Laparotomy, exploratory
Definition
A laparotomy is a large incision made into the abdomen. Exploratory laparotomy is used to visualize and examine the structures inside of the abdominal cavity.
Purpose
Exploratory laparotomy is a method of abdominal exploration, a diagnostic tool that allows physicians to examine the abdominal organs. The procedure may be recommended for a patient who has abdominal pain of unknown origin or who has sustained an injury to the abdomen. Injuries may occur as a result of blunt trauma (e.g., road traffic accident) or penetrating trauma (e.g., stab or gunshot wound). Because of the nature of the abdominal organs, there is a high risk of infection if organs rupture or are perforated. In addition, bleeding into the abdominal cavity is considered a medical emergency. Exploratory laparotomy is used to determine the source of pain or the extent of injury and perform repairs if needed.
Laparotomy may be performed to determine the cause of a patient's symptoms or to establish the extent of a disease. For example, endometriosis is a disorder in which cells from the inner lining of the uterus grow elsewhere in the body, most commonly on the pelvic and abdominal organs. Endometrial growths, however, are difficult to visualize using standard imaging techniques such as x ray, ultrasound technology, or computed tomography (CT) scanning. Exploratory laparotomy may be used to examine the abdominal and pelvic organs (such as the ovaries, fallopian tubes, bladder, and rectum) for evidence of endometriosis. Any growths found may then be removed.
Exploratory laparotomy plays an important role in the staging of certain cancers. Cancer staging is used to describe how far a cancer has spread. A laparotomy enables a surgeon to directly examine the abdominal organs for evidence of cancer and remove samples of tissue for further examination. When laparotomy is used for this use, it is called staging laparotomy or pathological staging.
Some other conditions that may be discovered or investigated during exploratory laparotomy include:
- cancer of the abdominal organs
- peritonitis (inflammation of the peritoneum, the lining of the abdominal cavity)
- appendicitis (inflammation of the appendix)
- pancreatitis (inflammation of the pancreas)
- abscesses (a localized area of infection)
- adhesions (bands of scar tissue that form after trauma or surgery)
- diverticulitis (inflammation of sac-like structures in the walls of the intestines)
- intestinal perforation
- ectopic pregnancy (pregnancy occurring outside of the uterus)
- foreign bodies (e.g., a bullet in a gunshot victim)
- internal bleeding
Demographics
Because laparotomy may be performed under a number of circumstances to diagnose or treat numerous conditions, no data exists as to the overall incidence of the procedure.
Description
The patient is usually placed under general anesthesia for the duration of surgery. The advantages to general anesthesia are that the patient remains unconscious during the procedure, no pain will be experienced nor will the patient have any memory of the procedure, and the patient's muscles remain completely relaxed, allowing safer surgery.
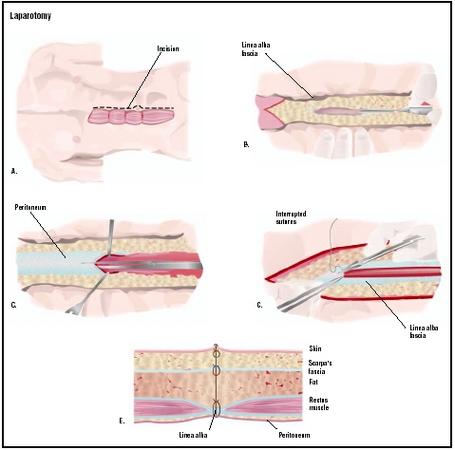
Incision
Once an adequate level of anesthesia has been reached, the initial incision into the skin may be made. A scalpel is first used to cut into the superficial layers of the skin. The incision may be median (vertical down the patient's midline), paramedian (vertical elsewhere on the abdomen), transverse (horizontal), T-shaped, or curved, according to the needs of the surgery. The incision is then continued through the subcutaneous fat, the abdominal muscles, and finally, the peritoneum. Electrocautery is often used to cut through the subcutaneous tissue as it
Abdominal exploration
The surgeon may then explore the abdominal cavity for disease or trauma. The abdominal organs in question will be examined for evidence of infection, inflammation, perforation, abnormal growths, or other conditions. Any fluid surrounding the abdominal organs will be inspected; the presence of blood, bile, or other fluids may indicate specific diseases or injuries. In some cases, an abnormal smell encountered upon entering the abdominal cavity may be evidence of infection or a perforated gastrointestinal organ.
