Heart transplantation
Definition
Heart transplantation, also called cardiac transplantation, is the replacement of a patient's diseased or injured heart with a healthy donor heart.
Purpose
Heart transplantation is performed on patients with end-stage heart failure or some other life-threatening heart disease. Before a doctor recommends heart transplantation for a patient, all other possible treatments for his or her disease must have been attempted. The purpose of heart transplantation is to extend and improve the life of a person who would otherwise die from heart failure. Most patients who have received a new heart were so sick before transplantation that they could not live a normal life. Replacing a patient's diseased heart with a healthy, functioning donor heart often allows the recipient to return to normal daily activities.
Demographics
Patients are not limited by age, sex, race, or ethnicity. In 1999, the primary diagnoses of adult patients receiving cardiac transplantation include coronary artery disease, cardiomyopathy, congenital diseases, and re-transplantation associated with organ rejection. Characteristics of patient presentation include cardiomegaly, severe dyspnea, and peripheral edema.
Adults with end-stage heart failure account for 90% of heart transplant recipients. Pediatric patients make up the remaining 10%, with 50% of those going to patients under the age of five. In the United States, patients that receive heart transplant are 73% male, 77% are white, 19% are ages 35–49, and 51% are ages 50–64.
Because healthy donor hearts are in short supply, strict rules dictate criteria for heart transplant recipients. Patients who may be too sick to survive the surgery or the side effects of immunosuppressive therapy would not be good transplant candidates.
These conditions are contraindications for heart transplantation:
- active infection
- pulmonary hypertension
- chronic lung disease with loss of more than 40% of lung function
- untreatable liver or kidney disease
- diabetes that has caused serious damage to vital organs
- disease of the blood vessels in the brain, such as a stroke
- serious disease of the arteries
- mental illness or any condition that would make a patient unable to take the necessary medicines on schedule
- continuing alcohol or drug abuse
Description
Patients with end-stage heart disease unresponsive to medical treatment may be considered for heart transplantation. Potential candidates must have a complete medical examination before they can be put on the transplant waiting list. Many types of tests are done, including blood tests, x rays, and tests of heart, lung, and other organ function. The results of these tests indicate to doctors how serious the heart disease is and whether or not a patient is healthy enough to survive the transplant surgery .
Organ waiting list
A person approved for heart transplantation is placed on the heart transplant waiting list of a heart transplant center. All patients on a waiting list are registered with the United Network for Organ Sharing (UNOS). UNOS has organ transplant specialists who run a national computer network that connects all the transplant centers and organ-donation organizations.
When a donor heart becomes available, information about the donor heart is entered into the UNOS computer and compared to information from patients on the waiting list. The computer program produces a list of patients ranked according to blood type, size of the heart, and how urgently they need a heart. Because the heart must be transplanted as quickly as possible, a list of local patients is checked first for a good match. After that, a regional list and then a national list are checked. The patient's transplant team of heart and transplant specialists makes the final decision as to whether a donor heart is suitable for the patient.
The transplant procedure
When a heart becomes available and is approved for a patient, it is packed in a sterile cold solution and rushed to the hospital where the recipient is waiting. The recipient will be contacted to return to the hospital if chronic care occurs outside of the hospital.
A description of the procedure follows:
- General anesthesia is provided by an anesthesiologist experienced with cardiac patients.
- Intravenous antibiotics will prevent bacterial wound infections.
- The patient is put on a heart/lung machine, which performs the functions of the heart and lungs by pumping the blood to the rest of the body during surgery. This procedure is called cardiopulmonary bypass.
- Once the donor heart has arrived to the operating room , the patient's diseased heart is removed.
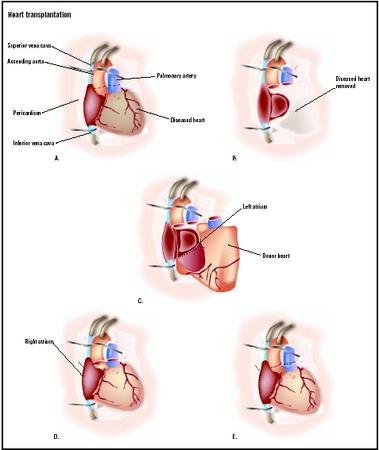
- The donor heart is attached to the patient's blood vessels, including the atrium(s), pulmonary artery, and aorta.
