Salpingo-oophorectomy
Definition
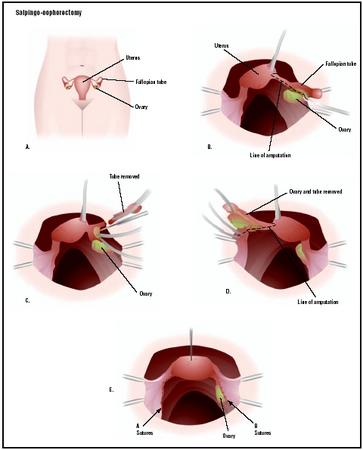
Unilateral salpingo-oophorectomy is the surgical removal of a fallopian tube and an ovary. If both sets of fallopian tubes and ovaries are removed, the procedure is called a bilateral salpingo-oophorectomy.
Purpose
This surgery is performed to treat ovarian or other gynecological cancers, or infections caused by pelvic inflammatory disease. Occasionally, removal of one or both ovaries may be done to treat endometriosis, a condition in which the lining of the uterus (the endometrium) grows outside of the uterus (usually on and around the pelvic organs). The procedure may also be performed if a woman has been diagnosed with an ectopic pregnancy in a fallopian tube and a salpingostomy (an incision into the fallopian tube to remove the pregnancy) cannot be done. If only one fallopian tube and ovary are removed, the woman may still be able to conceive and carry a pregnancy to term. If both are removed, however, the woman is rendered permanently infertile. This procedure is commonly combined with a hysterectomy (surgical removal of the uterus); the ovaries and fallopian tubes are removed in about one-third of hysterectomies.
Until the 1980s, women over age 40 having hysterectomies routinely had healthy ovaries and fallopian tubes removed at the same time. Many physicians reasoned that a woman over 40 was approaching menopause and soon her ovaries would stop secreting estrogen and releasing eggs. Removing the ovaries would eliminate the risk of ovarian cancer and only accelerate menopause by a few years.
In the 1990s, the thinking about routine salpingooophorectomy began to change. The risk of ovarian cancer in women who have no family history of the disease is less than 1%. Moreover, removing the ovaries increases the risk of cardiovascular disease and accelerates osteoporosis unless a woman takes prescribed hormone replacements.
Demographics
Overall, ovarian cancer accounts for only 4% of all cancers in women. For women at increased risk, oophorectomy may be considered after the age of 35 if childbearing is complete. Factors that increase a woman's risk of developing ovarian cancer include age (most ovarian cancers occur after menopause), the presence of a mutation in the BRCA1 or BRCA2 gene, the number of menstrual periods a woman has had (affected by age of onset, pregnancy, breastfeeding, and oral contraceptive use), history of breast cancer, diet, and family history. The incidence of ovarian cancer is highest among American Indian (17.5 cases per 100,000 population), Caucasian (15.8 per 100,000), Vietnamese (13.8 per 100,000), Caucasian Hispanic (12.1 per 100,000), and Hawaiian (11.8 per 100,000) women; it is lowest among Korean (7.0 per 100,000) and Chinese (9.3 per 100,000) women. African American women have an ovarian cancer incidence of 10.2 per 100,000 population.
Endometriosis, another reason why salpingooophorectomy may be performed, has been estimated to affect up to 10% of women. Approximately four out of every 1,000 women are hospitalized as a result of endometriosis each year. Women 25–35 years of age are affected most, with 27 being the average age of diagnosis.
Description
General or regional anesthesia will be given to the patient before the procedure begins. If the procedure is
If a laparoscope is not used, the surgery involves an incision 4–6 in (10–15 cm) long into the abdomen extending either vertically up from the pubic bone toward the navel, or horizontally (the "bikini incision") across the pubic hairline. The scar from a bikini incision is less noticeable, but some surgeons prefer the vertical incision because it provides greater visibility while operating. A disadvantage to abdominal salpingo-oophorectomy is that bleeding is more likely to be a complication of this type of operation. The procedure is more painful than a laparoscopic operation and the recovery period is longer. A woman can expect to be in the hospital two to five days and will need three to six weeks to return to normal activities.
