Scleral buckling
Definition
Scleral buckling is a surgical procedure in which a piece of silicone plastic or sponge is sewn onto the sclera at the site of a retinal tear to push the sclera toward the retinal tear. The buckle holds the retina against the sclera until scarring seals the tear. It also prevents fluid leakage which could cause further retinal detachment.
Purpose
Scleral buckling is used to reattach the retina if the break is very large or if the tear is in one location. It is also used to seal breaks in the retina.
Demographics
Retinal detachment occurs in 25,000 Americans each year. Patients suffering from retinal detachments are commonly nearsighted, have had eye surgery, experienced ocular trauma, or have a family history of retinal detachments. Retinal detachments also are common after cataract removal. White males are at a greater risk, as are people who are middle-aged or older. Patients who already have had a retinal detachment also have a greater chance for another detachment.
Some conditions, such as diabetes or Coats' disease in children, make people more susceptible to retinal detachments.
Description
Scleral buckling is performed in an operating room under general or local anesthetic. Immediately before the procedure, patients are given eye drops to dilate the pupil to allow better access to the eye. The patient is given a local anesthetic. After the eye is numbed, the surgeon cuts the eye membrane, exposing the sclera. If bleeding or inflammation blocks the surgeon's view of the retinal detachment or hole, he or she may perform a vitrectomy before scleral buckling.
Vitrectomy is necessary only in cases in which the surgeon's view of the damage is hindered. The surgeon makes two incisions into the sclera, one for a light probe and the other for instruments to cut and aspirate. The surgeon uses a tiny, guillotine-like device to remove the vitreous, which he then replaces with saline. After the removal, the surgeon may inject air or gas to hold the retina in place.
After, the surgeon is able to see the retina, he or she will perform one of two companion procedures.
-
Laser photocoagulation. The laser is used when the retinal tear is small
or the detachment is slight. The surgeon points the laser beam through a
contact lens to
burn the area around the retinal tear. The laser creates scar tissue that will seal the hole and prevent leakage. It requires no incision.
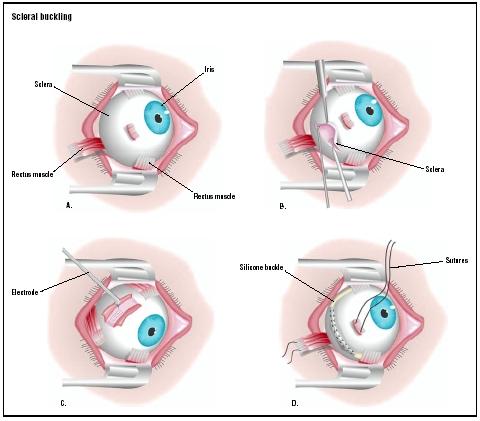 In a scleral buckling procedure, one of the eye's rectus muscles are severed to gain access to the sclera (A). The sclera is cut open (B), and an electrode is applied to the area of retinal detachment (C). A silicone buckle is threaded into place beneath the rectus muscles (D), and the severed muscle is repaired. (Illustration by GGS Inc.)
In a scleral buckling procedure, one of the eye's rectus muscles are severed to gain access to the sclera (A). The sclera is cut open (B), and an electrode is applied to the area of retinal detachment (C). A silicone buckle is threaded into place beneath the rectus muscles (D), and the severed muscle is repaired. (Illustration by GGS Inc.) - Cryopexy. Using a freezing probe, the surgeon freezes the outer surface of the eye over the tear or detachment. The inflammation caused by the freezing leads to scar formation that seals the hole and prevents leakage. Cryopexy is used for larger holes or detachments, and for areas that may be hard to reach with a laser.
After the surgeon has performed laser photocoagulation or cryopexy, he or she indents the affected area of the sclera with silicone. The silicone, either in the form of a sponge or buckle, closes the tear and reduces the eyeball's circumference. This reduction prevents further pulling and separation of the vitreous. Depending on the severity of the detachment or hole, a buckle may be placed around the entire eyeball.
When the buckle is in place, the surgeon may drain subretinal fluid that might interfere with the retina's reattachment. After the fluid is drained, the surgeon will suture the buckle into place and then cover it with the conjunctiva. The surgeon then inserts an antibiotic (drops or ointment) into the affected eye and patches it.
