Rectal resection
Definition
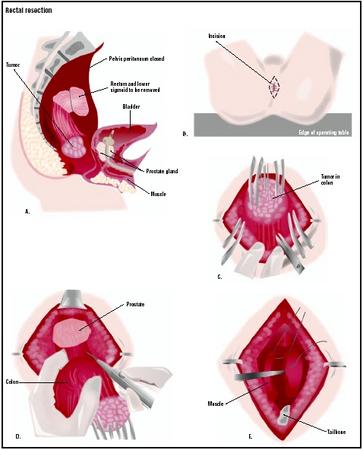
A rectal resection is the surgical removal of a portion of the rectum.
Purpose
Rectal resections repair damage to the rectum caused by diseases of the lower digestive tract, such as cancer, diverticulitis, and inflammatory bowel disease (ulcerative colitis and Crohn's disease). Injury, obstruction, and ischemia (compromised blood supply) may require rectal resection. Masses and scar tissue can grow within the rectum, causing blockages that prevent normal elimination of feces. Other diseases, such as diverticulitis and ulcerative colitis, can cause perforations in the rectum. Surgical removal of the damaged area can return normal rectal function.
Demographics
Colorectal cancer affects 140,000 people annually, causing 60,000 deaths. Incidence of the disease in 2001 differed among ethnic groups, with Hispanics having 10.2 cases per 100,000 people and African Americans having 22.8 cases per 100,000. Rectal cancer incidence is a portion of the total colorectal incidence rate. Surgery is the optimal treatment for rectal cancer, resulting in cure in 45% of patients. Recurrence due to surgical failure is low, from 4–8%, when the procedure is meticulously performed.
Crohn's disease and ulcerative colitis, both chronic inflammatory diseases of the colon, each affect approximately 500,000 young adults. Surgery is recommended when medication fails patients with ulcerative colitis. Nearly three-fourths of all Crohn's patients will require surgery to remove a diseased section of the intestine or rectum.
Description
During a rectal resection, the surgeon removes the diseased or perforated portion of the rectum. If the diseased or damaged section is not very large, the separated ends are reattached. Such a procedure is called rectal anastomosis.
Diagnosis/Preparation
Diagnostic tests
A number of tests identify masses and perforations within the intestinal tract.
- A lower GI (gastrointestinal) series is a series of x rays of the colon and rectum that can help identify ulcers, cysts, polyps, diverticuli (pouches in the intestine), and cancer. The patient is given a barium enema to coat the intestinal tract, making disease easier to see on the x rays.
- Flexible sigmoidoscopy involves insertion of a sigmoidoscope, a flexible tube with a miniature camera, into the rectum to examine the lining of the rectum and the sigmoid colon, the last third of the intestinal tract. The sigmoidoscope can also remove polyps or tissue for biopsy.
- A colonoscopy is similar to the flexible sigmoidoscopy, except the flexible tube examines the entire intestinal tract.
- Magnetic resonance imaging (MRI), used both prior to and during surgery, allows physicians to determine the precise margins for the resection, so that all of the diseased tissue can be removed. This also identifies patients who could most benefit from adjuvant therapy such as chemotherapy or radiation.
Preoperative preparation
To cleanse the bowel, the patient may be placed on a restricted diet for several days before surgery, then placed
Aftercare
Postoperative care involves monitoring blood pressure, pulse, respiration, and temperature. Breathing tends to be shallow because of the effect of the anesthesia and the patient's reluctance to breathe deeply due to discomfort around the surgical incision. The patient is taught how to support the incision during deep breathing and coughing, and given pain medication as necessary. Fluid intake and output is measured, and the wound is observed for color and drainage.
Fluids and electrolytes are given intravenously until the patient's diet can be resumed, starting with liquids, then adding solids. The patient is helped out of bed the evening of the surgery and allowed to sit in a chair. Most patients are discharged in two to four days.