If an abnormality is found, the surgeon has the option of treating the patient before closing the wound or initiating treatment after exploratory surgery. Alternatively, samples of various tissues and/or fluids may be removed for further analysis. For example, if cancer is suspected, biopsies may be obtained so that the tissues can be examined microscopically for evidence of abnormal cells. If no abnormality is found, or if immediate treatment is not needed, the incision may be closed without performing any further surgical procedures.
During exploratory laparotomy for cancer, a pelvic washing may be performed; sterile fluid is instilled into the abdominal cavity and washed around the abdominal organs, then withdrawn and analyzed for the presence of abnormal cells. This may indicate that a cancer has begun to spread (metastasize).
Closure
Upon completion of any exploration or procedures, the organs and related structures are returned to their normal anatomical position. The incision may then be sutured (stitched closed). The layers of the abdominal wall are sutured in reverse order, and the skin incision closed with sutures or staples.
Diagnosis/Preparation
Various diagnostic tests may be performed to determine if exploratory laparotomy is necessary. Blood tests or imaging techniques such as x ray, computed tomography (CT) scan, and magnetic resonance imaging (MRI) are examples. The presence of intraperitoneal fluid (IF) may be an indication that exploratory laparotomy is necessary; one study indicated that IF was present in nearly three-quarters of patients with intra-abdominal injuries.
Directly preceding the surgical procedure, an intravenous (IV) line will be placed so that fluids and/or medications may be administered to the patient during and after surgery. A Foley catheter will be inserted into the bladder to drain urine. The patient will also meet with the anesthesiologist to go over details of the method of anesthesia to be used.
Aftercare
The patient will remain in the postoperative recovery room for several hours where his or her recovery can be closely monitored. Discharge from the hospital may occur in as little as one to two days after the procedure, but may be later if additional procedures were performed or complications were encountered. The patient will be instructed to watch for symptoms that may indicate infection, such as fever, redness or swelling around the incision, drainage, and worsening pain.
Risks
Risks inherent to the use of general anesthesia include nausea, vomiting, sore throat, fatigue, headache, and muscle soreness; more rarely, blood pressure problems, allergic reaction, heart attack, or stroke may occur. Additional risks include bleeding, infection, injury to the abdominal organs or structures, or formation of adhesions (bands of scar tissue between organs).
Normal results
The results following exploratory laparotomy depend on the reasons why it was performed. The procedure may indicate that further treatment is necessary; for example, if cancer was detected, chemotherapy, radiation therapy, or more surgery may be recommended. In some cases, the abnormality is able to be treated during laparotomy, and no further treatment is necessary.
Morbidity and mortality rates
The operative and postoperative complication rates associated with exploratory laparotomy vary according to the patient's condition and any additional procedures performed.
Alternatives
Laparoscopy is a relatively recent alternative to laparotomy that has many advantages. Also called minimally invasive surgery, laparoscopy is a surgical procedure in which a laparoscope (a thin, lighted tube) and other instruments are inserted into the abdomen through small incisions. The internal operating field may then be visualized on a video monitor that is connected to the scope. In some patients, the technique may be used for abdominal exploration in place of a laparotomy. Laparoscopy is associated with faster recovery times, shorter hospital stays, and smaller surgical scars.
Resources
books
Marx, John A., et al. Rosen's Emergency Medicine. St. Louis, MO: Mosby, Inc., 2002.
periodicals
Hahn, David D., Steven R. Offerman, and James F. Holmes. "Clinical Importance of Intraperitoneal Fluid in Patients with Blunt Intra-abdominal Injury." American Journal of Emergency Medicine 20, no. 7 (November 2002).
other
Awori, Nelson, et al. "Laparotomy." Primary Surgery. [cited April 6, 2003]. http://www.meb.uni-bonn.de/dtc/primsurg/index.html .
"Surgery by Laparotomy." Stream OR. 2001 [cited April 6, 2003]. http://www.streamor.com/opengyn/openindex.html .
Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Depending on the reason for performing an exploratory laparotomy, the procedure may be performed by a general or specialized surgeon in a hospital operating room . In the case of trauma to the abdomen, laparotomy may be performed by an emergency room physician.
QUESTIONS TO ASK THE DOCTOR
- Why is exploratory laparotomy being recommended?
- What diagnostic tests will be performed to determine if exploratory laparotomy is necessary?
- Are any additional procedures anticipated?
- What type of incision will be used and where will it be located?
I just had this surgery done to remove adhesions and my left fallopian tube. The recovery has been rough and I am in more pain then I was prior to surgery. Honestly, if given the option again I would of chosen a lap surgery rather than this invasive one. Considering my symptoms will reuccur within time.