For less severe detachments, the surgeon may choose a temporary buckle that will be removed later. Usually, however, the buckle remains in place for the patient's lifetime. It does not interfere with vision. Scleral buckles in infants, however, will need to be removed as the eyeball grows.
Diagnosis/Preparation
Retinal detachment is considered an emergency situation. In the case of an acute onset detachment, the longer it takes to repair the detachment, the less chance of successful reattachment. Usually the patient sees floating spots and experiences peripheral visual field loss. Patients commonly describe the vision loss as having someone pull a shade over their eyes. In extreme cases, patients may lose vision completely.
An ophthalmologist or optometrist will take a complete medical history, including family history of retinal detachment and any recent ocular trauma. In addition to performing a general eye exam, which includes a slit lamp examination, examination of the macula and lens evaluation, physicians may perform the following tests to determine the extent of retinal detachment:
- echography
- 3-mirror contact lens/panfunduscopic
- scleral indentation
Small breaks in the retina will not require surgery, but patients with acute onset detachment require reattachment in 24–48 hours. Chronic retinal detachments should be repaired within one week.
Because scleral buckling is usually an emergency procedure, there is no long-term preparation. Patients are required to fast for at least six hours before surgery.
Aftercare
Immediately following the surgery, patients will need help with meals and walking. Some patients must remain hospitalized for several days. Many scleral buckling procedures however are performed on an outpatient basis.
After release from the hospital, patients should avoid heavy lifting or strenuous exercise that could increase intraocular pressure. Rapid eye movements should also be avoided; reading may be prohibited until the surgeon gives permission. Sunglasses should be worn during the day and an eye patch at night. Pain and a scratchy sensation as well as redness in the eye also may occur after surgery. Ice packs may be applied if the conjunctiva swells. Patients may take pain medication, but should check with their physician before taking any over-the-counter medication.
Excessive pain, swelling, bleeding, discharge from the eye or decreased vision is not normal, and should immediately be reported to the physician.
If a vitrectomy was performed in conjunction with the scleral buckling, patients must sleep with their heads elevated. They also must avoid air travel until the air bubble is absorbed.
After scleral buckling, patients will use dilating, antibiotic or corticosteroid eye drops for up to six weeks to decrease inflammation and the chance of infection. Best visual acuity cannot be determined for at least six to eight weeks after surgery. Driving may be prohibited or restricted while vision stabilizes. At the six-to-eight week postoperative visit, physicians determine if the patient needs corrective lenses or stronger prescription lenses. Full vision restoration depends on the location and severity of the detachment.
Risks
Complications are rare but may be severe. In some instances, patients lose sight in the affected eye or lose the entire eye.
Scar tissue, even pre-existing scar tissue, may interfere with the retina's reattachment and the scleral buckling procedure may have to be repeated. Scarring, along with infection, is the most common complication.
Other possible but infrequent complications include:
- bleeding under the retina
- cataract formation
- double vision
- glaucoma
- vitreous hemorrhage
Patients may also become more nearsighted after the procedure. In some instances, although the retina reattaches, vision is not restored.
Normal results
The National Institutes of Health reports that scleral buckling has a success rate of 85–90%. Restored vision depends largely on the location and extent of the detachment, and the length of time before the detachment was repaired. Patients with a peripheral detachment have a quicker recovery then those patients whose detachment was located in the macula. The longer the patient waits to have the detachment repaired, the worse the prognosis.
Morbidity and mortality rates
The danger of mortality and loss of vision depends on the cause of the retinal detachment. Patients with Marfan syndrome, pre-eclampsia and diabetes, for example, are more at risk during the scleral buckling procedure than a patient in relatively good health. The risk of surgery also rises with the use of general anesthesia. Scleral buckling, however, is considered a safe, successful procedure.
Severe infections that are left untreated can cause vision loss, but following the prescribed regimen of eye drops and follow-up treatment by the physician greatly minimizes this risk.
Alternatives
Vitrectomy is sometimes performed alone to treat retinal detachments. Laser photocoagulation and cryopexy also may be used to treat less serious tears. The more common alternative, however, is pneumatic retinopexy, which is used when the tear is located in the upper portion of the eye. The surgeon uses cryopexy to freeze the area around the tear, then removes a small amount of fluid. When the fluid is drained and the eye softened, the surgeon injects a gas bubble into the vitreous cavity. As the gas bubble expands, it seals the retinal tear by pushing the retina against the choroid. Eventually, the bubble will be absorbed.