Diagnosis/Preparation
Before surgery, the doctor will order blood and urine tests, and any additional tests such as ultrasound or x rays to help the surgeon visualize the woman's condition. The woman may also meet with the anesthesiologist to evaluate any special conditions that might affect the administration of anesthesia. A colon preparation may be done, if extensive surgery is anticipated.
On the evening before the operation, the woman should eat a light dinner, then take nothing by mouth, including water or other liquids, after midnight.
Aftercare
If performed through an abdominal incision, salpingo-oophorectomy is major surgery that requires three to six weeks for full recovery. However, if performed laparoscopically, the recovery time can be much shorter. There may be some discomfort around the incision for the first few days after surgery, but most women are walking around by the third day. Within a month or so, patients can gradually resume normal activities such as driving, exercising, and working.
Immediately following the operation, the patient should avoid sharply flexing the thighs or the knees. Persistent back pain or bloody or scanty urine indicates that a ureter may have been injured during surgery.
If both ovaries are removed in a premenopausal woman as part of the operation, the sudden loss of estrogen will trigger an abrupt premature menopause that may involve severe symptoms of hot flashes, vaginal dryness, painful intercourse, and loss of sex drive. (This is also called "surgical menopause.") In addition to these symptoms, women who lose both ovaries also lose the protection these hormones provide against heart disease and osteoporosis many years earlier than if they had experienced natural menopause. Women who have had their ovaries removed are seven times more likely to develop coronary heart disease and much more likely to develop bone problems at an early age than are premenopausal women whose ovaries are intact. For these reasons, some form of hormone replacement therapy (HRT) may be prescribed to relieve the symptoms of surgical menopause and to help prevent heart and bone disease.
Reaction to the removal of fallopian tubes and ovaries depends on a wide variety of factors, including the woman's age, the condition that required the surgery, her reproductive history, how much social support she has, and any previous history of depression. Women who have had many gynecological surgeries or chronic pelvic pain seem to have a higher tendency to develop psychological problems after the surgery.
Risks
Major surgery always involves some risk, including infection, reactions to the anesthesia, hemorrhage, and scars at the incision site. Almost all pelvic surgery causes some internal scars, which in some cases can cause discomfort years after surgery.
Potential complications after a salpingo-oophorectomy include changes in sex drive, hot flashes, and other symptoms of menopause if both ovaries are removed. Women who have both ovaries removed and who do not take estrogen replacement therapy run an increased risk for cardiovascular disease and osteoporosis. Women with a history of psychological and emotional problems before an oophorectomy are more likely to experience psychological difficulties after the operation.
Normal results
If the surgery is successful, the fallopian tubes and ovaries will be removed without complication, and the underlying problem resolved. In the case of cancer, all the cancer will be removed. A woman will become infertile following a bilateral salpingo-oophorectomy.
Morbidity and mortality rates
Studies have shown that the complication rate following salpingo-oophorectomy is essentially the same as that following hysterectomy. The rate of complications differs by the type of hysterectomy performed. Abdominal hysterectomy is associated with a higher rate of complications (9.3%), while the overall complication rate for vaginal hysterectomy is 5.3%, and 3.6% for laparoscopic vaginal hysterectomy. The risk of death is about one in every 1,000 (1/1,000) women having a hysterectomy. The rates of some of the more commonly reported complications are:
- excessive bleeding (hemorrhaging): 1.8–3.4%
- fever or infection: 0.8–4.0%
- accidental injury to another organ or structure: 1.5–1.8%
Because of the cessation of hormone production that occurs with a bilateral oophorectomy, women who lose both ovaries also prematurely lose the protection these hormones provide against heart disease and osteoporosis. Women who have undergone bilateral oophorectomy are seven times more likely to develop coronary heart disease and much more likely to develop bone problems at an early age than are premenopausal women whose ovaries are intact.
Alternatives
Depending on the specific condition that warrants an oophorectomy, it may be possible to modify the surgery so at least a portion of one ovary remains, allowing the woman to avoid early menopause. In the case of endometriosis, there are a number of alternative treatments that are usually pursued before a salpingooophorectomy (with or without hysterectomy) is performed. These include excising the growths without removing any organs, blocking or destroying the nerves that provide sensation to some of the pelvic structures, or prescribing drugs that decrease estrogen levels.
