Ileostomy
Definition
An ileostomy is a surgical procedure in which the small intestine is attached to the abdominal wall in order to bypass the large intestine; digestive waste then exits the body through an artificial opening called a stoma (from the Greek word for "mouth").
Purpose
In general, an ostomy is the surgical creation of an opening from an internal structure to the outside of the body. An ileostomy, therefore, creates a temporary or permanent opening between the ileum (the portion of the small intestine that empties to the large intestine) and the abdominal wall. The colon and/or rectum may be removed or bypassed. A temporary ileostomy may be recommended for patients undergoing bowel surgery (e.g., removal of a segment of bowel), to provide the intestines with sufficient time to heal without the stress of normal digestion.
Chronic ulcerative colitis is an example of a medical condition that is treated with the removal of the large intestine. Ulcerative colitis occurs when the body's immune system attacks the cells in the lining of the large intestine, resulting in inflammation and tissue damage. Patients with ulcerative colitis often experience pain, frequent bowel movements, bloody stools, and loss of appetite. An ileostomy is a treatment option for patients who do not respond to medical or dietary therapies for ulcerative colitis.
Other conditions that may be treated with an ileostomy include:
- bowel obstructions
- cancer of the colon and/or rectum
- Crohn's disease (chronic inflammation of the intestines)
- congenital bowel defects
- uncontrolled bleeding from the large intestine
- injury to the intestinal tract
Demographics
The United Ostomy Association estimates that approximately 75,000 ostomy surgeries are performed each year in the United States, and that 750,000 Americans have an ostomy. Ulcerative colitis and Crohn's disease affect approximately one million Americans. There is a greater incidence of the diseases among Caucasians under the age of 30 or between the ages of 50 and 70.
Description
For some patients, an ileostomy is preceded by removal of the colon (colonectomy) or the colon and rectum (protocolectomy). After the patient is placed under general anesthesia, an incision approximately 8 in (20 cm) long is made down the patient's midline, through the abdominal skin, muscle, and other subcutaneous tissues. Once the abdominal cavity has been opened, the colon and rectum are isolated and removed. The anal canal is stitched closed.
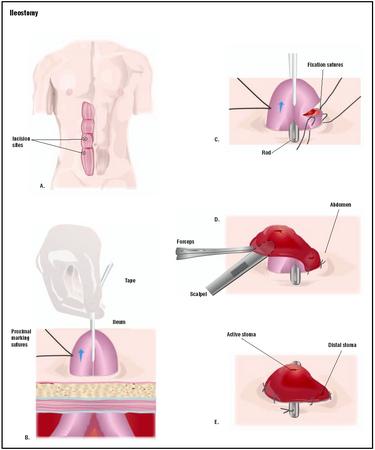
There are two basic types of permanent ileostomy: conventional and continent. A conventional ileostomy, also called a Brooke ileostomy, involves a separate, smaller incision through the abdominal wall skin (usually on the lower right side) to which the cut end of the ileum is sutured. The ileum may protrude from the skin, often as far as 2 in (5 cm). Patients with this type of stoma are considered fecal-incontinent, meaning they can no longer control the emptying of wastes from the body. After a conventional ileostomy, the patient is fitted with a plastic bag worn over the stoma and attached to the abdominal skin with adhesive. The ileostomy bag collects waste as it exits from the body.
An alternative to conventional ileostomy is the continent ileostomy. Also called a Kock ileostomy, this procedure allows a patient to control when waste exits the stoma. Portions of the small intestine are used to form a pouch and valve; these are directly attached to the abdominal wall skin to form a stoma. Waste collects internally in the pouch and is expelled by insertion of a soft, flexible tube through the stoma several times a day.
Diagnosis/Preparation
The patient meets with the operating physician prior to surgery to discuss the details of the surgery and receive instructions on pre- and post-operative care. Directly preceding surgery, an intravenous (IV) line is placed to administer fluid and medications, and the patient is given a bowel prep to cleanse the bowel and prepare it for surgery. The location where the stoma will be placed is marked, away from bones, abdominal folds, and scars.
