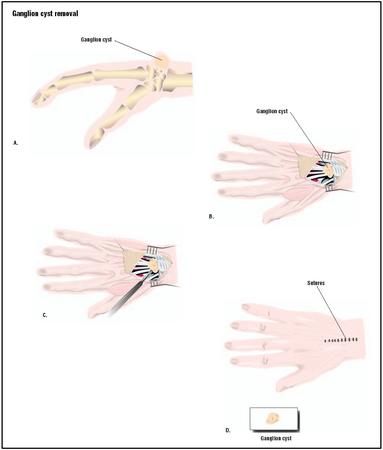
Ganglion cyst removal
Definition
Ganglion cyst removal, or ganglionectomy, is the removal of a fluid-filled sac on the skin of the wrist, finger, or sole of the foot. The cyst is attached to a tendon or a joint through its fibers and contains synovial fluid, which is the clear liquid that lubricates the joints and tendons of the body. The surgical procedure is performed in a doc tor's office. It entails aspiration, or draining fluid from the cyst with a large hypodermic needle. The cyst may also be excised (removed by cutting).
Purpose
Ganglion cysts are sacs that contain the synovial fluid found in joints and tendons. They are the most common forms of soft tissue growth on the hand and are distinguished by their sticky liquid contents. The cystic structures are attached to tendon sheaths via a long thin tube-like arm. About 65% of ganglion cysts occur on the upper surface of the wrist, with another 20%–25% on the volar (palm) surface of the hand. Most of the remaining 10%–15% of ganglion cysts occur on the sheath of the flexor tendon. In a few cases, the cysts emerge on the sole of the foot.
Ganglion cysts have appeared in medical writing from the time of Hippocrates (c. 460–c. 375 B . C .). Their exact cause is unknown. There are some indications, however, that ganglion cysts result from trauma to or deterioration of the tissue lining in the joints that secretes synovial fluid.
Ganglion cysts can emerge quite quickly, and can disappear just as fast. They are benign growths, usually causing problems in the functioning of the joints or tendons of the hand or finger only when they are large. Many people do not seek medical attention for ganglion cysts unless they cause pain, affect the movement of the nearby tendons, or become particularly unsightly.
An old traditional treatment for a ganglion cyst was to hit it with a Bible, since the cysts can burst when struck. Today, cysts are removed surgically by aspiration but often reappear. Surgical excision is the most reliable treatment for ganglion cysts, but aspiration is the more common form of therapy.
Demographics
Ganglion cysts account for 50%–70% of all soft tissue tumors of the hand and wrist. They are most likely to occur in adults between the ages of 20 and 50, with the female: male ratio being about 3: 1. Most ganglion cysts are visible; however, some are occult (hidden). Occult cysts may be diagnosed because the patient feels pain in that part of the hand or has noticed that the tendon cannot move normally. In about 10% of cases, there is associated trauma.
Description
Patients are given a local or regional anesthetic in a doctor's office. Two methods are used to remove the cysts. Most physicians use the more conservative procedure, which is known as aspiration.
Aspiration
- An 18- or 22-gauge needle attached to a 20–30-mL syringe is inserted into the cyst. The doctor removes the fluid slowly by suction.
- The doctor may inject a corticosteroid medication into the joint after the fluid has been withdrawn.
- A compression dressing is applied to the site.
- The patient remains in the office for about 30 minutes.
Excision
Some ganglion cysts are so large that the doctor recommends excision. This procedure also takes place in the physician's office with local or regional anesthetic.
Excision of a ganglion cyst is performed as follows:
- The physician palpates, or feels, the borders of the sac with the fingers and marks the sac and its periphery.
- The sac is cut away with a scalpel.
- The doctor closes the incision with sutures and applies a bandage.
- The patient is asked to remain in the office for at least 30 minutes.
Diagnosis/Preparation
Ganglion cysts are fairly easy to diagnose because they are usually visible and pliable to the touch. They are distinguished from other growths by their location near tendons or joints and by their fluid consistency. Ganglion cysts are sometimes confused with a carpal boss (a bony, non-mobile spur on the top of the wrist), but can usually be distinguished by the fact that they can be moved and are usually less painful for the patient.
