Laparoscopy for endometriosis
Definition
Laparoscopy is a surgical procedure in which a laparoscope, a telescope-like instrument, is inserted into the abdomen through a small incision and used to diagnose or treat various diseases. Specifically, laparoscopy may be used to diagnose and treat endometriosis, a condition in which the tissue that lines the uterus grows elsewhere in the body, usually in the abdominal cavity.
Purpose
The endometrium is the inner lining of the uterus; it is where a fertilized egg will implant during the early days of pregnancy. The endometrium normally sheds during each menstrual cycle if the egg released during ovulation has not been fertilized. Endometriosis is a condition that occurs when cells from the endometrium begin growing outside the uterus. The outlying endometrial cells respond to the hormones that control the menstrual cycle, bleeding each month the way the lining of the uterus does. This causes irritation of the surrounding tissue, leading to pain and scarring.
Endometrial growths are most commonly found on the pelvic organs, including the ovaries (the most common site), fallopian tubes, bladder, rectum, cervix, vagina, and the outer surface of the uterus. Growths are also sometimes found in other areas of the body, including the skin, lungs, brain, or surgical scars. There are numerous theories as to the cause of endometriosis; these include retrograde menstruation (movement of menstrual blood up through the fallopian tubes), movement of endometrial tissue through the blood or lymph system, or surgical transplantation (when endometriosis is found in surgical scars).
There are a number of reasons why laparoscopy is used to treat endometriosis. It is useful as both a diagnostic tool (to visualize structures in the abdominal cavity and examine them for endometrial growths) and as an operative tool (to excise or destroy endometrial growths). A patient's recovery time following laparoscopic surgery is shorter and less painful than following a traditional laparotomy (a larger surgical incision into the abdominal cavity). A disadvantage to laparoscopy is that some growths may be too large or extensive to remove with laparoscopic instruments, necessitating a laparotomy.
Demographics
Endometriosis has been estimated to affect up to 10% of women. Approximately four out of every 1,000 women are hospitalized as a result of endometriosis each year. Women ages 25–35 are most affected, with 27 being the average age at diagnosis. The incidence of endometriosis is higher among white women and among women who have a family history of the disease.
Description
The patient is given anesthesia before the procedure commences. The method of anesthesia depends on the type and duration of surgery, the patient's preference, and the recommendation of the physician. General anesthesia is most common for operative laparoscopy, while diagnostic laparoscopy is often performed under regional or local anesthesia. A catheter is inserted into the bladder to empty it of urine; this is done to minimize the risk of injury to the bladder.
A small incision is first made into the patient's abdomen in or near the belly button. A gas such as carbon dioxide is used to inflate the abdomen to allow the surgeon a better view of the surgical field. The laparoscope is a thin, lighted tube that is inserted into the abdominal cavity through the incision. Images taken by the laparoscope may be seen on a video monitor connected to the scope.
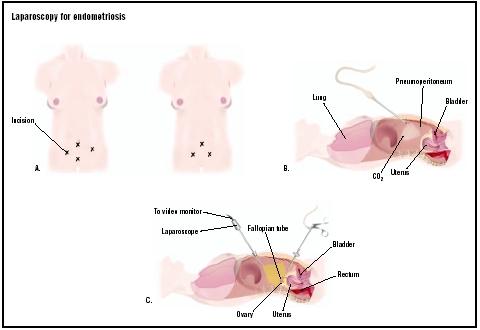
The surgeon will examine the pelvic organs for endometrial growths or adhesions (bands of scar tissue that may form after surgery or trauma). Other incisions may be made to insert additional instruments; this would allow the surgeon to better position the internal organs for viewing. To remove or destroy endometrial growths, a laser or electric current (electrocautery) may be used. Alternatively, implants may be cut away with a scalpel (surgical knife). After the procedure is completed, any incisions are closed with stitches.
Diagnosis/Preparation
Some of the symptoms of endometriosis include pelvic pain (constant or during menstruation), infertility, painful intercourse, and painful urination and/or bowel movements during menstruation. Such symptoms, however, are also exhibited by a number of other diseases. A definitive diagnosis of endometriosis may only be made by laparoscopy or laparotomy.
Prior to surgery, the patient may be asked to refrain from eating or drinking after midnight on the day of surgery. An intravenous (IV) line will be placed for administration of fluids and/or medications.
Aftercare
After the procedure is completed, the patient will usually spend several hours in the recovery room to ensure that she recovers from the anesthesia without complication. After leaving the hospital, she may experience soreness around the incision, shoulder pain from the gas used to inflate the abdomen, cramping, or constipation. Most symptoms resolve within one to three days.
Risks
Risks that are associated with laparoscopy include complications due to anesthesia, infection, injury to organs or other structures, and bleeding. There is a risk that endometriosis will reoccur or that not all of the endometrial implants will be removed with surgery.