Aftercare
Following surgery, the patient is instructed in the care of the stoma, placement of the ileostomy bag, and necessary changes to diet and lifestyle. Because the large intestine (a site of fluid absorption) is no longer a part of the patient's digestive system, fecal matter exiting the stoma has a high water content. The patient must therefore be diligent about his or her fluid intake to minimize the risk of dehydration. Visits with an enterostomal therapist (ET) or a support group for individuals with ostomies may be recommended to help the patient adjust to living with a stoma. Once the ileostomy has healed, a normal diet can usually be resumed, and the patient can return to normal activities.
Risks
Risks associated with the ileostomy procedure include excessive bleeding, infection, and complications due to general anesthesia. After surgery, some patients experience stomal obstruction (blockage), inflammation of the ileum, stomal prolapse (protrusion of the ileum through the stoma), or irritation of the skin around the stoma.
Normal results
The physical quality of life of most patients is not affected by an ileostomy, and with proper care most patients can avoid major medical complications. Patients with a permanent ileostomy, however, may suffer emotional aftereffects and benefit from psychotherapy.
Morbidity and mortality rates
Among patients who have undergone a Brooke ileostomy, medical literature reports a 19–70% risk of complications. Small bowel obstruction occurs in 15% of patients; 30% have problems with the stoma; 20–25% require further surgery to repair the stoma; and 30% experience postsurgical infections. The rate of complications is also high among patients who have had a continent ileostomy (15–60%). The most common complications associated with this procedure are small bowel obstruction (7%), wound complications (35%), and failure to restore continence (50%). The mortality rate of both procedures is less than 1%.
Alternatives
Patients with mild to moderate ulcerative colitis may be able to manage their disease with medications. Medications that are given to treat ulcerative colitis include enemas containing hydrocortisone or mesalamine; oral sulfasalazine or olsalazine; oral corticosteroids ; or cyclosporine and other drugs that affect the immune system.
A surgical alternative to ileostomy is the ileal pouch-anal anastomosis, or ileoanal anastomosis. This procedure, used more frequently than permanent ileostomy in the treatment of ulcerative colitis, is similar to a continent ileostomy in that an ileal pouch is formed. The pouch, however, is not attached to a stoma but to the anal canal. This procedure allows the patient to retain fecal continence. An ileoanal anastomosis usually requires the placement of a temporary ileostomy for two to three months to give the connected tissues time to heal.
Resources
books
"Inflammatory Bowel Diseases: Ulcerative Colitis." In The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
Pemberton, John H., and Sidney F. Phillips. "Ileostomy and Its Alternatives" (Chapter 105). In Sleisenger and Fordtran's Gastrointestinal and Liver Disease , 7th ed. Philadelphia: Elsevier Science, 2002.
Rolandelli, Rolando H., and Joel J. Roslyn. "Colon and Rectum," (Chapter 46), In Sabiston Textbook of Surgery . Philadelphia: W. B. Saunders Company, 2001.
periodicals
Allison, Stephen, and Marvin L. Corman. "Intestinal Stomas in Crohn's Disease." Surgical Clinics of North America 81, no. 1 (February 1, 2001): 185-95.
organizations
Crohn's and Colitis Foundation of America. 386 Park Ave. S., 17th Floor, New York, NY 10016. (800) 932-2423. http://www.ccfa.org .
United Ostomy Association, Inc. 19772 MacArthur Blvd., Suite 200, Irvine, CA 92612-2405. (800) 826-0826. http://www.uoa.org .
other
Hurst, Roger D. "Surgical Treatment of Ulcerative Colitis." [cited May 1, 2003]. http://www.ccfa.org/medcentral/library/surgery/ucsurg.htm .
Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Ileostomies are usually performed in a hospital operating room . The surgery may be performed by a general surgeon, a colorectal surgeon (a medical doctor who focuses on diseases of the colon, rectum, and anus), or gastrointestinal surgeon (a medical doctor who focuses on diseases of the gastrointestinal system).
QUESTIONS TO ASK THE DOCTOR
- Why is an ileostomy being recommended?
- What type of ileostomy would work best for me?
- What are the risks and complications associated with the recommended procedure?
- Are any nonsurgical treatment alternatives available?
- How soon after surgery may I resume my normal diet and activities?