The doctor may schedule one or more imaging studies of the hand and wrist. An x-ray may reveal bone or joint abnormalities. Ultrasound may be used to diagnose the presence of occult cysts.
Aftercare
Patients should avoid strenuous physical activity for at least 48 hours after surgery and report any signs of infection or inflammation to their physician. A follow-up appointment should be scheduled within three weeks of aspiration or excision. Excision may result in some stiffness after the surgery and some difficulties in flexing the hand because of scar tissue formation.
Risks
Aspiration has very few complications as a treatment for ganglion cysts; the most common aftereffects are infection or a reaction to the cortisone injection. Complications of excision include some stiffness in the hand and scar formation. Ganglion cysts recur after excision in about 5–15% of cases, usually because the cyst was not completely removed.
Normal results
Aspirated ganglion cysts disappear and cause no further symptoms in 27–67% of cases. They may, however, reoccur and require repeated aspiration. Aspiration combined with an injection of cortisone has more success than aspiration by itself. Excision is a much more reliable procedure, however, and the stiffness that the patient may experience after the procedure eventually goes away. The formation of a small scar is normal.
Morbidity and mortality rates
The only risks for ganglion cyst removal are infections or inflammation due to the cortisone injection. There is a small risk of damage to nearby nerves or blood vessels.
Alternatives
Alternatives to aspiration and excision in the treatment of ganglion cysts include watchful waiting and resting the affected hand or foot. It is quite common for ganglion cysts to fade away without any surgical treatment.
Resources
books
"Common Hand Disorders." Section 5, Chapter 61 in The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
Ferri, Fred F. Ferri's Clinical Advisor: Instant Diagnosis and Treatment . St. Louis, MO: Mosby, Inc., 2003.
Ruddy, Shaun, et al. Kelly's Textbook of Rheumatology , 6th ed. Philadelphia, PA: W.B. Saunders, 2001.
periodicals
Tallia, A. F., and D. A. Cardone. "Diagnostic and Therapeutic Injection of the Wrist and Hand Region." American Family Physician 67 (February 15, 2003): 745-750.
Nancy McKenzie, PhD
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Aspiration or excision to treat ganglion cysts is done by primary care doctors as well as orthopedic surgeons. The procedures may be performed in the doctor's office or at an outpatient clinic.
QUESTIONS TO ASK THE DOCTOR
- May I continue to exercise and continue my other regular activities with this cyst?
- Would you recommend removal rather than aspiration?
- How effective is aspiration in preventing these cysts from recurring?
- How successful have excisions been with your patients?
Any tips?
Kimmie
I now have one on my left wrist and am planning to go back to the doctor who did the first one. The only thing I would recommend you do is to find a doctor who specializes. Here we have a practice where each doctor while he can see or treat you for any break, etc, they each have one area that they are best at. (i.e., one does toes and feet, one does hands and fingers, etc).
many thanks dave
I can't afford to have something come back again...worse?
I have not read of any other cysts becoming elongated, should this concern me?
I can't bend my wrist further than a 120° angle, and it is in a lot of pain from when I accidentally bent it the other day. I wear a brace when it hurts, but right now it's not helping. Seems to make it even weaker.
I'm sick of my wrist being so weak. I can barely do anything with it. I'm considering the surgery, but I'm afraid it'll make things worse.
Anybody had it and it went well?
Had major surgery on my foot ganglion cyst 6 months ago. Paid a fortune for it, even though I have insurance. Well, at least I met my huge deductible for the year. ha.
Now have a nasty brownish 5 inch scar down the top of my foot. Did I mention I had to be on crutches for a month too? Ugh. At least I had high hopes it was done with and I was cured of it forever.
NOT!!! It's already coming back right where it started the last time, in the same place. Already the little bump is the diameter of a dime protruding underneath the skin where it all started in the first place....before it took over the near entire surface of the top of my foot like last time.
Starts out as a small little marble looking thing under the skin and already it is junctioning sideways in the form of a rectangle! It doesn't really hurt all that much again yet, it just feels like a giant pimple underneath my skin that would happily SPEW its little heart out if given a needle for relief. Sorry, I know that sounds grose. But I know it's going to get huge again like last time. That's how it's been so far. Numerous aspirations and cortisone injections. Finally getting too thick for that form of therapy, then requiring surgery.