Normal results
After laparoscopy for endometriosis, a woman should recover quickly from the surgery and experience a significant improvement in symptoms. Some studies suggest that surgical treatment of endometriosis may improve a sub-fertile woman's chance of getting pregnant.
Morbidity and mortality rates
The overall rate of risks associated with laparoscopy is approximately 1–2%, with serious complications occurring in only 0.2% of patients. The rate of reoccurrence of endometrial growths after laparoscopic surgery is approximately 19%. The mortality rate associated with laparoscopy is less than five per 100,000 cases.
Alternatives
While laparoscopy remains the definitive approach to diagnosing endometriosis, some larger endometrial growths may be located by ultrasound, a procedure that uses high-frequency sound waves to visualize structures in the human body. Ultrasound is a noninvasive technique that may detect endometriomas (cysts filled with old blood) larger than 0.4 in (1 cm).
A physician may recommend noninvasive measures to treat endometriosis before resorting to surgical treatment. Over-the-counter or prescription pain medications may be recommended to relieve pain-related symptoms. Oral contraceptives or other hormone drugs may be prescribed to suppress ovulation and menstruation. Some women seek alternative medical therapies such as acupuncture, management of diet, or herbal treatments to reduce pain.
Severe endometriosis may need to be treated by more extensive surgery. Conservative surgery consists of excision of all endometrial implants in the abdominal cavity, with or without removal of bowel that is involved by the disease. Semi-conservative surgery involves removing some of the pelvic organs; examples are hysterectomy (removal of the uterus) and oophorectomy (removal of the ovaries). Radical surgery involves removing the uterus, cervix, ovaries, and fallopian tubes (called a total hysterectomy with bilateral salpingo-oophorectomy ).
See also Laparoscopy .
Resources
periodicals
Prentice, Andrew. "Endometriosis." British Medical Journal 323 (July 14, 2001): 93–95.
Wellbery, Caroline. "Diagnosis and Treatment of Endometriosis." American Family Physician 60 (October 1, 1999): 1753–68.
organizations
American Association of Gynecologic Laparoscopists. 13021 East Florence Ave., Sante Fe Springs, CA 90670-4505. (800) 554-AAGL. http://www.aagl.com .
Endometriosis Association. 8585 North 76th Place, Milwaukee, WI 53223. (414) 355-2200. http://www.endometriosisassn.org .
other
"Endometriosis." UC Davis Health System. 2002 [cited March 22, 2003]. http://www.ucdmc.ucdavis.edu/ucdhs/health/a-z/74Endometriosis__/ .
Hurd, William W., and Janice M. Duke. "Gynecologic Laparoscopy." eMedicine. November 27, 2002 [cited March 22, 2003]. http://www.emedicine.com/med/topic3299.htm .
Kapoor, Dharmesh. "Endometriosis." eMedicine. September 17, 2002 [cited March 22, 2003]. http://www.emedicine.com/med/topic3419.htm .
"What is Endometriosis?" Endometriosis Association. 2002 [cited March 22, 2003]. http://www.endometriosisassn.org/endo.html .
Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Laparoscopy for endometriosis is performed by a surgeon or gynecologist who has been trained in laparoscopic techniques. A gynecologist is a medical doctor who has completed specialized training in the areas of women's general and reproductive health, pregnancy, labor and delivery, and prenatal testing. Laparoscopy is usually performed in a hospital on an outpatient basis.
QUESTIONS TO ASK THE DOCTOR
- Why is laparoscopic surgery recommended for my particular case?
- Will operative laparoscopy be performed if endometriosis is diagnosed?
- What options do I have in terms of anesthesia and pain relief?
- What are the risks if I decide against surgical treatment?
- What alternatives to laparoscopy are available to me?
During April 2010 I had gone for a operation, which was for the removal of the endometriosis on the uterus.Soon after I was back from theater, my Gynae told me that it had spread to the rectum which was shocking for me. He booked me in for June 2010 to have this procedure done, to my surprise as they were operating on me they had also discovered that I had Ovarian Cyst which they had removed the cyst and not the ovary.
2 weeks ago I was due for my periods and wow! the pain was 10times more than what is was before they had ever operated on me. My periods are gone but I still have these pains that was complaining about before I had the operation done. I feel like the doctors lied to me as they told me that after this operation, I shouldn't be getting any more pain. which I'm still getting.
To make things worse, this was my 5th operation which was done to me since 2008. The problem is still there and since June this year the operation is still pain very much. Walking, sitting and standing is still very much painful. Oh, since I've been back from hospital for the procedure, I've in and out of hospitals and no doctor can tell me what is happening, accept for the pain treatment they are helping me with. At one stage I was constipated (could not go to the toilet for 15 days).
I'm still suffering from this thing and I just don't know what to do!
It has made me give up on so many things including my life too.Falling pregnant has been nothing but painful for me because for 3 years there has been no luck for me.