Regards,
Leslie Bates
llvanbates@sbcglobal.net
January 9, 2009
i m vary to study your article
its nice work regarding to a medical reserch,
plz send me more article
problems. Also, I need suggestions on what food to eat to help my condition.
Thank you.
that the best thing in the world to use to clear it up is "Athsma-court" (inhaler). You will need a perscription from your Dr. but it is almost an instant healing. Just spray it on the very broke down skin and within a 24hr. period it will be healed.
I have had four small soft bowel movements in the past week.
Is that something I should talk to my doctor about?
Regards,
MOIN
BUT I have to agree on one thing that I am blessed with, I am not sick like I was before the surgery. So I am happy with my results from Mayo Clinic. And yes I would do it again. Good Luck
I am wondering if anyone has had this type of surgery done and what comments they would have for me to make a decision.
THE PROCEDURE IS QUIET INTERESTING AND LIFE SAVING AS WELL
Please I want to understand it and email to me the clear answer.
Thanks!!
My father recently had an Ileostomy and after 3 weeks in the hospital he was allowed to go home, under the care of my mother. While in the hospital there were many times where he did not have appetite and the protein in his blood was very low, so they fed him intravenously. After this he started eating. Just yesterday he came home he was okay and then today he did not have an appetite again. I am just hoping that he can regain his appetite. Is this normal? And how long does it really take to get into a routine life style without all the complications of surgery? By the way my dad is 71, but he worked until just a few days before his operation which was on July 12. Thank you in advance for your response to my questions.
Shahin
She also has a history of cardiac issues. She was very active in her earlier years. My question is what extra foods can help her maintain her energy levels. I recently made her a strawberry/bannana milk/ice cream smoothy. She told me her stomach did "flip flops". Does this mean she can't digest lactose? Your response is greatly appreciated.
I will have ileostomy surgery soon. This is such a horror to me that I can't contemplate life afterward. I've suffered for 22 years with Crohn's disease and there is no treatment left for me. Just the thought of having to care for a stoma makes me want to vomit. The smell, the mess, the sores and blockages. This is a normal life? Who's saying that? Is it the doctor or the patient? After reading everyone's concerns (and my heart and soul go out to every one of you) I can see that I'm going to be dealing with an unnatural, disgusting and unacceptable procedure.
I currently have a good friend with a colostomy. He is skeletal, he smells all the time, and is always having trouble with his stoma.
After reading these comments, I have decided that I'd rather live with the pain of my disease than go through this horrendous, dibilitating and undignified procedure. I just can't do this.
I've now had my ileo for only three weeks, and it's been an adjustment for sure. Yesterday, was the first day i didn't cry about it. But, as I start to feel better I can begin moving on with my life. I'm almost hurt you could call this horrendous, dibilitating, and undignified. If you think that the 750,000 Americans who currently have ostomy's are horrendous, that's truly unfortunate because surgery is not a loss. It's a way to regain a life...and not everyone has problems with blockages, odour, care etc...it's somewhat painful, but it's not as bad as the cramps I use to have!
I wish you all the best in making your decision. I hope you don't have to live sick forever because of your fear. We're doing the best we can with what's available to us. I have a temporary ileo, and will be having a second surgery to open my "J-pouch" in a few months time. I'll be able to go to the bathroom normally (rectum), but will not have the full function of a colon. So 6-8x a day, about the same as emptying your bag. Maybe this is an option for you? Then you only have to have the stoma for a few months? Talk to your surgeon team or GI for some info on this...it's quite common now :)
i need to nok as soon as possible please help
Its normal for skin irritation too. I use a stoma heasive powder on my daughter..as well as some past.. than i take the middle of the bag im cutting out to fit around the stomas and cover the skin in between and than put duo derm over that..and some more past..so not much is sticking out..it works wonders.. :) i also take off her bag from time to time and let her stomas air out :) it helps a lot.
illostomys do bleed its irritation :) its completely normal.
I am having surgery on Nov. 17,2010. I am scared because the doctor told me today that I am not only having the left colon removed but they are also stating out the right colon and the small bowel. Does anyone out there willing to go over this procedure with me and e-mail or talk to me for a couple? please e-mail me at jillpooh@comcast.net Thank you inadvance for your help. Jill Myron
And to the men out there who have ileostomys and you were that man's man(the handy man of every trade) before your surgery what have you done to keep up your spirits and return to a semi-normal quality of life, including sexually. My fiance has not attempted or even tried to initiate any type of sexual encounter. How did you get passt that?