I didn't get to see what was actually taken out because I was put under for an hour while it was surgically removed, but at my followup appointment all the doctor and nurse could talk about was that it was the 'hugest one they had ever SEEN, and it looked like a gigantic jellyfish! Wish I could have seen it for myself before it got sent off to the lab. Oh well.
Am going back to the same Podiatrist Specialist after another ordered MRI next week and will probably have to undergo either another aspiration and cortisone injection in the office. Which never helps. Seems the little devil feeds off off all that attention.
Mine was from an accident from dropping a vacuum cleaner on my foot 3 years ago. A lesson learned. Wear steel toed boots in everything you do...or risk dealing with leaky tendon juice that turns thick in no time, and requires surgery after surgery to get that root sack cut off somehow.
Maybe I should name the little guy something, and just learn to live with it?...I don't know. Haven't read anything too promising on this website. If I am ever found to be permanently rid of this, and happen to turn out to be a SUCCESS STORY, I will be sure to post it on this website to give others some form of hope and relief from this ridiculous burden ! : )
amie
Now I have a cyst at the base of my finger! Hurts worse each day I am going to have it removed in January! What makes these things come back? Good luck to each one of you.
About 1 1/2 months ago, after feeling pain in my left foot, this thing appeared all of a sudden! I had been feeling pain there but had no idea a ganglion cysts could form on the top of my foot. Off to the doc I went. After an x-ray and an MRI a ganglion cysts was diagnosed. After aspiration of very little fluid as it had solidified, the area was "traumatized" with the needle in hopes of it dissipating. Well, two to three days later, it had smoothed out and it started looking like a foot again. Yeah! Well, it's been two weeks now and a small area looks like it it starting again. Oh boy here we go again! After researching I discovered that the rate do reoccurrence can be as high as 80%. Some of us are just prone to ganglion cysts. They really do not know what make them for other than repeated use of the area. The doctor has done everything possible to help this situation. There is no blame to place. There is only more research to be done. The good news no matter how painful or disruptive your cyst(s) are, it or (they) are BENIGN!
Oh, and it's not really bugging me at all, unless I bend my toe too far. Otherwise, i can apply pressur and it's not too bad. Oh, and for anyone who wants to tell me "Just smack it!" I can't for 2 reasons. 1)I'd probably hurt my toe and 2)I'm a chicken
Can you ever get rid of them & have them not come back?
Many friends of mine told me that it can be cured completely with good accupunture doctor, some know and confirm that by seeing their family/friends, some even went through with accupunture doctor. Don't waste your time and your money with mri/surgery because the cyst will come back very soon after the surgery!
Has or does anyone out there had/have a ganglion cyst on the middle joint of their finger? NOT at the base, NOT at the tip--but on the CENTER joint? I've had one for nearly 2 years now and it just will NOT go away--needless to say in my line of work I'm always using my hands, as I'm a cook and barista at two different cafes.ity
Any suggestions? The cyst is located on the inside of my right forefinger, smack dab in the middle of it on the middle joint right where it bends--it looks wierd, like I've got some sort of deformity, ugh!
PLEASE email me if you have/have had a ganglion like this before--so far I've found no one with one in the same location. >.
One thing I want to say about surgery is yes, you will get swelling if the hand is not elevated after surgery. Keep hand elevated and wiggle fingers at every opportunity to keep swelling down while arm is bandaged.
Also, I did at least nine months of exercises to get my forearm rotation back to normal - the surgery is the easy part, the post-op exercises is the hard part.
Good luck
I am just trying to recover from having my gangion removed from the same finger; but mine was on same joint but on top rather than under. I am now almost 3 months out of surgery and it's AWFUL. It is swollen, hurts like hell,and red. I've had it checked now 7x and all I get is , "It takes time to heal". Well, I'm sure since they had to go into the bone that it does need time; but I am convinced now that either a stitch was left that didn't dissolve OR a piece of bone is still festering in there. I'm going for another opinion and an x-ray to see what's wrong . If you can avoid surgery, avoid it. I hope you find a good solution.
