Dermabrasion
Definition
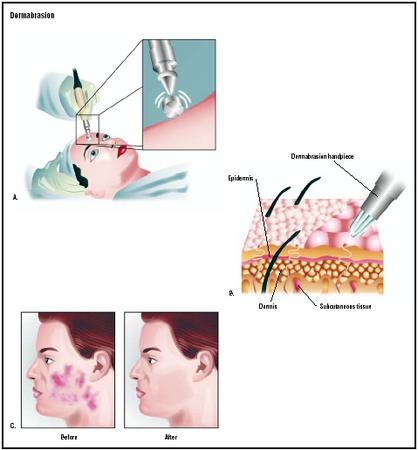
Dermabrasion is a procedure to improve the look of the skin involving the mechanical removal of the damaged top layer using a high speed rotary wheel.
Purpose
Originally developed as a means of treating acne scars, dermabrasion can be used to treat many kinds of skin problems including scars from other types of wounds, wrinkles, skin coloration abnormalities, and other more serious conditions such as rhinophyma, a disfiguring form of rosacea that affects the nose. Although the treatment is not a cure, in that the scar or other abnormality cannot be entirely removed, dermabrasion does soften the edges of the scar or other abnormality and can radically improve its appearance.
Dermabrasion is often used in combination with other plastic surgery techniques, such as chemical peels, excisions, punch grafting, and CO 2 laser resurfacing to achieve an overall smoothing of various skin abnormalities, particularly of the face.
Demographics
Dermabrasion is a technique that has been used in dermatology for over 100 years. Although used much less often since the advent of laser resurfacing, dermabrasion continues to be a viable treatment that has been reported to have quicker healing times, similar rates of complications, and is more effective in eliminating some types of lesions, particularly surgical scars. According to the American Society for Aesthetic Plastic Surgery, there were about 60,000 dermabrasion procedures performed in 2001.
Description
Dermabrasion is commonly performed using a handheld engine that can reach rotational speeds of 18,000–35,000 rpm. Rapid planing of the skin is achieved through the combination of this rotational speed, the abrading attachment, and pressure applied by the operator. Because of the importance of the skill of the operator, patients should select doctors with significant experience with the procedure.
There are three types of abrading attachments in common use: diamond fraises, wire brushes, and serrated wheels. Diamond fraises are stainless steel wheels that have diamond chips of various coarseness bonded
Before the procedure begins, medication is often given to relax the patient and reduce pain. For small areas, local anaesthetic nerve blocks are often used to numb the area being treated. Alternatively, topical cryoanaesthesia (numbing the skin using cold) can be used. This is done by spraying a cold-inducing agent on the skin. Sometimes the skin is pre-chilled with ice to increase the anaesthetic effect.
During the procedure the patient lies on his back on the surgical table, eyes covered with disposable eye patches. The area being treated is parted with Gentaian violet, a stain that will help gauge how deep the treatment is going. A gloved and gowned assistant holds the skin taut while each section of the face is abraded using the hand-held engine. The surgeon works in sections to avoid obvious lines of demarcation in the final results. If the entire face is to be dermabraded, laser is commonly used for the lower eyelids and lip as less than satisfactory results often occur in these areas.
Diagnosis/Preparation
Because there are several different skin surfacing techniques now available, the initial meetings with the dermatological or plastic surgeon must ensure that dermabrasion is the technique of choice for the particular skin abnormality and location that is being treated. Although controversial, some studies have reported abnormal scarring in patients previously treated with 13 cisretinoic acid (Accutane), so many surgeons will require a six month break from the medication before performing dermabrasion. A second contraindication for dermabrasion is HIV or hepatitis infection, as small droplets of blood becomes aerosolized (distributed within the air) during the treatment, creating a risk for the doctor and other staff.
Finally, even if there is no patient history of cold sores, it is important that anti-viral medicine is administered to anyone undergoing the procedure, as an outbreak after dermabrasion can be very severe and spread beyond the mouth to other areas of the face.
Aftercare
After the procedure, any treated areas are dressed for healing. For example, a dressing that is primarily water held on a mesh support, called Vigilon, can be used to cover the wound. It is changed daily for about five days, then the wound is left open to the air. This kind of treatment speeds the restoration of the epithelium, the cellular covering of the body. Using this technique, healing occurs in about five to seven days.
Generally, the patient is given pain medication, antibiotics , and anti-swelling medication during recovery. Antiviral drugs are also continued. Patients should avoid the sun during the healing process.
Risks
The most common complication of the procedure is the formation of keloid, a type of abnormal scar that results from excessive collagen production. Because this type of scarring tends to be associated with darker skin types, patients with this kind of skin should approach dermabrasion with caution. Other potential complications include abnormal pigmentation of the treated skin, persistent redness of the skin, and a localized dilation of small groups of blood vessels called telangiectasia. Finally, the formation of milia, bumps that form due to obstruction of the sweat glands, although this can be treated after healing with retinoic acid.
Normal results
Normal results include significant improvement in the appearance of the skin's surface after healing of the skin. It should be emphasized, however, that many scars will not be completely removed and the change in appearance is to due a softening of the edges of the abnormality, not elimination. If a patient cannot tolerate a residual presence of the scar or other abnormality, the treatment should not be used.
Morbidity and mortality rates
The morbidity and mortality rate of this cosmetic procedure is extremely low.
Alternatives
A variety of other skin resurfacing techniques are available and include chemical (phenol or trichloroacetic acid, TCA) peels and laser (CO 2 and Erbium) resurfacing.
See also Laser skin resurfacing .
Resources
books
Stuzin, James M., Thomas J. Baker, and Tracy M. Baker. "Treatment of Photoaging: Facial Chemical Peeling." In Plastic Surgery: Indications, Operations, and Outcomes. Vol. 5, edited by Craig A. Vander Kolk, et al. St. Louis: Mosby, 2000.
periodicals
Roenigk, Henry H. "Dermabrasion: State of the Art 2002." Journal of Cosmetic Dermatology 1 (2002): 72–87.
organizations
American Society for Aesthetic Plastic Surgery, 11081 Winners Circle, Los Alamitos, CA 90720. (800) 364-2147 or (562) 799-2356. http://www.surgery.org
American Society of Plastic Surgeons. 444 E. Algonquin Rd. Arlington Heights, IL 60005. (800) 475-2784. http://www.plasticsurgery.org
Michelle Johnson, M.S., J.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
This procedure should be performed by a dermatological or plastic surgeon with experience in dermabrasion. It is done in an outpatient suite. Hospitalization is not required.
QUESTIONS TO ASK THE DOCTOR
- What characteristics of my skin abnormality suggest using dermabrasion to treat it?
- Would laser or chemical treatments be an option?
- What is the expected cosmetic outcome for the treatment in my case?