I love my fiance and do not see him as disgusting or smelly. I have been with through all this and care for him deeply. An ileostomy is a complete change in your life but it is managable and it beats the alternative of death.
having a difficult time keeping the bag from leaking. The area is too close to his open
incision and over laps. Even the nurses are having a hard time and yet they expect me to be
able to handle this when he returns home. I am freaked out on taking care of it. He is also
coming home with a Trach as well as a g/j feeding tube. I do have a paper on what can and shouldn't be eaten by a person with an ileostomy. Mainly stay away from anything with skins unless peeled. No seeds or skins, nuts and anything that contains high fiber including most vegetables and multi grains. So in other words anything truly healthy is basically out of the question as well as high fat foods. But since my husband can't orally eat and will be on a feeding pump guess we don't need to deal with that. He is 53 and so far as lost 25 lbs Can't afford to loose anymore wasn't overweight to begin with. My biggest concern is he is constantly
elimanating and makes changing the bag difficult because it comes out so fast. And he has to have a reserve bag attached to the initial bag because it fills so quickly. How will we ever go out in public for any length of time? You can't carry around a huge folly bag? I am pretty discouraged and scared. Thx for the vent.
having a difficult time keeping the bag from leaking. The area is too close to his open
incision and over laps. Even the nurses are having a hard time and yet they expect me to be
able to handle this when he returns home. I am freaked out on taking care of it. He is also
coming home with a Trach as well as a g/j feeding tube. I do have a paper on what can and shouldn't be eaten by a person with an ileostomy. Mainly stay away from anything with skins unless peeled. No seeds or skins, nuts and anything that contains high fiber including most vegetables and multi grains. So in other words anything truly healthy is basically out of the question as well as high fat foods. But since my husband can't orally eat and will be on a feeding pump guess we don't need to deal with that. He is 53 and so far as lost 25 lbs Can't afford to loose anymore wasn't overweight to begin with. My biggest concern is he is constantly
elimanating and makes changing the bag difficult because it comes out so fast. And he has to have a reserve bag attached to the initial bag because it fills so quickly. How will we ever go out in public for any length of time? You can't carry around a huge folly bag? I am pretty discouraged and scared. Thx for the vent.
A combination of M9 drops and peppermint oil was a life saver!
There are a few things I'm worried about which I'll be very grateful if you could advice me on as you've had the ileostomy before. They are the following:
1) Odour- I'm very concerned about this issue. While wearing the bag can people smell the faeces that has filled it?? Although they say that the bags are odour proof I've read on the net within forums and blogs that smell may linger around ostmates. Please is this true? Because this is something I couldn't handle.
2) Leakage- Secondly what causes leakage? Does the bag leak itself and is this something I'll have to deal with quite often?
3) Skin irritation- What causes skin irritation? Is it the stools itself leaking? as i've heard that the bag itself may cause reaction with your skin.
4) Weight- Also since I've had UC i find it extremely difficult to put on weight as I cannot absorb food properly. I would love to gain my weight back. Having the bag does this mean that I will still have a lot of problems with weight loss? I just need to look proper healthy again.
5) Noisy wind- Another final major concern is the noise that I'll have to deal with, is it so loud that other's can hear it? Also how can i prevent this?
Sorry for bombarding any one with so many questions but as you know this operation is a major thing. Some times I just can't believe it's happening to me, my emotions these days are just ones of fright, i mean they say that taking out the colon will rid you of pain urgency etc which i hope will, but does one really and truly feel better after the op? Please help me on this one. To people with ileostomies, Would you say the op is a better way out of this constant pain?
How does the wafer stay on if you use an ointment? I've been having leakage problem lately (5x yesterday). The shape and protrusion of the stoma changed so I'm not getting a good seal. My skin is raw. I use the powder but finding it that it prevents the wafer to stick properly, and I leak. I'm so frustrated. How does the raw skin heal when you have to put the wafer over it. I wish I could air it out...So, how does the wafer stay if you use an ointment? What else do you use to keep it in place?