Thanks
Patsy
*one on my finger next to my thumb (just at base of nail)
*one big one on top of wrist (dorsal)
*one volar (below thumb on wrist)
*three on wrist (where pulse is taken)
Pain is terrible, went to doc a few weeks back, she said nothing could be done... just put a support on it when it's painful!!
Also, Anne - you need a new doctor. Go see a hand specialist or a hand surgeon. No way in heck there's "nothing to be done". That's a terrible doctor. There are other non-surgical treatments available too. Sheesh, you have NO REASON to be suffering.
He also said that he wants to remove the stem where the fluid leaks into the "balloon" to keep it from coming back. (Ive had this one for 5 years.)
My sister had a ganglion on her wrist aspirated a couple of days ago. Her doc gave her the choice between excision or aspiration. She had the aspiration/cortisone injection. She said that it was a big needle and that, that part of it hurt. She'll just have to wait and see if it comes back or not.
Whatever you do, don't smash it. Our bodies can absorb the water out of the gel in the cyst, but we can't absorb the gel itself. If a person smashes it, it might just make the gel spread over a larger area and be even harder to remove. (that's what my doc explained to me).
I'm having an excision on Wednesday. I'm kind of afraid of exacerbation, scar tissue, pain and nerve/tendon damage but I'm just so tired of this thing that I'm taking the risk. (:
forehead that continues to grow in size.
Would a clinic doctor perform such an
operation.
-John
Good luck to all.
Kelsy cabrera.
But overall, the surgery is definitely worth it.
The doctor said he did not know his cost. He told us there would be three costs. 1./ His surgery 2./ The hospital and 3./ The Anesthesiologist.
After seeing my son he directed us to patient finance at the hospital where he practices. The counselor in patient finance would not give us an answer about the cost either and directed us to patient information. At patient information we were told that THEY could not give us the cost of anything because it would require research. So they took my phone number and said they would call after researching the costs.
They called me today (after a week) and said the hospital cost averages about $5000.00. They would not give us the cost for the doctors fee or the anesthesiologist fee--they said it was completely up to the them. They told us the cost of an ultra sound was nearly $500.00 but there would be an additional fee to interpret the results of the ultra sound. Our doctor told us we could get an ultra sound in order to see if the bump is either a cyst or tumor. He examined my sons finger and had an x-ray taken (several) in his office but insisted that it was most likely a tumor.
I would like some knowledge about what my costs will be for this treatment. Am I asking to much?
Have I lost my mind?
It seems absolutely silly that the doctor (with his experience) doesn't know his fee and has no idea about what to expect an anesthesiologists fee might be? Is he that clueless? Is this typical?
Thank you
Thanks.
To the woman whose son has a cyst/tumor, they should know their fee to the dollar amount (except anesthesia cause thats based on how long the surgery is, they normally bill so much for every fifteen or thirty minutes). I got a quote for the surgery center and the doctor two weeks before surgery. Mine was $866 for the center due on surgery day and $425 for the doctor due before pre-op. The anesthesiologist was about $100 for 30 minutes of surgery. About $1400 total. My insurance did not cover cause I had not met my deductible yet. They should be able to diagnose with an x-ray or at most an MRI. Also I might think about getting a second opinion if I were you because a ganglion cyst is a type of benign tumor (and they should know what their fees are). A cyst is a tumor but not all tumors are cysts. My hand surgeon could tell it was a cyst by touching it. He did x-rays to verify cause insurance requires him to. A good specialist should be able to do this.
my remedy is to make a re clay poultice with appl cider vinegar.wrap the area when it dries out make another.
I also drink terramin clay,
may take a while but,just keep doing it,
IT WORKS,hope it helps,
Thanks
Jim H
Wondering if surgery can reconstruct back to normal ?
P.S.
It has moved like all over my wrist. You can e-mail me.
@ Alicia- What is Bikram Yoga? *googles*
@ Evelyn-
"Will I ever be able to use my hand again? What makes these cysts appear? Is it from a repetative motion associated with everyday movements? Is it hereditary?"
It sounds like excessive scar tissue. You may want to try massage and PT to regain full mobility. Can be caused by degeneration in as a result of repetitive movements. I feel that there can be a hereditary predisposition though there really is no evidence to support this.