As intrusive as this procedure seems to be, we have patients up and moving after the first day. (this helps the organs return to their proper positioning.)
To the hysterectomy above, leaving your ovaries in was a thoughtful and good decision, though in light of your subsequent situation, you may have been better off removing them. Taking/removing body parts preemptively is not SOP, nor should it be in my opinion. Your cysts could or could not be related to adjacent fibrous tissue, and the same is true for the adjacent adhesion. Adhesion is a common problem with this or any procedure involving the perforation of the abdominal cavity.
Best of luck.
Speaking with 13 years of experience with my scar, you will have severe muscle spasms in the region of the abdomen that was operated one. I'm 20 now and I still sit in class and sometimes couple over because of the spasms. Make SURE you get a proper rehabilitation after you have any type of surgery! And make sure you blow into that stupid toy because you will get pneumonia if you don't.
Like CarolLynn I am having a laparscopic surgery that can turn into laparotomy on 12/10/08 for severe cervical stenosis. Something I have found no information about anywhere. Has anyone had either procedure for this reason?
CarolLynn, hope you have a quick day surgery and will be looking for an update.
Let me know about it.. thank you..
Keep me in touch soon..
Break aleg!!!
Let me know about it.. thank you..
Keep me in touch soon..
Break aleg!!!
My question is I have a problem late period all in my life. I went to a hopital and the doctor told me I have to have a surgery Laparoscopoic ovarian cystectomy or Laparotomy.The doctor try to explain for me evrything, But I dont have any kids and I am 33 years old married women. Do you think I will have a problem if I get pregnant or the time I deliver the baby.
i also had surgery . my doctor suspected scar tissue in the left fallopian . my fallopian tube with swelled. he had planned on taking my left fallopian out . but when he got in there discovered that he counldnt take it out at this time due to i think he said it was glue or scar tissue was to close to colon. affraid he could damage my colon.so he just removed scar tissue and fluid from the tube and burned it the tube close. hoping that it want swell on me again. but im still in pain. going to talk to doctor on monday. also having lower back pain. was your anything like im describing. thanks pam hope you are better
first surgeon did it Dec 29. Something went wrong and cause one
more closer to my pubic area. Once open can the doctor take time
to explore the entire abdomun since there is history? I know it will make it more cutting, painful and a little longer healing
tme. Do you have any suggesstions?
Thanks
Sue Terry
My daughter is looking at having a lapratomy performed on her as per the docs advise, she has allready hd an endomytriosis and the doc has suggested a laprotomy, what are the dangers associated with this procedure and is it quite safe for her to go ahead with this procedure? your advise would be greatly appreciated thanks,
Regards,
Farouk Modisane.
P.S.
Please forward your response to the following email add
Email: faroukm@webmail.co.za
Before the procedure (3 weeks before)I used to take a multivitamine and multimineral (ALL ONE)wich has 1 gr. of vitamin C, 1 cap. 200 UI vit E from wheat and mixed tocopherols, 1 cap.20 mg. chelated zinc, 1 gr. omega-3 fish oil and a very good brand of proteolitic (sistemic) enzymes, 3 caps. a day between meals...with bromelain, papain, serrapeptase, nattokinase (this 2 becuause adhesionw were suspected), amylasa, pancreatin, rutin, Co-Q 10...all this ingredients were in the enzymes. I took them 3 months before the procedure.
I stopped the omega, vit.E, vitamin C, and the enzymes 5 days before the procedure, so wouldn´t affect with coagulation during surgery...you should take care also if you take ibuprofen, naproxen, aspirin, u other for the same reasons.
I had only a myoma, little one 1.5 cm..but since my uterus was in very bad position, retroverted and to the right, they cut my ligaments and tendons that support them and reposition the uterus in the RIGHT position, chromotubacy was performed inside the fallopian tubes to check for pattency and the frimbias and everything was ok. The scar (incision) was horizontal and 4 to 4.5 inches in lenght (not so small)
I clean my scar every day and apply a good concentrated and clean arnica cream 2 or 3 times a day.
After the surgery I take 50 gr. of rice and pea protein daily mixed with a juice divided in 2 doses, one in the morning and one in the evening, I add 4 extra grams of L-Lysine and 2 gr. of L-Proline with each protein shake. I started to take 3 gr. of buffered time-release vitamin C with flavonoids 3 days after the surgery (for collagen production enhancement).