Thank you.
So sorry to hear about your health problems. To answer some of your questions, I'm no expert since I only have temporary ileostomy (going on 8 weeks now).
Odor: there isn't any odor if the contents are in the bag. Just make sure you clean the opening of the bag good after emptying because that could be a source of odor. The opening of the bag will get dirty, so wash with water really good. Sometimes, based on what you've eaten, it is very hard to clean thoroughly.
Leakage: this is caused by many things...folds on the skin, bad seal, change in the shape of stoma, improper size at the opening of the bag to the stoma itself, etc. The leak comes from the contents seeping through the wafer, and coming out on the side. You will know immediately if it does. It feels warm. It usually doesn't smell. Always carry a new bag with the whole precut already, paper towels, stomahesive, or anything else you use. I had problems once the shape of my stoma changed (it changes and becomes smaller), and it seems to have retracted into my body so it doesn't stick out as much. You can use a bag with convexity for this so the stoma protrudes more from your abdomen.
Skin irritation: caused by the leakage. Stool is so Irritating to the skin. The tape the surrounds the bag is sometimes irritating as well. They have powders, creams, etc.
Weight: you will lose weight. It just happens. No matter how much I ate, I can't seem to gain weight.
Good luck. Hope this info helps...:)
I got my ileostomy at the age of 16 in 1998.
Feel free to e-mail me to discuss my experiences if you like.
Carynkeppler@gmail.com
Does anyone have anything that will actually heal the burn around my stoma. I am currently sitting with my stoma over a trash can and wiping the drainage with paper towels. HELP!
THANK YOU
please help me and my aunt. i need information on loop ileostomy. is it really normal for food to leave her body 5 minutes after eating? or did they make a mistake somewhere. i cant help but feel something is wrong. please help!!
Make it a Great Day!
Diana
make this happen?Do they reenter through the stomach? What surg.cuts do they do?Please mail to
email address.Thankyou .
to be changed?
Thank you.
Cathy
Personally, the ileostomy is a hell for me - yes I survived cancer, which I am eternally grateful, but the battle of weight loss, outputting on average 5 litres of waste a day, always feeling dehydrated, weak and tired, really gets you down.
The first couple of weeks after getting home, I had trouble keeping the skin around the area free from sores and redness, but the use of a skin barrier cream around the area of the ileostomy has helped no end. Still can't get use to the smell when I take the wafer off though.
I'm due for a reversal on 17 Jan. I know, that can have it's own complications and I may be jumping from the frying pan straight into the fire...but I can't wait. I honestly feel, that any longer, the ileostomy would have a major detrimental impact on my health as it stands at the moment.
My greatest advice is, try to keep hydrated. Through all this I have realised just how important hydration is to maintain health.
1. Always use Flexwear Wafers, they hold better & more comfortable. He uses the two piece drainable kind so we don't have to change bags every time he has a bowel movement. 2 piece drainable kind lasts 5 days usually, best if changed every 4 days.
2. Take hot shower to help loosen up the wafer from the skin when ready to change. Pick a time when you don't have bowel movements, if possible. Hubby prefers doing it in the mornings. Your skin would LOVE to aired out so if you can, just give your skin a few minutes to air before putting new bag on!
3. Use Cavilon No Sting Barrier spray or wipes. Spray works better. After shower, dry skin, spray Cavilon everywhere the wafer goes & especially right around the stoma, then fan it dry. Reapply the spray for double protection, fan dry.
4. Make sure you warm up the wafer with your hands before you remove the plastic & apply the paste. After applying the wafer to your skin, make sure you warm the wafer for at least 45 seconds to 1 minute with your hands, all the way around the wafer. This helps it stick better! Most forget to do this & has leakage problems.
5. We put Stomahesive Protective Powder right around the stoma after the wafer is applied to help keep it from getting infection. Then place the bag on the wafer and you're done!
6.. When you drain your bag, take a small glass of water & pour into bag from the drainable end to help clean the bag out. Hubby actually leans back a little to help clean the bag even better.He keeps a bottle of water with him wherever he goes so he can do this anywhere.
7. Keep an emergency bag kit, complete with wafer, bag, paste, spray, etc. ready to go in case you have to leave in a hurry to go somewhere.