@ Lydia-The corresponding area in the cartilidge of the joint casing is damaged in some way and leaking the fluid lubricant that causes the cyst. It's possible it could self-resolve or reslove-recur. I know of no homeopathy that has any effect but that's not to say it isn't a possibility.
I've had a dorsal ganglion removed from each wrist and it wasn't any big deal. Outpatient, next to zero recovery. I was maybe 15 the first time. I have also had the fluid aspirated from one in a quick in-office proceedure. That can be a lasting solution if the cyst is rather uncomplicated. It sounds to me that you may be in an area of more extensive progression, however. Have you had it imaged/checked out?
The CMC ganglion was another animal altogether. It extended itself through the carpal tunnel in one direction and throughout the palm to just about to the base of my fingers. An artery was compressed along with the median nerve. The nerves were wrapped around and embedded in the appendages but he managed to section it out in millimeters (give or take) and unwind the fibers without damaging them.
It was so numb it was excrutiating. I slept with a heating pad duct taped around it (shut up). I must have seen 3 diff doctors who all told me it was C.Tunnel and performed X-rays but no Mri and threw a bunch of pain killers at me. After about 6 months a tiny little pea-sized bump appeared mid-palm and there wasn't a surgeon who would touch it. If I remember correctly Dr. C called me the same afternoon I had the Mri. He wanted me in pre-op the next day and the O.R. a day after that.
He told me not to remove the brace or use my hand for any reason. That there was a very real possibility I would lose the hand.
I would urge anyone with a ganglion to have it excised. It isn't always as begnign as it seems. Or as is stated in most literature.
It still gets weak, painful and clumsy though the surgery was successful (8 years back). I had full mobility within 48 hours with no need for PT though he insisted I go in a couple of times. There hasn't been a recurrence so to speak but there was a very tiny mass within the tunnel a year back. Inconsequential.
The shoulder (along the same stop rooted in C6/7) bacame involved and caused the same symptoms add my hand going cold and numb. It was repaired 2 years back but the bouts of pain, loss of fine motor and tingling in the hand didn't resolve.
An EMG showed (shows) damage at the nerve root in C6/7 but that still doesn't account for the problems with my hand. They caught 2 small bilateral lesions at around C3, though,that could be a contributing factor but I'm inclined to believe that the ganglion caused some kind of permanent damage/impairment.
R
Mine popped up one day when I had pain in my foot. It never went away, and I had never injured my foot. I went to a podiatrist but he didn't find anything wrong. Simply told me to wear better shoes which did absolutely nothing. For two years, it only bothered me very occassionally and usually only if I hit the outer edge of my foot against something (wall, etc.).
It got bad this last year, and I could actually see a lump on my foot. Mine was located on the top of my foot between the 4th and 5th toes, right along a nerve. My doctor did x-rays, then decided to inject my foot with cortisone shots. I had three, none of which did anything to help. I finally opted for surgery, and on May 10th, I had the ganglion removed. It hurt much worse then I had expected-I thought it would be an easy procedure. But I guess the ganglion was large, and the surgery was pretty invasive. My foot bruised really bad and for a long time I couldn't move my toes. I had to wear a surgical shoe for 4 weeks. The results came back that I had a blood vessel tangled in the ganglion and damaged muscle as well. It took about six to really heal. It was GREAT having it out but it didn't last long.
I started having pain in the bottom my foot and was forced to go back to the doctor. I received an MRI and it was found that I had a very large soft tissue mass. I just had surgery again (5 months after the last one) on October 20th. This doctor cut my old scar open and made it larger, and removed the mass-turns out it was fibrious scar tissue that was growing so much that it was pressing my bones apart in my foot causing pain. I just think you guys need to know that there is a high chance for the ganglions to come back HOWEVER the scar tissue that I experienced has an even higher chance. Something to consider. This time around has been a lot worse. I had firey pain in my foot, I had to be put on crutches it was so bad and given percocet to control the pain and it's still pretty bad. My foot swelled up so much yesterday (10 days post op) that I could not see my ankle. the bruising is back again, but I expected that.
Anyway, that is a lot of talk to make sure that if you are having ganglion surgery be very aware of scar tissue problems that can arise. I am praying to God this is my last go around with this. I think we are all learning it a a bit of a difficult surgery to recover from.