- After the blood vessels are connected, the new heart is perfused with the patient's blood and begins beating. If the heart does not begin to beat immediately, the surgeon may use defibrillation to gain a productive rhythm.
- The patient is taken off the heart-lung machine.
- The new heart is stimulated to maintain a regular beat with medications and/or a pacemaker for two to five days after surgery, until the new heart functions normally on its own.
Heart transplant recipients are given immunosuppressive drugs to prevent the body from rejecting the new heart. These drugs are usually started before or during the heart transplant surgery. Immunosuppressive drugs keep the body's immune system from recognizing and attacking the new heart as foreign tissue. Normally, immune system cells recognize and attack foreign or abnormal cells such as bacteria, cancer cells, and cells from a transplanted organ. The drugs suppress the immune cells and allow the new heart to function properly. However, they can also allow infections and other adverse effects to occur to the patient.
Because the chance of rejection is highest during the first few months after the transplantation, recipients are usually given a combination of three or four immunosuppressive drugs in high doses during this time. Afterwards, they must take maintenance doses of immunosuppressive drugs for the rest of their lives.
Cost and insurance coverage
The total cost for heart transplantation varies, depending on where it is performed, whether transportation and lodging are needed, and whether there are any complications. The costs for the surgery and first year of care are estimated to be about $250,000. The medical tests and medications after the first year cost about $21,000 per year.
Insurance coverage for heart transplantation varies, depending on the policy. Most commercial insurance companies pay a certain percentage of heart transplant costs. Medicare pays for heart transplants if the surgery is performed at Medicare-approved centers. Medicaid pays for heart transplants in 33 states and in the District of Columbia.
Diagnosis/Preparation
Before patients are put on the transplant waiting list, their blood type is determined so a compatible donor heart can be found. The heart must come from a person with the same blood type as the patient, unless it is blood type O negative. A blood type O negative heart is a universal donor and is suitable for any patient regardless of blood type.
A panel reactive antibodies (PRA) test is also done before heart transplantation. This test tells doctors whether or not the patient is at high risk for having a hyperacute reaction against a donor heart. A hyperacute reaction is a strong immune response against the new heart that happens within minutes to hours after the new heart is transplanted. If the PRA shows that a patient has a high risk for this kind of reaction, then a crossmatch is done between a patient and a donor heart before transplant surgery. A crossmatch checks how close the match is between the patient's tissue type and the tissue type of the donor heart. Most people are not high risk, and a crossmatch usually is not done before the transplant because the surgery must be done as quickly as possible after a donor heart is found.
While waiting for heart transplantation, patients are given treatment to keep the heart as healthy as possible. They are regularly checked to make sure the heart is pumping enough blood. Intravenous medications may be used to improve cardiac output. If these drugs are not effective, an intra-aortic balloon pump or ventricular-assist device can maintain cardiac output until a donor heart becomes available.
Aftercare
Immediately following surgery, patients are monitored closely in the intensive care unit (ICU) of the hospital for 24–72 hours. Most patients need to receive oxygen for four to 24 hours following surgery. Continuous cardiac monitoring is used to diagnose and treat donor heart function. Renal, liver, brain, and pulmonary functions are carefully monitored during this time.
Heart transplant patients start taking immunosuppressive drugs before or during surgery to prevent immune rejection of the heart. High doses of immunosuppressive drugs are given at this time, because rejection is most likely to happen within the first few months after the surgery. A few months after surgery, lower doses of immunosuppressive drugs usually are given, and then must be taken for the rest of the patient's life.
For six to eight weeks after the transplant surgery, patients usually come back to the transplant center twice a week for physical examinations and medical tests, which check for any signs of infection, rejection of the new heart, or other complications.