8. Have your doctor keep track of your B12 level thru blood work. All Ileostomy patients will eventually lack B12 & have complications from it eventually. Hubby takes a multi-vitamin with B12 & will be getting B12 shots from his doctor starting next week. Best to take the liquid B12 or crush up the pill vitamins because the colon's gone & can't absorb the vitamin. Hubby was feeling drained, tired, no energy & it was all due to the B12 level being too low.
9. Drink LOTS of water!
10. If odor in the bag is too much, you can always add 2-3 drops of the Ostomy Appliance Deodorant to the bag & it really works!
Also, has anyone had an appliance problem (failure) caused by taking antibiotics?
Is anyone allergic to adhesive, and if so, what kind of, or brand of appliance do you use?
Has anyone had trouble with health insurance reimbursements from Medicare?
Thanks.
kate
In Oct 6, 2010 you wrote about your mum having trouble regulating her magnesium levels following an ileostomy. This sounds exactly like what my Dad is going through at the moment. What was the outcome for your Mum, were they able to regulate it. Any help/advice would be welcome. Hope everything is now going well for you both. Thanks A.
The chest pain appears after eating, especially if I lie down too soon. I struggle to drain the stoma by putting pressure on my abdomen in an effort to feel better. My mouth is dry at night, even after drinking a whole glass of water. I have HBP an CKD stage 3 at 68 years old. Very fatigued. And to complicate the issue I have the Hep C antibody probably from the transfusion I had after surgery at that early time(1980), I was told I have a negative PCR for the hep c virus. Also have diabetes for about twenty years, now on novalog 70/30 and fearful of gaining weight. Extreme fatigue and stomach distention also.
I feel that my chest pain and related back pain is due to delayed emptying, or some kind of obstruction causing the fundus of my stomach to push against my heart. Tried grape juice, and now prune juice. Is there another surgery that can help me? I feel like death warmed over.
One more thing IF you have UC and are considering surgery I believe that in 1970 by serendipity I caused my own remission by demanding a painkiller in the hospital while on hyperalimentation prednisone and azulphidine ( at that time the only meds used). They sent me a psychiatrist who unbeknown to me gave me haldol, my pain STOPPED and my UC exacerbation went away to the amazemement of my doctors. I did not connect the Haldol to the remission until after an emergency ileostomy for UC ten years later because I eventually went off the prednisone which was making me crazy. I remember I was on Haldol for only ten days and it worked. Doctors look at me as if I am crazy or smile condesendingly when I tell the story. I knew the stigma of Haldol and was actually insulted at the time (doctors warned a pain killer could cause paralytic ileus and toxic megacolon, however as I only took it for about eight days back in 1970 I had NO side effects, no withdrawal. Today I would gladly eat a plateful of Haldol, Thorazine or whatever it takes to avoid this surgery that has ruined my life physically and mentally. I suggest you bypass your gastro, or go comcomitantly to a shrink of your choosing for a short regimen of Haldol (skip the other drugs given to bi-polars) just to see if it helps quiet the bowel. Your gastro guy does not have to know you are trying this. Haldol if used for a short regimen is less toxic than the steroid prednisone with the side effect of making you moon faced and irritable. I wish some doctors would consider before suggesting surgery to try this anti-pychotic, only available to pychiatrists.
There is one thing that is happening that I do not beleive as normal at all and cannot find anything on it. I am having large amounts of very bad smelling, red fluid coming out of the vaginal area. Can anyone tell me if they have had this before?
Thank you to anyone who may have some insight.
A couple of things: consider yeast, in which case you need Mycostatin powder. It can be tough to get; make friends with a pharmacist or wound nurse. Powder goes right on the sores, with the twin benefit of treating the yeast and drying the skin.