The patient is required to remain in a certain position for at least a few days after surgery while the bubble helps seal the hole. Pneumatic retinopexy also is not as successful as scleral buckling. Complications include recurrent retinal detachments and the chance of gas getting under the retina.
Resources
books
Buettner, Helmut, M.D., editor. Mayo Clinic on Vision and Eye Health. Rochester, MN: Mayo Clinic Health Information, 2002.
Cassel, Gary H., M.D., Michael D., Billig, O.D., and Harry G. Randall, M.D. The Eye Book: A Complete Guide to Eye Disorders and Health. Baltimore, MD: Johns Hopkins University Press, 1998.
Everything You Need to Know About Medical Treatments , edited by Stephen Daly. Springhouse, PA: Springhouse Corp., 1996.
Sardgena, Jill, et al. The Encyclopedia of Blindness and Vision Impairment, 2nd Edition. New York, NY: Facts on File, Inc. 2002.
organizations
American Academy of Ophthalmology. PO Box 7424, San Francisco, CA 94120-7424. (415) 561-8500. http://www.aao.org .
American Board of Ophthalmology. 111 Presidential Boulevard, Suite 241, Bala Cynwyd, PA 19004-1075. (610) 664-1175. info@abop.org. http://www.abop.org .
National Eye Institute. 2020 Vision Place, Bethesda, MD 20892-3655. (301) 496-5248. http://www.nei.nih.gov .
other
Handbook of Ocular Disease Management: Retinal Detachment Review of Ophthalmology [cited April 21, 2003]. http://www.revoptom.com/handbook/SECT5R.HTM .
"Retinal Detachment." VisionChannel.net [cited April 12, 2003]. http://www.visionchannel.net/retinaldetachment/treatment.shtml .
"Retinal Detachment Repair." EyeMdLink.com [cited May 1, 2003]. http://www.eyemdlink.com/EyeProcedure.asp?EyeProcedureID=52 .
Wu, Lihteh, M.D. "Retinal Detachment, Exudative." emedicine.com . June 28, 2001 [cited May 1, 2003]. http://www.emedicine.com/oph/topic407htm .
Mary Bekker
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Scleral buckling can be performed by a general ophthalmologist, an M.D. who specializes in treatment of the eye. Even more specialized ophthalmologists, vitreo-retinal surgeons who specialize in diseases of the retina, may be called upon for serious cases.
The surgery is usually performed in hospital settings. Because of the delicacy of the procedure, sometimes an overnight hospital stay is required. Less severe retinal detachments can be treated on an outpatient basis at surgery centers.
QUESTIONS TO ASK THE DOCTOR
- How many scleral buckling procedures have you performed?
- Could other treatments be an option?
- Will I have to stay in the hospital?
- Will my sight be completely restored?
- What is the probability of having another retinal detachment in the same eye?
- Am I likely to have a retinal detachment in my unaffected eye?
Thanks Jay
Long term I have 100% of my vision, though it is not corrected to 20/20 (corrected - I've got a minus 8.0 correction). Its gotten better over time (since May) and I'm hoping that it wil ultimately come back so that I can see 20/20 with glasses. One problem I do have is that there is a "wrinkle" in the center of my vision. If I look at vertical line (for instance) it will appear to "pinch" in at various places along the line. This did not become apparent for a few weeks after surgery as I could not see well enough after surgery to notice it. I am hopeful that this will go away, but the doctor says that it very well may not.
I assume by now that you've had your surgery. Hopefully all went well.
Darrell
I am 64 years old, reasoably fit and very active. I am hypertensive but have no diabetes.
I had Cataract surgery in my right eye in 2005.
In 2006 I underwent the scleral buckle procedure for retinal detachment repair in the same eye.
Last week I had catarct surgery for my left eye. Now I find that my left eye is a great deal clearer than the right eyr which continues to have a blur, but has reasonable vision.
I do know that I am a potential candidate for retinal detachment in the left ete also.
The question I have is that, with necessaary precaution and timely action in the event of any signs or symptoms would it be possible to avoid the scleral buckle procedure, which essentially is a painful procedure with prolonged post operative discomfort.
Thanks and Regards,
George Vargis.
Bangalore,
South India.
All of us had the procedures above, with good results. My retinal surgeon is a miracle-worker. I lost vision completely in left eye, and now use it for reading and close work -- amazing!