I take enzymes as well, but without serrapeptase and nattokkinase, I read I must wait some days, but they have bromelain and papain to assist inflammation, and the other ingredients, protease, amylase, rutin, magnesium, Co-Q 10, I take 3 , 2 hours away from meals.And finally I take a good probiotic separated from antibiotics. Also 1 scoop of All one (multivitamin and multimineral with orange or carrot juice)
The 3rd day for me was the most difficult, at 5 days from surgery I´m feeling so much better. I was given 10 mg. ketorolac for pain every 8 hours, and prednisone 20 mg for 10 days (later will be 3 days on 10 mg and 2 days on 5mg), loratadine 10 mg.for 20 days
Can you please give me your opinion regarding this. do i need to undergo exploratory lap/open surgery? i really need your advice... thanks
can you please send your response to my e-mail add: eliza.john97@yahoo.com
I had the surgery 2 weeks 16 days ago and had 31 staples, My digestive system was the same, i ended up having 3 enimas, senna and lactose, i'm hardley eating much as its painful but it does get easier, i have good and bad days.i had bad pain in my tummy once i have eaten and the doctoe advised me to stop taking anti inflammitry tablets as the can irritate the gut.
good luck in your recovery x
I had the surgery 2 weeks 16 days ago and had 31 staples, My digestive system was the same, i ended up having 3 enimas, senna and lactose, i'm hardley eating much as its painful but it does get easier, i have good and bad days.i had bad pain in my tummy once i have eaten and the doctoe advised me to stop taking anti inflammitry tablets as the can irritate the gut.
good luck in your recovery x
I've had these pains since 2008 but always brushed it off as bad period pain. Cysts did not cross my mind that time. I wrestled with the pain all of 2009, still thinking it's just bad period pain. The pain would sometimes be SO bad during first or second day of period, I have to take painkillers to stop them. I break out into cold sweats and shiver from wrestling with the pain sometimes, just waiting for the painkillers to kick in. Sometimes, the pain makes me feel like I have gastric and that I feel like throwing up. The pain would also act up even when I'm NOT having my period. Feels like it's pushing on my pelvic floor. Sometimes it makes me feel bloaty, like there's so much air inside. I try to pass wind, but nothing comes out. I try to pass motion, but nothing comes out. Though nothing comes out, I feel pain in the rectum region. Sometimes, i DO pass wind or motion. It gives me temporary relief from the pain, and then it acts up again. Other times out of the blue, the pain would be at my lower abdomen and at the top of my legs (upper thigh on the sides). Feels like it's attacking my nerves in my hips, and I get the sensation that it's sorta like becoming numb.
A few days ago, I saw a gynae and she explained to me that it is most likely endometriosis. She recommends removal by laparotomy. I asked about doing the less-invasive laparoscopy, she said she could do it but I had to keep in mind that there was always the possibility that a laparotomy had to be done if laparoscopy is not sufficient.
I need advice. What are the risks if i DO or DO NOT do a laparotomy? I heard that with a laparotomy, they'd be able to get a better look and clean out the cysts and endometriamas more thoroughly than with laparoscopy?
I had this surgery over 4 weeks ago now to remove a hematoma, and am also experiencing the same kind of digestive problems... stomach pains, painful bloating and gas, the only difference is I also have diarrhoea! Nice! Please tell me that this has eased for you... I've gotta believe this gets better!!!
Thanks!
The second night after my surgery I got up out of bed too quickly and it hurt in my left side inside. The pain subsided. On the fourth day I was walking around, slowly for about 20 minutes and the same pain came back inside my left side. It subsided when I rested. There are no bruises, no pus, no bleeding on the three areas where the incisions were made. The stirry strips have been left in place, but my gauze and special tape has been replaced twice.
Am I just being paranoid, is this normal? I also hate to say it, but it has been 2 weeks and a couple of days and I really wish I could walk more and be not totally active as I was previously, but just be able to walk some more - maybe like 2 miles, I was used to running about 4-5 miles 3 times a week. How long does it take to heal? I have also noted 2 days ago that not at the IV site, but just below it a vein close to me left wrist bone has swollen up/raised, it feels like a bruise, should I be concerned about that? I also stopped taking the painkillers three days ago, I don't want to be constipated. Also it has been just 2 weeks and a cpl of days and already my job is asking when I think I am going to be ready to come back, my recovery was 4-6 weeks. Also my sticthes are scheduled to be removed five weeks after my surgery - is this normal as well? Can someone provide feedback about recovery time and what patients will typically experience after surgery.
since today the dragging has reappeared, i have to see the surgeon for a post op in december and i am worried he may want to repeat the procedure.
any advice would be helpful.
