Enucleation, eye
Definition
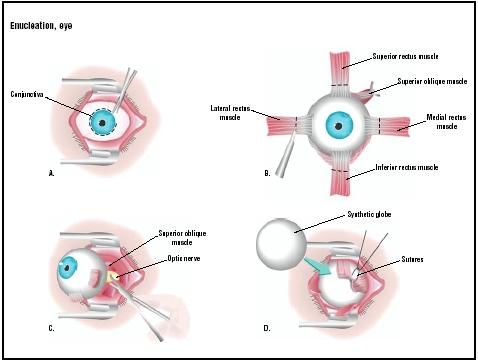
Enucleation is the surgical removal of the eyeball that leaves the eye muscles and remaining orbital contents intact.
Purpose
Enucleation is performed to remove large-sized eye tumors or as a result of traumatic injury when the eye cannot be preserved. In the case of tumors, the amount of radiation required to destroy a tumor of the eye may be too intense for the eye to bear. Within months to years, many patients who are treated with radiation for large ocular melanomas lose vision, develop glaucoma, and eventually have to undergo enucleation.
The two types of eye tumors that may require enucleation are:
- Intraocular eye melanoma. This is a rare form of cancer in which malignant cells are found in the part of the eye called the uvea, which contains cells called melanocytes that house pigments. When the melanocytes become cancerous, the cancer is called a melanoma. If the tumor reaches the iris and begins to grow, or if there are symptoms, enucleation may be indicated.
- Retinoblastoma. Retinoblastoma is a malignant tumor of the retina. The retina is the thin layer of tissue that lines the back of the eye; it senses light and forms images. If the cancer occurs in one eye, treatment may consist of enucleation for large tumors when there is no expectation that useful vision can be preserved. If there is cancer in both eyes, treatment may involve enucleation of the eye with the larger tumor, and radiation therapy for the other eye.
Demographics
Data from the U.S. National Center for Health Statistics estimate that nearly 2.4 million eye injuries occur in the United States annually. This report calculated that nearly one million Americans have permanent significant visual impairment due to injury, with more than 75% of these individuals being blind in one eye. Eye injury is a leading cause of monocular blindness in the United States, and is second only to cataract as the most common cause of visual impairment. While no segment of the population escapes the risk of eye injury, the victims are more likely to be young. The majority of all eye injuries occur in persons under thirty years of age. Trauma is considered the most common cause of enucleation in children over three years of age.
For the year 2000, Texas demographics for cancer of the eye and orbit were fewer than five per 100,000. According to the Nilt, there are about 2,200 cases of eye cancer diagnosed in the United States each year.
Description
Following anesthesia, the surgeon measures the dimensions of the eye globe, length of the optic nerve, and horizontal dimensions of the cornea. The surgeon then illuminates the globe of the eye before opening it. A dissecting microscope is used to detect major features and possible minute lesions. The eye is opened with a sharp razor blade by holding the globe with the left hand, cornea down against the cutting block, and holding the blade between the thumb and middle finger of the right hand. Enucleation proceeds with a sawing motion from back to front. The plane of section begins adjacent to the optic nerve and ends at the periphery of the cornea. The plane of section is dependent on whether a lesion has been detected. If not, the globe is cut along a horizontal plane, using as surface landmarks the superior and inferior oblique insertions and the long postciliary vein. If a lesion has been found, the plane of section is modified so that the lesion is included in the slab.
Diagnosis/Preparation
Enucleation may be performed under general or local anesthesia. In either case, the injection is given in the retrobulbar space. An antibiotic and an anti-inflammatory medication such as dexamethasone are also given intravenously.
Aftercare
Because the eye is surrounded by bones, it is much easier for patients to tolerate enucleation than the loss of a lung or kidney. When surgery is performed under general anesthesia, patients do not feel or see anything until they regain consciousness. Additional local anesthesia is often given at the end of the surgery so that the patient will have the least pain possible when waking up in the recovery room . Most patients have a headache for 24–36 hours after surgery that is relieved with two regular headache medication pills, such as Tylenol, every four hours. A firm pressure dressing is maintained for four to six days, such oral antibiotics are given for one week; and steroids, as prednisone, adjusted according to patient status, are given three times daily for four days. The socket is evaluated after removal of the pressure dressing. If the edema has disappeared, the sutures are removed. Topical antibiotics are applied four times daily for four weeks.
Risks
Enucleation surgery is very safe; only rarely do patients experience major complications. Complications include the following: bleeding, infection, scarring, persistent swelling, pain, wound separation, and the need for additional surgery. Complications may also occur with the orbital implants routinely used with patients who have undergone enucleation. Among these is the risk of infection.
Normal results
Within two to six weeks of enucleation surgery, patients are sent for a temporary ocular prosthesis (plastic eye). Besides the swelling and the black eye, patient features look normal. After a final prosthetic fitting, 90% of patients are usually quite happy with the way they look; 80% say others cannot even tell that they have only one eye.
Morbidity and mortality rates
In a study performed by the National Eye Institute on melanoma patients, at five-year follow-up, 82% of the patients who underwent enucleation remained alive. At a 10-year follow-up, 31% remained alive. As of 2003, the study is still ongoing and will follow all patients for up to 15 years.
Alternatives
There are no alternatives to enucleation because it is a procedure of last resort performed when other treatments have failed.
Resources
books
Linberg, J. W. Oculoplastic and Orbital Emergencies. New York: McGraw-Hill Professional, 1992.
Shields, J. A., and C. L. Shields. Atlas of Orbital Tumors. Philadelphia: Lippincott Williams & Wilkins, 1999.