The right eye is now 20/20 -- the retina here was only partially detached and required less work. I no longer need glasses. My daughter is doing fine.
My advise is to go for the procedure. I tried the CO2 welding method prior to the buckle and I wish I did that latter first.
i went under traetment
after i week
i was ok
and gave my exams
,
thought i dnt have any problem in vision wt gods grace bt at times i do see some floating things , doctor says avoid it, is it ok?
i want to wear contact lens but i am a nbit scared ?
Thanks
Since that time I have had no problems and all is good!!!
Oh, the worry about flying? No big deal. I am, however, forbidden to indulge in boxing, bungie jumping and barroom brawls...
I continue martial arts despite some doctors opinions (Some says OK others forbidden or it's your choice).
I try to have informations about removing the buckle because i can feel it when i look on the right and sometimes cause headache (I think it's something with the pressure). If you have such informations please Email me or post.
For conclusion i would say that most of the time you still have a normal life and that's the most important. Don't worry
PS : Sorry for my English I'm French
I had a vitrectomy and buckle surgery 17 days ago. I was a good girl and did what the doctor said: no lifting, no reading, no computers, etc. etc. All I did was sit up, watch TV, walk a LOT, and eat lots of antioxidants. I missed only 6 days of work (Friday--surgery, plus the whole next week), then returned and am doing well. I read a lot at work and am on the computer much of the day. I never got any bruising either, just a little swelling and a lot of redness and some crusties every morning.
I do have a pink bump on my eyeball (incision site?) that blocks about 20 degrees of my peripheral vision. And my vision with that eye is still not good. My pupil is still dilated somewhat. From above comments, it looks like that will take more time to get back to "normal."
I started driving again after 12 days. This may be too soon, but I turn my head a lot and use great caution. I feel ok going short distances.
Thanks to you earlier posters who said to be patient with all of this. I'm not good at that, but will try to wait it out and keep hoping for continued improvement.
I had a vitrectomy and buckle surgery 3 months ago. My condition was complicated by being diagnosed with leukemia as the cause for the hemorrhage in my eye three years ago . The real problem was a torn retina that eventually healed itself causing a scar. Lucky for me that I got connected with Wills Eye in PA, the most knowledgeable and professional team of folks in the northeast US. Wills has a team of the best professionals in this field. Wills is working very hard to restore my vision. It’s going to take another 3 months before the oil bubble will be removed . So my vision is blurred for now. My best advice to all is have patience. As long as you are confident that you are being cared for by professionals knowledgeable in this field just have faith. If you are in doubt related to your care contact the Will Eye Institute . I know people that really didn’t see an appreciable difference in their sight for almost a year.
It was the biggest mistake I ever made.
The pain after the surgery was excruciating and it lasted for two days before lessening.
My eye looked horrendous after the surgery.
It looked bloody and butchered and it took many weeks to start to resemble my normal eye again.
After about 18 months, my eye looked pretty much normal from the front, but whenever I looked to the side at all, the scarring and buckle were visible, and still are visible to this day (14 years later) ... and people often ask me what it is.
But, that's not the worst part.
The worst part is the nearsightedness.
The eye is virtually useless without glasses and I can't wear glasses because the unusual prescription required to accommodate the drastic difference in vision between my two eyes causes severe headaches.
So ... for the past 14 years I've been seeing most of the world through my one good eye which has been horrible.
I still get headaches unless I keep my bad eye closed all the time, but not nearly as bad as the headaches I get while wearing the glasses.
Also, the vision in my good eye has been getting worse and worse every year as the good eye tries to adjust to match the bad eye.
I'm not saying you shouldn't have the surgery.
If every doctor you visit tells you that you'll go blind without it, then you should probably get it.
But that wasn't the case for me.
The tear in my eye was tiny and I was told there was a chance that it could get worse so I should definitely have the surgery done.
When I asked about the surgery I was told that they would simply freeze the eye that would repair it.
I wasn't told that they would be cutting up my eye and installing a permanent silicone band that would destroy my vision.
It was actually a clear-cut case of malpractice.
The doctor saw that my family was poor ... that my parents were morons and I was a naive 17-year-old, and that our insurance company would pay for the whole thing .. so he went for the gold.
I looked into filing a lawsuit a few years ago but it turns out that my parents basically signed my life away just before I went into surgery.