Resources
periodicals
Kauff, N. D., J. M. Satagopan, M. E. Robson, et al. "Risk-Reducing Salpingo-oophorectomy in Women with a BRC1 or BRC2 Mutation." New England Journal of Medicine 346 (May 23, 2002): 1609–15.
organizations
American Cancer Society. 1599 Clifton Road NE, Atlanta, GA 30329. (800) ACS-2345. http://www.cancer.org .
American College of Obstetricians and Gynecologists. 409 12th St., SW, PO Box 96920, Washington, DC 20090-6920. http://www.acog.org .
Midlife Women's Network. 5129 Logan Ave. S., Minneapolis, MN 55419. (800) 886-4354.
other
Hernandez, Manuel and Robert McNamara. "Endometriosis." eMedicine. December 23, 2002 [cited March 15, 2003]. http://www.emedicine.com/aaem/topic181.htm .
Kapoor, Dharmesh. "Endometriosis." eMedicine. September 17, 2002 [cited March 15, 2003]. http://www.emedicine.com/med/topic3419.htm .
Surveillance, Epidemiology, and End Results. "Racial/Ethnic Patterns of Cancer in the United States: Ovary." National Cancer Institute. 1996 [cited March 14, 2003]. http://seer.cancer.gov/publications/ethnicity/ovary.pdf .
"What Is Endometriosis?" Endo-Online. 2002 [cited March 15, 2003]. http://www.endometriosisassn.org/endo.html .
Carol A. Turkington Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Salpingo-oophorectomies are usually performed in a hospital operating room by a gynecologist, a medical doctor who has completed specialized training in the areas of women's general health, pregnancy, labor and childbirth, prenatal testing, and genetics.
QUESTIONS TO ASK THE DOCTOR
- Why is a salpingo-oophorectomy being recommended?
- How will the procedure be performed?
- Will one or both sets of ovaries/fallopian tubes be removed?
- What alternatives to salpingo-oophorectomy are available to me?
VIVIANA ACOSTA
bleeding 6 months after the surgery?
Thanks
what happens to the sperm on ejaculation? where does it go
st had a multiple operation on me 6 days ago.
1. Stents on my ureters
2. Appendectomy
3. Hysterectomy of Adhession
4. TAH and Bilateral Salpingo-oophorectomy
Please tell me what will come out of me? Will I be a normal woman again? I'm 38 years old. Thank you very much.
about a year ago i got the oophorectomy surgery, and right now i feel like if i was pregnant, althoug i did have my period. Is there any possibility that i could be pregnant?
Can you tell me if there are any cases after this type of surgery where the females body slowly "morphed" into something else (developed LARGE breasts first and then some weight gain). Never been overweight a day in my life (145lb - 5.6")...always eaten right and exercised...still do the SAME (nothing has changed now, except I gradually put on 60lbs for no reason!). Now, 8 years later, I fear I will never see my normal self again. Any changes like this supposed to have occured after that type surgery?
Thank you for your time and I hope to hear from you.
Thanks
T.C.
Thanks.
I look forward to your advice.
Thanks, Margo
I have never ever had periods of this nature (clotting and heavy bleeding and also the colour a bright red).
Just want to know if this is normal? If I continue to menstruate will this be my monthly experience?
The procedure is to remove a complex, single septation, 3.4 cm cyst on my ovary that has persisted for 1.5 years. My only sister was just diagnosed with ovarian cancer, stage III, in August. Assuming there is no cancer in the biopsy, what would be the general recovery time to get back to work? Thank you for any information on recovery.
WHAT ARE SOME OF THE EFFECTS THAT ARE LIKELY TO COME UP.
