires little to no care after the dressing is removed. The area may be bathed gently with a mild soap. The sutures or the metal clips are removed three to seven days after the operation.
Risks
There are definite risks associated with the procedure. The thyroid gland should be removed only if there is a pressing reason or medical condition that requires it.
As with all operations, people who are obese, smoke, or have poor nutrition are at greater risk for developing complications related to the general anesthetic itself.
Hoarseness or voice loss may develop if the recurrent laryngeal nerve is injured or destroyed during the operation. Nerve damage is more apt to occur in people who have large goiters or cancerous tumors.
Hypoparathyroidism (underfunctioning of the parathyroid glands) can occur if the parathyroid glands are injured or removed at the time of the thyroidectomy. Hypoparathyroidism is characterized by a drop in blood calcium levels resulting in muscle cramps and twitching.
Hypothyroidism (underfunctioning of the thyroid gland) can occur if all or nearly all of the thyroid gland is removed. Complete removal, however, may be intentional when the patient is diagnosed with cancer. If a person's thyroid levels remain low, thyroid replacement medications may be required for the rest of his or her life.
A hematoma is a collection of blood in an organ or tissue, caused by a break in the wall of a blood vessel. The neck and the area surrounding the thyroid gland have a rich supply of blood vessels. Bleeding in the area of the operation may occur and be difficult to control or stop. If a hematoma occurs in this part of the body, it may be life-threatening. As the hematoma enlarges, it may obstruct the airway and cause a person to stop breathing. If a hematoma does develop in the neck, the surgeon may need to perform drainage to clear the airway.
Wound infections can occur. If they do, the incision is drained, and there are usually no serious consequences.
Normal results
Most patients are discharged from the hospital one to four days after a thyroidectomy. Most resume their normal activities two weeks after the operation. People who have cancer may require subsequent treatment by an oncologist or endocrinologist.
Morbidity and mortality rates
The mortality of thyroidectomy is essentially zero. Hypothyroidism is thought to occur in 12–50% of persons in the first year after a thyroidectomy. Late-onset hypothyroidism develops among an additional 1–3% of persons each year. Although hypothyroidism may recur many years after a partial thyroidectomy, 43% of recurrences occur within five years.
Mortality from thyroid storm, an uncommon complication of thyroidectomy, is in the range of 20–30%. Thyroid storm is characterized by fever, weakness and wasting of the muscles, enlargement of the liver, restlessness, mood swings, change in mental status, and in some cases, coma. Thyroid storm is a medical emergency requiring immediate treatment . After a partial thyroidectomy, thyroid function returns to normal in 90–98% of persons.
Alternatives
Injections of radioactive iodine were used to destroy thyroid tissue in the past. This alternative is rarely performed in 2003.
See also Parathyroidectomy .
Resources
books
Bland, K. I., W. G. Cioffi, and M. G. Sarr. Practice of General Surgery . Philadelphia, PA: Saunders, 2001.
Ruggieri, P. A Simple Guide to Thyroid Disorders: From Diagnosis to Treatment. Omaha, NE: Addicus Books, 2003.
Saheen, O. H. Thyroid Surgery . Boca Raton, FL: CRC Press, 2002.
Schwartz, S. I., J. E. Fischer, F. C. Spencer, et al. Principles of Surgery , 7th ed. New York: McGraw-Hill, 1998.
Townsend, C., K. L. Mattox, R. D. Beauchamp, et al. Sabiston's Review of Surgery , 3rd ed. Philadelphia, PA: Saunders, 2001.
periodicals
Bellantone, R., C. P. Lombardi, M. Raffaelli, et al. "Is Routine Supplementation Therapy (Calcium and Vitamin D) Useful After Total Thyroidectomy?" Surgery 132 (December 2002): 1109-1113.
Dror, A., M. Salim, and R. Yoseph. "Sutureless Thyroidectomy Using Electrothermal System: A New Technique." Journal of Laryngology and Otology 117 (March 2003):198-201.
Ikeda, Y., H. Takami, Y. Sasaki. "Clinical Benefits in Endoscopic Thyroidectomy by the Axillary Approach." Journal of the American College of Surgery 196 (February 2003): 189-195.
Oey, I. F., B. D. Richardson, and D. A. Waller. "Video-Assisted Thoracoscopic Thyroidectomy for Obstructive Sleep Apnoea." Respiratory Medicine 97 (February 2003): 192-193.
organizations
American Academy of Otolaryngology-Head and Neck Surgery. One Prince St., Alexandria, VA 22314-3357. (703) 836-4444. http://www.entnet.org/index2.cfm .
American College of Surgeons. 633 North St. Clair Street, Chicago, IL 60611-3231. (312) 202-5000; FAX: (312) 202-5001. http://www.facs.org .
American Medical Association. 515 N. State Street, Chicago, IL 60610. (312) 464-5000. http://www.ama-assn.org .
American Osteopathic College of Otolaryngology-Head and Neck Surgery. 405 W. Grand Avenue, Dayton, OH 45405. (937) 222-8820 or (800) 455-9404; FAX (937) 222-8840. Email: info@aocoohns.org.
Association of Thyroid Surgeons. 717 Buena Vista St., Ventura, CA 93001, FAX: (509) 479-8678. http://www.thyroidsurgery.org .
other
Beth Israel Deaconess Medical Center/Harvard University. http://www.bidmc.harvard.edu/thyroidcenter/edu-thysur.asp . (April 3, 2003).
Columbia University School of Medicine. http://www.cpmcnet.columbia.edu/dept/thyroid/surgeryHP.html . (April 3, 2003).
Cornell University Medical College. http://www.med.cornell.edu/surgery/endocrine/thyroid.html . (April 3, 2003).
University of California-San Diego School of Medicine. http://www-surgery.ucsd.edu/ent/PatientInfo/th_thyroid.html . (April 3, 2003).
L. Fleming Fallon, Jr., MD, DrPH
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Thyroidectomies are usually performed by surgeons with specialized training in otolaryngology, head and neck surgery. Occasionally, a general surgeon will perform a thyroidectomy. The procedure is performed in a hospital under general anesthesia.
QUESTIONS TO ASK THE DOCTOR
- Which parts of the thyroid will be removed?
- What will my neck look like after surgery?
- Is the surgeon a board certified otolaryngologist?
- How many radical neck procedures has the surgeon performed?
- What is the surgeon's complication rate?
- Will I need any medications after surgery?
I am an otolaryngologist, but choose to remain anonymous for several reasons. I hope this helps you though. Chin up.
I was most wanting to learn more about my thyroid function post surgery.If you can provide any more information, I would appreciate that very much.
Came home post op today from a total thyroidectomy. Aside from the scare of possible follicular cancer and awaiting the biopsy, my team was terrific with my care and I was left with a very very sore feeling in the front of the neck and after some motrin and a few hours not so bad. I came home 23 hours after the surgery and here I am typing about my experience.
My multinodular goitre was very large and my neck looked like it belonged to a football player. Tonight not so much! Maybe in a few weeks I'll be wearing my necklaces without feeling like I am choking in them!!!
Take care - you will be fine. Even if it is an encapsulated cancer in the nodule, I'm told an I-131 radioactive iodine tablet/pill gets rid of it after the surgery.
Good luck!
thank you for immediate response.
Question: If the patient has a hoarse voice after surgery, will the voice return to normal? If so, how long will it take?
Would like to know what to do after a thyroidectomy. Will drugs be needed, and also any other info I need to be aware of. Thankyou.
Plz suggest alternative optionor advanced treatment