They never read the paperwork that the doctor handed them to sign and that paperwork made him immune to virtually every kind of lawsuit.
If I could go back to 14 years ago, I would have taken my chances with the tiny tear.
I'm now looking into getting the scleral buckle removed.
Three weeks after surgery, I started wearing contact lenses (dr. said ok)and am seeing better. My vision is still changing, but I see improvement. I still find myself closing my eye pretty often, but not as much.
My one drawback: I have lost some peripheral vision to the right side (of my buckled eye) and down below. I bet I have lost 30% of it. The doctor thinks it's likely due to the re-shaping of the retina via the buckle. And, he says if, after many months, I get the buckle removed, the retina shoul go back to normal shape and I should have this vision again. No guarantee. Anyone else notice limits on peripheral vision after a buckle was installed? I play a lot of sports and am anxious about not having a full field of vision.
I had detachments in both eyes 10 years ago. Both eyes were successfully repaired with a combination of buckles, vitrectomy, cryo. and laser. It did take a long time for the redness of the eye to go away (probably two months), but time does heal. I do have a reduction in peripheral vision. However, my impression was that this was a result of the retinal tears and an optic nerve problem, not from the buckle itself. My surgeon referred me to a neuro-ophthalmologist to have the nerve issue checked out (to rule out strokes and other stuff). 10 years later, the reduced peripheral vision hardly bothers me at all. You learn to compensate very quickly (I turn my head a lot more when driving). I don't play sports so I can't comment on that, though I can see how it would be concerning. Otherwise, I lead a very normal life, as long as I have a pair of sunglasses handy! Good luck to you!
Unfortunately, I have had intense pain for the past 3 years, antibiotics helped though. My retina specialist thinks I have an underlying infection and that is what's causing the pain. On July 27th I am getting the buckle removed and I am pretty nervous about it. Hopefully all goes well.
That said, does anyone know what we're resticted from doing (aside from bungie jumping and boxing? lol). I'm always lifting something heavy and do a lot construction. Also alot of aerobic exercizing with quick movements (both arm and head).
The bottom line is it just stinks to have this surgery (especially for the younger folks on this board). I'm 41 and wondering "why me"? I had cataract surgery 6 mos prior which is even more of a mystery - but the bottom line is it happened and life today is about recovery and moving forward.
Best wishes and prayers to everyone on this board. Things will get better.
Anyone have this done? What are the risks/complications?
I wouldn't have agreed to this procedure if the doctor wasn't so upbeat about it being removed after 3 months.
I suggest anyone going for this massively invasive procedure first decide if the cryo/laser is enough to mend the retina. Then, if that doesn't work come back a few days/weeks to have the buckle placed in. Do not agree to the cryo + buckle combo to begin with. Learn from my mistake!
DON'T GIVE UP! It takes time. At first, I could hardly see anything, my eye was swollen and as red as a tomato. I could hardly open it, it hurt and then itched like crazy. As the weeks went by, I could see more and more. It took months for the redness to go away, and it is still pink at times. But the itching, swelling and inability to move my eye like before, ALL these things are back to normal. So don't panic and lose hope. My eye does not feel the same, and I have a slight blind spot in my peripheral vision. But otherwise, my vision is pretty much like prior to surgery. And if your eye 'appears' to look smaller than before, this too, may change. Mine did, I even took pictures and was so sad to see how my right eye looked smaller. But not anymore, it looks just like before. I wish you all the best with your recovery and hope this helped you in some way.
I then had the cataract surgery on my right eye about five years ago. Ever since then, I get very bad pain in my left eye (the one with the scleral buckle) from reading, even for a few minutes. This makes my job very difficult and painful as I am a software developer. I love my work and am not interested in doing anything else. When my left eye hurts (which is most of the time), it actually feels like the bones around the eye hurt more than the eye itself.
I feel certain that the scleral buckle must be the cause of this. Can it be removed after so many years? What will the impact be on my vision? If my vision was impacted would I even be a candidate for Lasik?
Please remove the two nospam from my address to reply. I'd appreciate any ideas. Of course I am going to see my ophthalmologist, but I'd like to show up armed with a few facts.