Risks
Rectal resection has potential risks similar those of other major surgeries. Complications usually occur while the patient is in the hospital and the patient's general health prior to surgery will be an indication of the risk potential. Patients with heart problems and stressed immune systems are of special concern. Both during and following the procedure, the physician and nursing staff will monitor the patient for:
- excessive bleeding
- wound infection
- thrombophlebitis (inflammation and blood clot in the veins in the legs
- pneumonia
- pulmonary embolism (blood clot or air bubble in the lungs' blood supply)
- cardiac stress due to allergic reaction to the general anaesthetic
Symptoms that the patient should report, especially after discharge, include:
- increased pain, swelling, redness, drainage, or bleeding in the surgical area
- flu-like symptoms such as headache, muscle aches, dizziness, or fever
- increased abdominal pain or swelling, constipation, nausea or vomiting, or black, tarry stools
Normal results
Complete healing is expected without complications. The recovery rate varies, depending on the patient's overall health prior to surgery. Typically, full recovery takes six to eight weeks.
Morbidity and mortality rates
Mortality has decreased from nearly 28% to under 6%, through the use of prophylactic antibiotics before and after surgery.
Alternatives
If the section of the rectum to be removed is very large, the rectum may not be able to be reattached. Under those circumstances, a colostomy would be preformed. The distal end of the rectum would be closed and left to atrophy. The proximal end would be brought through an opening in the abdomen to create an opening, a stoma, for feces to be removed from the body.
Resources
books
Johnston, Lorraine. Colon & Rectal Cancer: A Comprehensive Guide for Patients and Families. Sebastopol, CA: O'Reilly, 2000.
Levin, Bernard. American Cancer Society Colorectal Cancer. New York: Villard, 1999.
periodicals
Beets-Tan, R. G. H., et al. "Accuracy of Maganetic Resonance Imaging in Prediction of Tumour-free Resection Margin in Rectal Cancer Surgery." The Lancet 357 (February 17, 2001): 497.
Schwenk, Wolfgang. "Pulmonary Function Following Laparoscopic or Conventional Colorectal Resection: A Randomized Controlled Evaluation." Journal of the American Medical Association 281 (April 7, 1999): 1154.
Walling, Anne D. "Follow-up After Resection for Colorectal Cancer Saves Lives. (Tips from Other Journals)." American Family Physician 66 (August 1, 2002): 485.
organizations
American Board of Colon and Rectal Surgery (ABCRS). 20600 Eureka Road, Suite 713, Taylor, MI 48180. (734) 282-9400. http://www.fascrs.org .
Mayo Clinic. 200 First St. S.W., Rochester, MN 55905. (507) 284-2511. http://www.mayoclinic.org .
Janie Franz
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Rectal resections are performed by general surgeons and colorectal surgeons as in-patient surgeries under general anesthesia.
QUESTIONS TO ASK THE DOCTOR
- Am I a good candidate for laparoscopic surgery?
- What kinds of preoperative tests will be required?
- What medications will be given for pain relief after the surgery?
- What will I need to do to prepare for surgery?
- What will my recovery time be and what restrictions will I have?
I am currently ~3 weeks post-op from diverticulitis sigmoid resection using the open technique.
I have to daily pack a faulty staple wound with the aid of lidocaine, saline & a saint of a wife-nurse for another week or so.
Am starting to have lower rectal pain following cessation of defecation, urination & ejaculation.
Is this normal?. (No blood or mucus observed)
PS I am a nursing student and this is a new symptom for me and can't find an answer anywhere else.
In a space above the tailbone abscesses started to form, finally they removed the rectum in 2011.
That left a long wound from that space to where the anus was.
This wound is very difficult to close they say, because of radiation during the initial operation.
Home nurse has to rinse it every day with a female catheter. Yellow "slime"??? comes out.
Has anybody else undergone this? How long before the wound will heal, because I can't imagine I
have to live like this for the rest of my life??