In addition to physical examination , the following tests may be done during these visits:
- laboratory tests to check for infection
- chest x ray to check for early signs of lung infection
- electrocardiogram (ECG) to check heart function
- echocardiogram to check the function of the ventricles in the heart
- blood tests to check liver and kidney function
- complete blood counts (CBC) to check the numbers of blood cells
- taking of a small tissue sample from the donor heart (endomyocardial biopsy) to check for signs of rejection
During the physical examination, the blood pressure is checked and the heart sounds are listened to with a stethoscope to determine if the heart is beating properly and pumping enough blood. Kidney and liver functions are checked because these organs may lose function if the heart is being rejected.
An endomyocardial biopsy is the removal of a small sample of the heart muscle. This is done by cardiac catheterization . The heart muscle tissue is examined under a microscope for signs that the heart is being rejected. Endomyocardial biopsy is usually done weekly for the first four to eight weeks after transplant surgery, and then at longer intervals after that.
Risks
The most common and dangerous complications of heart transplant surgery are organ rejection and infection. Immunosuppressive drugs are given to prevent rejection of the heart. Most heart transplant patients have a rejection episode soon after transplantation. Rapid diagnosis ensures quick treatment, and when the response is quick, drug therapy is most successful. Rejection is treated with combinations of immunosuppressive drugs given in higher doses than immunosuppressive maintenance. Most of these rejection situations are successfully treated.
Infection can result from the surgery, but most infections are a side effect of the immunosuppressive drugs. Immunosuppressive drugs keep the immune system from attacking the foreign cells of the donor heart. However, the suppressed immune cells are then unable to adequately fight bacteria, viruses, and other microorganisms. Microorganisms that normally do not affect persons with healthy immune systems can cause dangerous infections in transplant patients taking immunosuppressive drugs.
Patients are given antibiotics during surgery to prevent bacterial infection. They may also be given an antiviral drug to prevent virus infections. Patients who develop infections may need to have their immunosuppressive drugs changed or the dose adjusted. Infections are treated with antibiotics or other drugs, depending on the type of infection.
Other complications that can happen immediately after surgery are:
- bleeding
- pressure on the heart caused by fluid in the space surrounding the heart (pericardial tamponade)
- irregular heart beats
- reduced cardiac output
- increased amount of blood in the circulatory system
- decreased amount of blood in the circulatory system
About half of all heart transplant patients develop coronary artery disease one to five years after the transplant. The coronary arteries supply blood to the heart. Patients with this problem develop chest pains called angina. Other names for this complication are coronary allograft vascular disease and chronic rejection.
Normal results
Heart transplantation is an appropriate treatment for many patients with end-stage heart failure. The outcomes of heart transplantation depend on the patient's age, health, and other factors. According to a year 2000 data from the Registry of the International Society for Heart and Lung Transplantation (ISHLT), 81% of transplant recipients survive one year. During the first year, infection and acute rejection are the leading causes of death. A constant 4% decrease occurs yearly after the first year as the incidence of coronary allograft vascular disease increases.
Pediatric patients less than one year of age are least likely to reject the donor heart, but 30% of older pediatric patients succumb to transplant rejection.
After transplant, most patients regain normal heart function, meaning the heart pumps a normal amount of blood. A transplanted heart usually beats slightly faster than normal because the heart nerves are cut during surgery. The new heart also does not increase its rate as quickly during exercise . Even so, most patients feel much better and their capacity for exercise is dramatically improved from before they received the new heart. About 90% of survivors at five years will have no symptoms of heart failure. Patients return to work and other daily activities. Many are able to participate in sports.
Alternatives
End-stage heart disease is associated with a high mortality rate even with associated medical treatment. With as many as 30,000 patients awaiting transplantation according to the ISHLT database, and only 2,196 transplants performed in 2000, viable alternatives are necessary. Additionally, 500,000 patients in the United States are diagnosed with cardiac failure, adding to the almost 4.5 million already affected. Data from the REMATCH trial, published in 2001, demonstrated ventricular assist to be a viable alternative for patients not eligible for cardiac transplant compared to medical therapy alone. After one year, quality of life was improved in patients who received ventricular assist device compared to medical therapy alone. Additionally, biventricular pacing and myocardial resection for ventricular restoration show promising results. Adding destination therapies such as the AbioCor total artificial heart and the Thoratec Heart-Mate VE may provide other alternatives for the transplant candidate.