I have a genuine problem please help me for God sake. I m 33 years old , married since 7 years and 4 months, Feb 2011 , i got pregnant first time, but it was ectopic pregnancy in my right tube. Doctor recommended Laparotomy and said ur left tube is also blocked or damaged, due to Laparoscopy done in 2008. They also said that ur tube size is small of 4cm. They removed my Two months Ectopic pregnancy with my right tube. and left my left side tube. now please guide me whether i become mother or not? i have no kid and want to concieve i m too tenssed please help me.. i m waiting ur urgent reply
Mamoonah
Although post-op recovery was quite unpleasant with lots of pain and gripey wind pain, I am finally feeling more normal again. I do have a feeling of numbness combined with a tingling sensation between my umbilicus and the incision line which gets irritated by clothing.This is usually by the day end and when I have been walking a lot.
My surgeon applied a wide dressing strip along the wound and has advised me to change it daily and to continue applying Micropore tape for up to 6 months to prevent scarring. Already my scar is very fine and is becoming difficult to see.
Although post-op recovery was quite unpleasant with lots of pain and gripey wind pain, I am finally feeling more normal again. I do have a feeling of numbness combined with a tingling sensation between my umbilicus and the incision line which gets irritated by clothing.This is usually by the day end and when I have been walking a lot.
My surgeon applied a wide dressing strip along the wound and has advised me to change it daily and to continue applying Micropore tape for up to 6 months to prevent scarring. Already my scar is very fine and is becoming difficult to see.
She is in so much pain sometimes she just wants her life to end, this is crazy and she doesn't mean it but I don't blame her ... I cannot believe how long it is taking.
Andrew
Ottawa, Ontario
hi.
i did a laparoscopy in 2007 that showed that my tubes has multiple adhesions, and after my operation the resurts said that my chances of conceiving are poor.. anyone with help any information what to do after. i dont have a child of my own and im 34 years old.
What could it be. I am scared to undergo another surgery as I was put on oxygen for days immediately after surgery.
Can anyone tell me if they have been successful with recovery to start excercising again? its been 8 weeks since my lap and i used to be quite active in gym and in general. Right now i feel like it wont be happening for a few months still but after reading some of the above im starting to think my days of sit ups are over. is this right? i understand that everyone is different but i havent read to many good luck stories as yet.
tony
So I had a wreak 7 years ago and I have abdominal trauma and I also a laparotomy surgery and they cut me down my stomach. I am now pregnant and I'm trying to find out if I'm going to be ok?
Any help please
This procedure lead to a leak of his intestine that caused an infection inside that could not be contained after 10 days with antibiotics. He had to go into surgery again to clean and repair any damage. His condition severely deteriorated and was put into icu immediately after surgery where he spent the next 3 weeks intubated. They kept him under fentanyl the entire time. Week 4 in the ICU his kidney failed and had dialysis once a day which quickly became twice a day until he passed 4.5 weeks in the icu. I just wanted to share my experience and mention that this procedure requires a very long and difficult recovery if you are young and no recovery for my father in law age 80 who only had only mild stomach pains prior.
Any thoughts?
Wow I'm not alone! Here's my case
I'm scheduled for a laparoscopic myomectomy in a couple of weeks for a LARGE 11 by 11cm subserosal uterine fibroid that bulges out sometimes which kinda makes me look like I'm expecting.
I feel the lump when I'm laying down on my back mostly; its large, firm and mobile (it moves when i apply a bit of pressure). I'm only 23 yrs old going on 24. Also my period has become quite irregular and i feel very heavy at times. There is an extremely low chance this myomectomy would be converted to a laparotomy as per the surgeon.
I'm worried that this fibroid may be uterine sarcoma/cancer that has been misdiagnosed. I'm scared that during the surgery, the doctor might have to switch to a laparotomy due to the SIZE and nature of this growth. If a laparoscopic myomectomy is performed, I'm worried that the morcellation technique would worsen the growth or state. I'm scared of the general idea and nature of surgery, either laparoscopic or open.
I'm trying to stay hopeful, positive and optimistic about this procedure and my future but the truth is that I'm really scared, stressed and worried, especially closer to date. I definitely also want to keep my chances and options of having kids naturally.
I want to completely trust the diagnosis and doctors but i always have doubt, and that's fine, nothing is 100% and people are different. So many questions.
Please kindly advise on my concerns and share your thoughts.
Thanks!