Best I have found though is Betaderm cream for any area not covered by the appliance. Under the appliance you need Betaderm liquid. Use it when you change. Apply liquid generously to sores, allow to air dry and then put appliance in place. Betaderm is normally a scalp treatment so you have to insist with doctor. You need a prescription. Do not discount the value of a dermatologist.
my mother has a illistomy and is in alot of pain has had 31 surgeries in 41 years and only aboaut now 10 inches left of the small intestine.. thats it and im very worried she had her stoma dilated and they cant find anything when he stuck his finger in to feel and it was scar tissue but he broke it up and he has done alot of the surgeries on my mother. the problem she had another cat scan to see if he missed anything and cant find anything no hernia and she is in worse pain then before she is to go to grand rapids hospital to a group of dr's at ferguson hospital but found out her insurance company wont cover that dr. they are not accepting her insurance. im so concerned the first sergion wanted to do a scope but now told her it is too risky now we are all very concerned.. dont know what or where to turn now... she is in alot of pain and she never complaines over all these years and so now when she tells me she is in alot of pain i know she is... pain killers helping only for short times, she states its like a knife jabbing in side and i see her face twinge and she tries to not show it killing her.. but she is getting worn out. i try searching on line nothigin i foudn this site.. i am lost
sara beth
Another secret is my back up pouch security. For the curved Hollister clip with the hook (a favorite) I found that I can secure it like fort knox with a simple O ring (one cm in diameter) that you can find in a specialty hardware. For the Velcro closure I found a simple metal paper bonding clip (the kind with the wire handles used to bind folders), I get an assortment at the dollar store and use the smallest binder clip to give extra security to the Velcro, whether its the lock and roll variety, or whatever. It works! I use the larger diameter holister convex appliance to give my skin a break at home but I find the larger diameter of the faceplate makes it too easy to pull off, or fall off if I am having trouble draining it.
I am not happy with the extreme belly distension and the pressures I feel even when lying down with my new stoma, and I still have a sticking pain (like an open cut) at the site of my old stoma. I also can no longer massage and push my intestine to drain out what is left, or even to get it to move, it has its own mind. I also suffer from total body itching and depression. Does anyone else have this problem?
with leakage and damaged skin. Is it possible for the stoma to be corrected? Thank you.
Having an ostomy is not fun, but it is more of an occasional inconvenience than anything. You can do this!
Thanks
I had occassion of stool blockage in last 3 months 3-4 occassion and probably it is due to fibre/leafy food.Took assistance from hospital.subjected to abdomen x ray/sonography.. both are ok...
My overall health is ok, but i am scared to travel long distance / afraid to take any job assignment. I am 65 years , well expereinced oil and gas operation/commissioning person.
Please suggest me how to handle this pouch system in better way? Is there any case where small intestine again join to rectum canal or transplant of rectum and j pouch to get rid of external pouch? is any one know such case?
my wishes to all who are facing problems alike and also to all those having better life and inspire us and give hope to improve our life... thanks
is this a normal issue or did the first surgery go bad and they went again to cover up a mistake...
Also, a trick to make the bag stick, I use my blow dryer's heat around the stoma. Once it is place I heat it again then I fold a pillow and lay flat for a few minutes. If I see a bubble or crimp I place a small round bandaid 1/2 way on the bag and 1/2 on my skin. I also use a moldable ring, which is similar to putty, and it lifts the bag away from my skin.
After reading your posts I am terrified about my ileostomy. I have a couple of questions maybe someone can answer. Has anyone had their rectum removed at the same time? If so, how did that go? Did anyone have drainage tubes? Do you have significant weight loss? How long was your recovery? Were you able to go home following your stay in the hospital and how long was your stay? I am 69 and live alone and am hoping I will be able to return home after I leave the hospital.
God Bless each of you as you continue with your journey. Here's a prayer hoping you can find some relief and peace. My ostomy supplier has been Edgepark who provides Colaplast products. They did everything within their means to accommodate me following my colostomy and I feel comfortable they will do the same with my ileostomy if I decide to move forward.
I have some concerns about weight gain since I've recovered from my Illieostomy surgeries. I under went 3 of these surgeries because after my closures my intestines kept rupturing open again. Now I only have 50% of my intestines and now I cannot stop gaining weight. Due to numerous surgeries for this situation my abdomen always hurts and I cannot handle doing any strenuous activity such as, cleaning the house, going up & down the steps to do laundry, long walks, lifting more than 10 -12 pounds, exercising. Standing on my feet of more than 30 minutes. I've also had numerous other abdomen surgeries before these for serve endometriosis. What can I do to loose weight? Please help me.