It really can be a bad experience I do sympatise with anybody enduring the same, I guess the only good thing is that when you are coming out on the other side everything seems so much better, it does take time and you need to stay positive because eventually it does go in the right direction, follow the advice given rest try to be patient and do not lift or bend down for anything, if like me it was sheer hell and I have to say a life changing experience as I will not take so much for granted and hope not to have to go through that hell ever again.
My problems all stem from terribly vision: -16 in both eyes. (The tears originally happened in lattice areas). At any rate, I'm overjoyed that I still have my vision, even if it is reduced somewhat in my left eye. Cataract surgery will likely be up soon due to vitrectomy, and I"m a little worried about that because of the risk of detachment, but that's just something that needs to be dealt with.
As others have said, educate yourself. I realize now that I have a great doctor who took the time to talk about why buckle instead of vitrectomy first, the side effects (double vision is the worst for me), the pain associated with surgery, what the eye would look like. I saw the doctor often after my buckle surgery and he answered all the questions that I had.
Check with your doc about his/her view of the surgery - what they feel your recovery time will be, how often they will do follow up (i was in every few days for a couple of weeks, and then once a week for a while - then I had the second detachment). That follow up care is important I think. For me anyway, the surgery worked out well (even though I had the vitectromy) because I didn't really have a lot of problems post surgery. My eye is still red from that surgery (at least I don't think it's from the vitrectomy), but that's gotten a lot better recently.
I do still have a fairly dilated pupil (about 50% larger than it should be I think), but that will probably get better too - if not, *shrug*, I can still see so it doesn't matter much. I did spend about 16 weeks total on atropine so I can imagine that it will never get all the way down to what my other eye looks like.
Luckily there is the web... your article is very informative...
I am looking for help with double vision... my left eye has half a buckle. The vision is a such that I see left lower and twisted clockwise, but that is only when I am tired, expecially on the computer it might be better to were an eye patch. Driving is not so much a problem, close by is... reading, computer. I was reading about prism glasses... well, do I have to change at night when I am tired? Also, I am 50y, what can I expact getting older? What about muscle excercises? I am sure that muscles can be trained to be strong, my doctor says it does not matter, I do not think so? Any accumpuncture or accupressure points that help stimulate? Any herbs, avoiding foods etc... I am curious to hear from people in the same situation, trying to find there way back to normality... I also saw eye muscle surgery listed as a solution... So if you are a doctor that belleves there is a solution.. I would apreciate your input, feedback and perhaps help.
Please let me know if you have any idea?
Billy
I had just turned 40 in July and not even a month later, the eye doctor discovered blood in the vitreous humor. The blood was obscuring a tear in the retina. it tooks less than 24 hours from the time i noticed more floaters to a complete black spot. Thank god i paid attention to the symptoms and got to the retinal specialist immediately.
I learned that I am in a high-risk category: 40 years old, high myopia (-19, -17), prior eye surgery (Inter-collamer lens in both eyes), and prior Choroidal neo-vascularization.
I was 10 days into the recovery with a gas bubble and noticed a gray area that i didn't recall seeing before. Rushed to the retina surgeon. Had a new tear. He gave me my options and after lying with my head down for 7 days the first time, i opted for oil this time. I chose the oil so I could have somewhat of a life - moving around, working, sleeping in less restrictive positions. Of course, now that 10 more days has passed, i sort of wish I had done gas again. The oil has little tiny bubbles in it that the gas didn't have. They seem to cluster like a bunch of grapes right in my central vision. I have to tip my head straight up for a few seconds until they float to the sides. I can see fairly well when looking down - 45 - 90 degrees or so. The oil does catch the light and give weird refractions so I have to wear the old-man cataract sunglasses when i go outside or if i'm in a bright room. So far, I have had no unexpected side effects from either surgery. I do get headaches, but i think it's from not seeing clearly. It is challenging, but not impossible to drive since each eye has totally different vision. But I have just started off slowly - driving in familiar areas, when traffic is light, and not venturing out too far from home. The worst part is the "halos" i see at night from the street lights. It's pretty much impossible to drive at night. Even with that eye shut, the lack of depth perception makes me paranoid. I'm trying to get glasses of some sort for just the left eye that will reduce the glare and sharpen the central vision. So far, a magnifying glass style has improved the periphery, but the central vision is still off.
Glad to read that patience is the key. I try to stay positive, but like so many others, feel "why me?" when I'm otherwise healthy. My problem now is this horrible feeling of dread that I will be trying to live my life again and this will happen when i'm away from home: on a cruise, out of the country, etc.