Best wishes to all of you with pesk ganglions, and here is to hoping nobody has an reoccurrances!!
:)
I finally had a doctor slice it, the fluid removed and the cortosteroid injection. A bandage held it-no stitches. After removel of the bandage, it appeared that the doctor did not remove all of the fluid. Eventually (maybe 2 weeks) the skin returned to normal (flat) and I had a 'pretty' thumb again. Then, it returned.
I tried to drain it again, myself, and couldn't get the needle in-the skin was really tough this time. After a few days, it grew to the point it looked like a huge pimple on top of a small mountain. It got really painful and I couldn't stand it so I bit it. The pressure was released and the pain was gone. Ugly though.
Yesterday I saw a doctor who referred me to a surgeon. After reading all these comments, I am opting NOT to get the surgery at this time. I think I'll ride it out and see if it dissolves like some have said. Good luck to you, and hope this helps.
i hope helped some of you with this information..i have an appoint this upcoming week *anxious*
I have a ganglion cyst in the top of my left foot. It was there for sometime (like 7 years) and it wasn't causing pain or anything. I just couldn't wear (or I thought I couldnt wear cute shoes) since the cyst is right on top. I went to the podiatrist to get it checked out since my sis kept bugging me about it. She was convinced black pus would shoot out. It didn't, lol only the honey like substance oozed out. Doc stuck a needle to numb the area (which is put right into the nerve), waited for about 5-10min to let it all numb up. Doc then poked the lump with another needle and began to squeeze, once this was done the area now looked sunken in. I walked out with no issues. No foot pain just sore from it being pushed on. One month later it was back, did the same thing all over again. Another month went by and I noticed it getting bigger. I am set to have surgery in a few months, wanted to wait until after the holidays. I wish i never began messing with it. I have soreness all the time. Oh before I forget, I went to the nail salon for a pedicure (which i never do because of the cyst) the nail tech was ok but massaged the hell outta my feet and after the light pounding and rubbing the cyst actually went down a little. Needless to say it filled right back up. I am afaid of the surgery as it may not do the job and the whole "bible bump" thing freaks me out. My sister had a big hardcover book (Encyclopedia) and was about to wack the thing but I chicken'd out. good luck to all
I noticed a lump inside my middle finger 2nd joint on my right hand in August of this year, and as of October my whole hand gets numb and I have limited movement in my middle finger along with swelling and tenderness. I have since seen 3 doctor's (my primary and 2 specialists) and they all did the same thing. They sent me for X-rays which doesn't show anything but a mass because its not a bone issue, so my crappy insurance finally approved me for an MRI well my primary gave me the results last night and it's devastating, all I heard was possibly cancer and biopsy before I started crying. I am scheduled to go for my surgical consultation next week. I pray that it is just a ganglion cyst or something less strenuous. I am a little freaked out by some of the stories I have read on here, I hope that everyone come out of their situations great. I will update you all on my results.
Take Care,
*Pastrychef*
I had a ganglion cyst on the back of my left wrist for decades. It got to be slightly smaller than a gumball or those balls that used to live inside your computer mouses. It never hurt, but when I noticed it enlarging laterally a few weeks ago, i had it aspirated. (It was so noticeable, my boss asked about it once) Came right back 36 hours later. So I scheduled the surgery with a very impressive hand specialist in NYC. I had the surgery Friday morning (today is Sunday). I was knocked out and woke up with a "dead arm", wrapped up. Surprisingly, there was hardly any pain, though I took a percoset at night just in case. The numbness sucked and kept me from doing things, but that wore off by the next morning, and now it's basically like having a cast -- my fingers are free to type and pick up light things. Just my wrist is immobilized. My only concern is they wanted me to keep it elevated and i wonder how vigilant i should be about that. I sleep with a big spongy thing that keeps it raised, and keep it up most of the time when I'm not using it (the sling makes it impossible to use the hand), but maybe that part isn't as important anymore. The doctor wants to see me in two weeks, when he'll take off the bandage, but maybe I can cut that by a few days. Typing is crucial to my work.