Resources
books
Bellenir, Karen, and Peter D. Dresser, eds. Cardiovascular Diseases and Disorders Sourcebook. Detroit: Omnigraphics, 1995.
Texas Heart Institute. Heart Owner's Handbook. New York: John Wiley and Sons, 1996.
Rother, Anne L., and Charles D. Collard. "Anesthetic Management for Cardiac Transplantation." In A Practical Approach to Cardiac Anesthesia, 3rd edition, edited by Frederick A. Hensley, Donald E. Martin, and Glenn P. Gravlee. Philadelphia, PA: Lippincott Williams & Wilkins, 2003.
organizations
American Council on Transplantation. P.O. Box 1709, Alexandria, VA 22313. (800) ACT-GIVE.
Health Services and Resources Administration, Division of Organ Transplantation. Room 11A-22, 5600 Fishers Lane, Rockville, MD 20857.
United Network for Organ Sharing (UNOS). 1100 Boulders Parkway, Suite 500, P.O. Box 13770, Richmond, VA 23225-8770. (804) 330-8500. http://www.unos.org .
other
Craven, John, and Susan Farrow. "Surviving Transplantation." SupportNET Publications, 1996-1997.
"Facts About Heart and Heart/Lung Transplants." National Heart, Lung, and Blood Institute, November 27, 1998 [cited March 3, 1998]. http://www.nhlbi.nih.gov/index.htm .
"What Every Patient Needs to Know." United Network for Organ Sharing (UNOS). http://www.unos.org/frame_Default.asp?Category=Patients .
Toni Rizzo
Allison J. Spiwak, MSBME
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
According to the American Heart Association, there are currently 196 centers performing cardiac transplant surgery in the United States. To meet criteria to be listed with UNOS, centers must perform 12 cardiac transplants per year with a one-year survival of 70%. A cardiac surgeon with additional training in transplant surgery will be consulted to perform the operation.
QUESTIONS TO ASK THE DOCTOR
- Is the transplant center listed with UNOS?
- How many transplants have been performed at this center in the last year, and what is the one-year survival rate?
- May I be introduced to the transplant coordinator and any other physicians who may be involved in patient care?
- What precautions are in place to guarantee that the donor heart will be a correct match?
- If the donor heart is rejected, what is the likelihood of another donor heart becoming available?
- Given patient specific information, how long is the wait on the transplant list?
- What type of medical treatment will be supplied while awaiting cardiac transplantation?
- What alternative therapies are available for destination therapy, and are those devices available at the transplant center?
it's quite interesting.
Bianca
I like to get some knowledge of heart transplantation. I was just informed that I can be a candidate for a heart transplant, since I have had 2 Open heart surgeries, l5 heart catherizations, a defriberlator and a pacemaker and now just went through a test and upon exertion my heart levels are quite high. When are you put on this list? At end stage or do they put you on the heart transplant list now and wait until it get worse?? I did read that you can not be overweight, well by the time I need a transplant I have about 25 pounds to loose, would I still be a candidate if I loose that quickly and keep it off. There are so many questions and who makes the final decision? Thanks for all of your help.
combat Veteran.I suffer from Agent Orange and also was one of the survivors of Chinese poison Heparin.11/4/2007! I was given the Pill lecture stating i had reached maximum medical improvement and would not be restarted,then after them hearing me discuss this on national radio i received a phone call early Monday morning stating i may had misunderstood.Now,i have been told i am not on a Waite list for transplant now,at the age of 64 that they are most likely won't reach that is the cut off! When the Doctor asked what keeps me going long after most in my condition.I explained,just to annoy you Still Practicing Doctors! must be a Marine thing!
Ihope this has been helpful my daughter had aheart transplant nearly five years ago she is doing well and there are no major concerns. You realise that meds indefinitely are the least of the worries. As this is all for QUALITY OF LIFE yes, and quantity of life would be very short without those all important medicines. Thanks and good luck, that little bit of luck goes a long way when you swim in these waters. Kayte