I'm happy to share stories with anyone in this situation. :)
i had an accident and having severely damage in my right eye it mean doctor said retina is fully damage.cannot get a vision i had 5 times surgery now i having silicon oil in my eye been 8 years so i would like to know can we replace a new retina ? or how can i get the vision ? now i am 23 years before 8 years it happen
it's a pleasure to hear you soon...
chamni divan
sri lanka
Florent.
I only waited 4 days to go to the optometrist about the shadow on the right when I looked left. She diagnosed this possible RD and called the local hospital that specialized in eye care. In less than 6 hours, the surgery had been done by a leading opthamologist in our city.
Here's hoping that there are no further complications...find it very hard to be lazy.
I was told it could take months for recovery. My question is, will I regain any sight? I don't understand what has to happen for sight to return. From what I read about other's experiences, they are able to see after surgery, albeit not always well at first. I could see nothing but blackness prior to surgery, now post op I can detect light only. Could someone let me know what to expect. I am preparing myself for the worst.
Thank you.
5 weeks later (still not returned to work yet) I can see pretty well, the pain is infrequent and not too bad, I rarely take paracetamol to ease it and, apart from the frustrating bubble in my eye (which is now about 10% of my visual area, originally 95%) it just feels a little more short sighted. My sight gets better daily, but apparently it could take a few months to stabilize. I have started driving again this weekend without any problems, and I have been doing 2-4 hours work form home emailing, reading reports etc.
I have a consultants appointment next week, when it is likely that he will be able to tell me how my vision is doing. It wasn't a pleasant experience by any means, but it wasn't that bad on the scale of things and the recovery time is relatively short. Hopefully I will be told the surgery was successful next week.
If you have to have the surgery, it really isn't too bad in my experience and much better than the alternative of going blind.
Anyway, the whole situation was very confusing, but I trusted the doctors. When they told me I needed to have cryopexy and a scleral buckle, I accepted it. They did not entirely explain to me the risks nor did I have the time or opportunity to research and find out if this was true. Having read about these things afterwards, I feel like they rushed me into a more expensive and possibly unnecessary procedure for a small hole that cryopexy could likely have fixed by itself.
To make matters worse, I have a large bump on the top of my eye. When I asked my retinal specialist about it at a follow up, he merely smiled and said that it was from where the buckle was placed. He seemed to indicate that it would just always be there. But again, I have now read that it is supposed to mostly go away. Over a year after the surgery it is still the same size as before. It rubs against my eye socket sometimes and I can feel it moving around in there. If I close my eye and look down, it can be seen rubbing up against the eyelid. I also still have an occasional moving flash right in the area of the surgery (the same spot in my vision where the gas bubble had been for two weeks). My doctor told me my eye was fine and not to worry about the flash unless it got worse.
I also had another complication. About six months after the surgery, I was playing basketball by myself in my yard when I noticed there was a weird flash that I could see when I moved my eyes left to right. It was not a normal flash, but instead looked like a jagged line, like a river might look on a map, or the way a scar would look. It was always the same shape and located in the same area of my vision. I could see it whether my eyes were opened or closed, but only when my eyes were moving. I noticed it more when I wore contacts, but at other times I would not notice it at all. When I finally went to see my retinal specialist, I ended up getting his son instead. He asked me rather quizzically about my symptoms and did a thorough job examining BOTH my eyes, not just the one I had trouble with. Of course I later found out I was being charged double for that. He could not give me an answer for what I was seeing, but suggested that it was just the scleral sponge rubbing when I moved my eye. He said it was nothing to worry about, but he wanted me to come back in two weeks for a follow up, which made me suspicious. At the two week appointment he told me I was fine, but then asked me to come back in a month. I refused to make another appointment because it was clear to me that either something was wrong and they didn't want to tell me, or nothing was wrong and they simply wanted to bill me for extra appointments.
So what I would like to know from others who have had this surgery is whether or not you have a bump on your eye from the buckle, and if so, how long have you had it? Has it receded/gone down any? I'm concerned that I may have received a botched job.
I had a buckle put in about 3 years ago after getting hit in the face with a football. I had the operation less than 48 hours after. I was scared and it's nerve racking. My doctor explained the risks which were around vision being affected after the surgery as the buckle can change the shape of the eye and affects vision.