Tasman, W., et al. The Wills Eye Hospital Atlas of Clinical Ophthalmology. Philadelphia: Lippincott Williams & Wilkins, 2001.
Vafidis, G. et al. Perioperative Care of the Eye Patient. Annapolis Junction, MD: BMJ Books, 2000.
periodicals
Adenis, J. P., P. Y. Robert, and M. P. Boncoeur-Martel. "Abnormalities of orbital volume." European Journal of Ophthalmology 12 (September-October 2002): 345–350.
Burroughs, J. R., C. N. Soparkar, J. R. Patrinely, et al. "Monitored anesthesia care for enucleations and eviscerations." Ophthalmology 110 (February 2003): 311–313.
Chantada, G., A. Fandino, S. Casak, et al. "Treatment of overt extraocular retinoblastoma." Medical Pediatric Oncology 40 (March 2003): 158–161.
Gragoudas, E., W. Li, M. Goitein, et al. "Evidence-based estimates of outcome in patients irradiated for intraocular melanoma." Archives of Ophthalmology 120 (December 2002): 1665–1671.
Jordan, D. R., S. R. Klapper, and S. M. Gilberg. "The use of vicryl mesh in 200 porous orbital implants: a technique with few exposures." Ophthalmologic and Plastic Reconstruction Surgery 19 (January 2003): 53–61.
organizations
American Academy of Ophthalmology. P.O. Box 7424, San Francisco, CA 94120-7424. (415) 561-8500. http://www.aao.org/index.html .
American College of Eye Surgeons. 2665 Oak Ridge Court, Suite A, Fort Myers, FL 33901. (239) 275-8881. http://www.aces-abes.org/ .
National Cancer Institute. Suite 3036A, 6116 Executive Boulevard, MSC8322, Bethesda, MD 20892-8322.(800) 422-6237. http://cancer.gov/ .
other
Finger, Paul T., MD, FACS. "Enucleation." Eye Cancer Network. [cited May 5, 2003]. http://www.eyecancer.com/Enucleation/enuc.html .
Monique Laberge, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Eye enucleation is usually performed by an ophthalmic surgeon or an ophthalmologist in a hospital setting. Young and healthy patients may undergo the surgery on an outpatient basis but most stay in the hospital for at least one night after surgery. Ophthalmic surgeons are members of the American College of Eye Surgeons, and are certified by the American Board of Eye Surgery after submitting to an extensive written application. Before ABES certification, they must be certified by the American Board of Ophthalmology (ABO). This certification indicates successful completion of an approved residency program and acquisition of sufficient knowledge in the areas of medical and surgical ophthalmology.
QUESTIONS TO ASK THE DOCTOR
- Why is enucleation required?
- Will there be pain after surgery?
- How many enucleations do you perform in a year?
- How much time will I need to recover from the operation?
- When can I get a prosthesis?
This article had good information and answered most of the questions that were in my mind. Thank you.
Debbie Cummings
Thanks, Deborah
I am 25 now and now scared that the doctors who have held my hand the whole time will age before me. What happens then? And is this a normal fear? Or is it even a fear worth acknowledging?
Thanks and Regards.
Debashis Mondal
Today, I am seeing a plastic ophthalmologist. The eye needs to be removed. My understanding is that during surgery, cadaver sclera will be implanted into my head, an artificial prosthesis will be placed in the eye, and the conjunctiva will be used to cover the eye. When I open my eye, I will see gunk and pink.
I have already suffered, as we all have, the tortures of the damned. My question is this: How long is the recovery? I am still working full-time and only have 17 sick days left. Please be as honest as possible and let me know how long you were out of work. Many thanks.
Thanks. James
more prevalent in different light. When I shut my right eyelids tightly, the "haze" disappears. My brain is trying to get signals from my right eye and reacts to the right eyelids being closed.
Anyone else have this challenge?
I also have had sinus issues on the right side - from low grade, long term infections to pressure when the barometer changes (I can predict snow and rain :)!!!). I have had some crania-sacral sessions which relieved some of these issues; I also am starting to do nasal washes. Hoping to keep sinuses clear and improve breathing on right side while reducing/eliminating the almost constant drainage and throat clearing. Anyone else have this challenge?
Blessed to be alive!
The drainage should stop after a while. Ask your ocularist. If there are air pockets in the socket, they can fill up with fluid. They should be able to fill these in. But also, just having a foreign object in the eye can cause the mucous glands to react. Once the conjunctiva has completely grown over the implant (which can take 3 - 6 mons, from what I've heard), this should reduce the mucous production.
I'm 11 weeks post-op enucleation and should have my prosthetic eye by the end of next week. I had a derma-fat graft and currently have constant drainage - a combo of mucous and bloody-tinged fluid. I'll be happy when this subsides!
Why is this still happening?
This article is great it has given me loads off information.
My surgeon was brilliant and I have suffered no pain or bruising and I have no regrets about choosing enucleation. I am looking forward to my temporary prosthetic eye in 5 weeks time.
My nephew just had his left eye removed yesterday... due to pain and pressure also there was a retinal detachment and he's been legally blind almost since birth. As soon as we left the hospital he complained of great pressure and still feeling lots of pain. I figured that's normal because the anesthesia is wearing off. This morning he is still in lots of pain but now also says that he is seeing really blurry from the right eye (his good eye) and I'm kinda scared and don't know what to do... but calm him down and wait it out a few more days
How long did it take to recover? were you able to return to work right after since I've read that it is an outpatient surgery or will possibly spend either 1 night in the hospital.
how would you rate the pain 10 being the worst pain & 1 being not as painful . any information would be greatly appreciated thank you
The view is a black background with a shiny flickering surface.it makes me dizzy at times
Has anyone else experienced this.