Of course if it is affecting your quality of life, or causing pain by pressing on a nerve, then by all means do what you need to do.
I have one on my left wrist that over a few weeks grows to the size of a cherry tomato, then it slowly goes away over a few months. It has recently come back for a week, and then by gentle massaging it "deflated" under the skin and is barely detectable now.
Mine does not cause pain, so I don't need to go to a barber to have it poked or cut.
If you have a ganglionic cyst, your should leave it alone unless it begins to become painful or impedes motion of a joint or function of a tendon. Let a physician properly treat it,
"backyard surgery" often has very unexpected and potentially very bad consequences associated with it!
I'm seeing a hand surgeon in 2 weeks so we'll see what he says. I did have the first one aspirated and it was back within 24 hours, so they went ahead with surgery. I'm expecting they'll probably try aspirating it again before considering excision. The MRI scan also confirmed something that I'd wondered about having tried to feel where it was stemming from - I have a septated ganglion, which means it has more than one chamber. It's a bit of a nuisance, but I do at least know what I'm in for this time - I'm still hoping to go ahead with surgery in spite of knowing how uncomfortable it is recovering from it!
I've been dealing with a ganglion cyst for 3-4 years now. I've had it drained 5 times and it keeps coming back. Now I am getting arthritis too. My orthopedic officially recommended surgery last week. I have mixed feelings about this. While having the cyst is painful and now having arthritis is even more painful, I am nervous for surgery. What is the recovery time like. I type ALL day at work. How long could I be out. Could the cyst still come back after surgery?
Thanks!
thanks
It went all the way down for one week after that. Now it's back twice the size it were before surgery. I've done some research and found that there are compression gloves to be worn after surgery for several weeks. I'm going to the doctor tomorrow to have her remove it completely this time and order the gloves for post surgery treatment.
Will I need it surgically removed? Do you need it removed? Obviously an aspiration is impossible for me considering it's location.
My cyst I'm guessing is from trauma from my soccer incident.
Thank you
Or anyone with an painful occult cyst in wrist?
R/
S
I had a ganglion cyst on my L wrist top. It wasn't painless but my doc. suggested me to get it aspirated. I did it on 28th dec.2013 and he tied a tight pink bandage on my wrist to restrict its movement. However he suggested me to remove it at the end of the day and also advise to continue working as usual. I did exactly the same. Let me tell you, here, when my doc. injected steroid into the cyst, it was harsh pain (a mix of needles like sensation + burning + aching). I dropped my guests from 3rd floor to Parking with not-that-heavy luggage in the same hand. While removing the bandage in the night, I saw that my hand was swollen and was paining.
The swelling continued to be there till next 4-5 days. Now it has been more than 10 days, still my wrist is aching. Sometimes little finger pains the other time, thumb and index fingers. Sometimes even the carpal bone hurts as if my hand has got a sudden massive jerk in a vehicle. What is this? Does anyone sailing in the same boat?
Thanks, Sydney
Can I take do anything beside taking pain killers thank u
I too, have a ganglion cyst on the sole of my foot about the size of a small grape and it hurts when walking, burns at times.
I'm considering an appt with a Podiatrist for treatment...but also read where suggested treatments are to apply a salicylic adic patch to the area. I have used such a patch before on a wart...which made the area sore and had some burning. Has anyone else had this type of treatment and wondering too, how it was? Please email me!!
Before surgery, i did not have a problem with the cyst(i didn't even know what it was for about a year), until it got to the pint where my eft hand was always tingling and it got numb. I play many instruments in my band, and i was unable to play my instruments because i couldn't move my fingers.
I went to see two specialists and the second one said i was going to have surgery because it was affecting the nerves in my left hand.
Now, six months later, there is another bump on the surgery site. It feels soft and it is becoming painful(however, there isnt any numbness in my hand this time). I noticed it formed there about 11 days ago, and i dont know if it just because of the surgery. I hear that it is possible for another cyst to for even after excision. But im worried to let ym family know, because if it is another cyst and i need surgery again, well. We dont have the money for it.
Should I get this checked out? or should i just wait it out?
what symptoms of rsd did you have? How did the doctors diagnos it? Was it because of you weak wrists?
Also has anyone donated blood and got a ganglion cyst after?