I had it under general anaesthetic as there was no way I could have it done under local although they did offer!!! The operation went really well and I felt worse from the anaesthetic than I did from the operation itself. My eye was sore and red which is to be expected. I put the drops in and wore a patch at night time. It was sore/unconfortable but not painful.
I can see the buckle stitch if I look to the side but it's only two small bumps so I don't mind it and I can't feel it. I had an eye test the morning after the op and my eyesight was back to normal. I didn't have any double vision or if I did it lasted a limited time. I occasionally see black dots but normally in extreme sunlight and it's certainly not even every day.. Your brain learns to filter it out..
I had a very good experience with this op and i want people to hear my story.
Anyway, everything went well for the first months... at first, my eye wouldn't move correctly and I had double vision, but that was due to the local anesthesia they had used. They told me I shouldn't wear a patch, since the eye needed some air, so instead I covered the right side of my glasses. Then I restarted using a contact lense but only in my left eye. Meanwhile, I visited the doctor weekly, and he told me that everything was going right. I waited like a month or so to use the lense in the right eye, and soon I realised that I had some kind of distorted vision, which I found out trough the internet, is called Metamorphopsy. When I told this to the doctor, he told me that it was normal, and it could be gone in a year or so.
So I went back to my life in a pretty normal way. I used to play football (or soccer) before the surgery, and I had to wait like three or four months to do it again, but luckily I was able to. In january, 6 months after the surgery, I stopped wearing sunglasses, since me eye wasn't so red and swollen. But one day I woke up early to play football with my friends, and found out these annoying floaters moving through my vision. I got really depressed when I was told that they would never go away, though in time I would get used to them. So I kept living my life until, a week or two ago, I was still seeing my eye kind of swallen, because the drooping eyelid that has been improoving for months, wasn't entirely gone. My doctor told me that it was due to the silicon buckle, and that it could still improve. He also told me that it was not advisable to remove it, since it was still helping the retina hold in place. By the way, the metamorphopsy didn't completely go away, although it's almost unnoticeable and I'm still getting used to the floaters (I have my days). The eye may still get a little pink when I use the lense, but the doctor told me this could happen, and that I should have patience.My question is, for those who have had the surgery a long time ago, does the eye recover aesthetically, or does it look smaller than before? I know it may not sound as a big deal, but I'm twenty years old and it kind of is to me. Should I wait until the buckle has no effect on the retina and try to get it removed or simply wait and see if the eye goes back to normal with the buckle in it?
thanks
Short term discomfort, but nothing too bad. No loss of vision.
Long term effects
1. Early onset cataract (20 years after the scleral buckle) - possibly as a side effect of the earlier surgery. Good outcome for cataract surgery.
Retina is good - now discharged from regular checkups after 45+ years :)
Even now if I get over tired I can become aware of it. Small price to pay for your sight though.
It was all very new tech in 1972, 5 years previous and I might well be one eyed.
Thank you
Jenny D
I am a Canadian Snow Bird, 75 years old in good health, taking no medication.
February 2017 I experienced a detachment of my retina in the left eye, subsequent examinations determined I have an operation to secure it, laser treatment along with gas in the eye ball to help hold the retina in position.
The Western Florida Eye Clinic did the procedure, the experience was amazing, the facility and interest, care and follow up by the staff and the surgeon were beyond reproach, I highly recommend this facility.
Two weeks ago, while returning to Canada on a cruise, I experienced another detachment, follow up in Toronto Weston Hospital, the facility a little dated but, again the dedication of the staff and surgeon amazing.
The surgeon determined a buckle would be best used, how ever he gave me a option of gas, oil or silicone filling, explaining the pros and cons of each, although, given the problems that could occur with the oil and the residue left, I can't imagine why anyone would choose to use it?
The decision I determined would be his, give he was the expert.
He used a gas fill again and as before vision after the surgery was purely a presence of light and slight shadows, this took four to six weeks after my initial procedure before I could "look" over the bubble (that eventually disappeared) and see 20/20.
One week after my surgery I have experienced some pain that was minimized by the occasional Aleve tablet and, as before can't determine any thing through the affected eye.
Taking it easy is the key word with as little activity as possible (fortunately I'm retired with just hobbies to keep me active).
As yet I don't know what the long term effects will be but to all who have read and contributed to this blog, I wish you a full and a speedy recovery.