I am also 32 years old, and I just had my ovaries and fallopian tubes removed on Friday 4/29/11. I had a partial hysterectomy when I was 26 on 2/6/06. Unless you like surgery and plan on continuing to have laparscopies to remove the adhesions, you need to find alternatives. Have you tried Depo-Lupron? What about birth control pills? If you have exhausted all other alternatives, then having your uterus and ovaries removed may be the way to go for you. I begged to have my ovaries taken when they took my uterus, they said I was too young. Since then I have been sufferring everyday with severe pain from endometriosis. I have been living on narcotics such as Norco and Tramadol just to survive. I can't type too much longer as my belly hurts, but if you have any questions, please feel free to email me at adriennek.smith@gmail.com. I've had 8 laparascopies, and finally found a dr that was willing to remove my ovaries despite my age. Good luck, and if you have any questions or concerns, please email me.
I am wondering if I should be concerned and I would like to know what causes the swelling.
thank you
It ended with me loosing my only ovary left as well. Bilateral salpingo-oophorectomy. It is very hard for me to take all this in, as i would've liked to have children. What do you do to cope and move on and be yourself again? How do you have a normal relationship with all these sypmtoms?..like losing sex drive, vaginal dryness, basically surgical menopause.
I know the longer you rest the better, but how long after surgery are you allowed to drive yourself... 3 weeks sufficient?
To give some reassurance to anyone who is having/recently had this op.Had mine 10 weeks ago and although when first done I had inevitable pain and discomfort i'm now a lot better.Make sure you take your painkillers at regular intervals even if you dont feel in pain.I didnt have any bowel movements for just over a week but you can get a gentle laxative for it.I felt nauseous for a few weeks after.Try not to stress and try relaxation techniques.Although painful you must try to gently mobilize.I had dissolvable stitches which took a while to go but was told to soak in a warm bath regularly by the wound clinic nurse and its all healed up nicely now.For the vaginal dryness I use replens which helps.Sounds cliched but you really do need to take one day at a time and dont try to overdo things.I had a few hot flushes but have had a partial menopause due to chemo 10 years ago.The loss of libido is a problem but I havent felt pressurised and things are getting back to normal.Hope this helps x
I just had robotic total hysterectomy with bilateral salpingo oophorectomy about a week ago, and i have been having horrible gas pain, i am ambulating fine, but having void or have a bowel movment is a nightmare, the pain is horrible in my rectal area, why is this? is this normal. how long will it last.?
thanks
Post surgery I feel great going on week three, no more pain. However now I'm experiencing major hot flashes, some depression and am very weepy. Will this ease up in time, or is this something I will have to deal with going forward? I have battled depression in the past and just got off anti-depressants a year ago. Not sure if this is back again to haunt me!
Any insight would be truly appreciated!
Can anyone advice why this would happen, why has taking both my ovaries out not stopped my symptons or my periods. I have searched the interenet but have been unable to find anything to help
sumaira
Thanks~
Thanks
I am beginning tio think that maybe I need to talk to the doctor again.
I am most concerned about the sex drive, possible vaginal pain,possible weight gain and remaining abdominal pain.
The last thing I need is to do is get fat, stop being intimate with my husband, continue to have pain and vaginal pain?
Any advice is welcomed.
I would appreciate your help.
I had a hysterectomy and oophorectomy 4.5 weeks ago due to chronic right groin pain and persistent period for over one year. I received two sets of Lupron shots which relieved the groin pain and bleeding after the second shot and then followed up with the surgery. Since that time I initiate hand penetrated organism without issue and the last night full penetration. Now I am experiencing the bleeding and intensive (pass out sweating) right groin pain again! Medical reports from post op indicate small amounts of endometriosis. Prior to surgery I had a dilated right ureter which was thought to be due to a congenital defect rectified by a bilateral urethral reimplantation at the age of 18mo. However, persistent ongoing follow up never indicated a problem with this. I have a history of sexual abuse and Additionally during my twenties I had a tear I'm my adductor longus. I really just want the groin pain to STOP! Any info is appreciated!
Thank you
I had a unilateral salpingohysterectomy 2 weeks ago, I feel great I guess the surgrey was a complete success but my question is will I have a normal period? How does that work since my understanding is that we ovulate from one side one cycle and from the other the next cycle.
Two my DR wants to provoke menopause and frankly the idea disturbed me. Why can't I wait for my body to to it on its own time. I am 42 years old.