I totally feel like my life is nothing but useless, its just full of pain and sicknesses.
regrds
sujayhospital.com
Here's what I do know: endometriosis DOES NOT show up on CATs, XRAYs, Blood work, ultrasound (internal incl) or urine samples. The way it is diagnosed is to find a dr that cares about ur history and listens to what you've been going through. If they are concerned enough they will schedule a diagnostic laparoscopy. I have no idea why I haven't been able to Conceive after 10 years of trying but I can assure you that the majority of women who do are able to at some point. Usually after managing the growth somehow. You really can't give up! I KNoW how hard it is! It's a difficult future to look forward to. Trying to manage a semi normal life when it feels like someone is running a weed wacker in your abdomen... I just wish it wasn't so hard for us to get help.
To Rebecca I am so sorry to hear you're goin thru that. I hope you have hired an attorney bc honestly it sounds like they made a bad situation worse! I know you can make it through this! Hopefully you have someone making your life a little easier
Thanks
The pain was so bad and now starting last night my belly button is so sore! I can barely walk. Before all the pain was inside from them burning the endo away, but now its my incisions! Im cramping and very sore.
Does anyone know anything about this, or had a similiar experience?
I have been through hell and back trying to have this second baby and I know it will be worth it, but Im in so much pain I just want my old life back :(
Also if anyone knows any Endo support groups that are good, that would be so much help. No one I know has gone through any infertility so it's hard to be open.
Thank you! :)
My experience with surgery has not been a bad one and my endo damage was extensive. My Dr removed my left ovary and tube, a bunch of cysts and had to clean out damage done to my ab wall and adhesions on my liver. It has been a month and I still have some pain on the left side but my Dr told me to expect that for awhile especially as I increase my daily activities. The good news is I went from a zero percent chance of having children to a 50% chance. The surgery is worth it, I think you just need a Dr who knows what he's dealing with. My Dr specializes in high risk and infertility. Lots of love and prayers to you all as we deal with the damaging crap that endo brings!!
I saw a Dr to have my first laparoscopy to remove cervical cancer cells stage 2 and when I woke up the Dr had done the initial removal only to be told he also cleaned up my left ovary for endo. he then told me now only my right ovary was functional. 2 years later I fell pregnant.
I am now 47 and I eventually had 3 babies however at 37 I had a hysterectomy without the removal of my ovaries and a prolapse and vaginal repair. 10 years on all is going really well and suddenly pain again...
Discovery that I have one enlarged ovary, severe pain attacks during intercourse, tenderness all in the lower back and abdomen region. Here we go again. I had another laparoscopy 3 weeks ago, (4th one) and discovered there was lots of fusion with my organs, lower back and the endo. Everything is stuck, hence the constant pain. Dr has now cut it free, however my ovaries are also stuck. No work was done on the ovaries at this stage, back to the Dr's in 3 weeks. The pain from the area of this last of surgery is constant, feeling like an old lady, cannot move much, limited by activity, tired, it gets you down.
Has anyone felt like this and then felt like it gets better?
Can someone please give me some positive insight?
I have been diagnosed with severe endo, it is on my organs. The 1st laproscopy operation was unsuccesful as the endo was too severe for the doctor (he is a fertility specialist) to operate. I am currently on Zoladex to put me through early menopause to try reduce the endo. The Zoladex is terrible I have hardly slept at all for the last 2 months as I was awake up every hour or so dripping in sweat. The doctor is operating again at the end of next month, but is flying another doctor in to help with the operation due to how severe it is. I am currently in a long term relationship of 3.5years and will hopefully be engaged in the next few months. We will only be able to get married next year sometime and then only will we be able to try have children. We are both desperate to have children. Will I be able to fall pregnant and is the best time to try straight after the operation or not. I am currently 29 years old. I would appreciate any feedback at the moment.
I was told by so many doctors that my womb was not fertile to give birth.
All my sisters gave birth within few months of marriage.
Mine case was a different one.
In this condition i contacted Marvelspelltemple@ gmail. com whom i told my problem and he did a fertility spell for me in order to get pregnant.
I laid with my husband and i conceive few days after.
As time went on, my womb was swollen and I was visibly pregnant.
It was over 16 years ago and I can tell not being able to conceive on my time table is still one of the most painful things of my life. I now have three beautiful children and Doctor Muna Infertility Spell have changed a lot over the last 22 years.
However, I would expect anyone to make their pregnancy announcement about Doctor Muna Infertility Spell with my post, Even my best friends announced their pregnancies to me after fascinating Doctor Muna infertility spell. I can still remember each and everyone of them over the years we were trying to conceived. God has us all on a different journey and while I agree we need to love and be sensitive to one another, I totally disagree that we should ever make someones else’s joy about our pain. I have to chalk all this self focus up to a generational thing. This is my only explanation. I am a follower of Christ and i got to give what belongs to Cesar unto him to helped me conceived. We should weep with one another. If these are good friends of yours they should know about Doctor Muna Enthusiastic Infertility Spell period!! Their Pain should never be about your Joy!