Splenectomy
Definition
A splenectomy is the total or partial surgical removal of the spleen, an organ that is part of the lymphatic system.
Purpose
The human spleen is a dark purple bean-shaped organ located in the upper left side of the abdomen just behind the bottom of the rib cage. In adults, the spleen is about 4.8 X 2.8 X 1.6 in (12 X 7 X 4 cm) in size, and weighs about 4–5 oz (113–14 g). The spleen plays a role in the immune system of the body. It also filters foreign substances from the blood and removes worn-out blood cells. The spleen regulates blood flow to the liver and sometimes stores blood cells—a function known as sequestration. In healthy adults, about 30% of blood platelets are sequestered in the spleen.
Splenectomies are performed for a variety of different reasons and with different degrees of urgency. Most splenectomies are done after a patient has been diagnosed with hypersplenism. Hypersplenism is not a specific disease but a syndrome (group or cluster of symptoms)
Splenectomy always required
There are two diseases for which a splenectomy is the only treatment—primary cancers of the spleen and a blood disorder called hereditary spherocytosis (HS). In HS, the absence of a specific protein in the red blood cell membrane leads to the formation of relatively fragile cells that are easily damaged when they pass through the spleen. The cell destruction does not occur elsewhere in the body and ends when the spleen is removed. HS can appear at any age, even in newborns, although doctors prefer to put off removing the spleen until the child is five to six years old.
Splenectomy usually required
There are some disorders for which a splenectomy is usually recommended. They include:
- Immune (idiopathic) thrombocytopenic purpura (ITP). ITP is a disease in which platelets are destroyed by antibodies in the body's immune system. A splenectomy is the definitive treatment for this disease and is effective in about 70% of cases of chronic ITP.
- Trauma. The spleen can be ruptured by blunt as well as penetrating injuries to the chest or abdomen. Car accidents are the most common cause of blunt traumatic injury to the spleen.
- Abscesses. Abscesses of the spleen are relatively uncommon but have a high mortality rate.
- Rupture of the splenic artery. This artery sometimes ruptures as a complication of pregnancy.
- Hereditary elliptocytosis. This is a relatively rare disorder. It is similar to HS in that it is characterized by red blood cells with defective membranes that are destroyed by the spleen.
Splenectomy sometimes required
Other disorders may or may not necessitate a splenectomy. These include:
- Hodgkin's disease, a serious form of cancer that causes the lymph nodes to enlarge. A splenectomy is often performed in order to find out how far the disease has progressed.
- Autoimmune hemolytic disorders. These disorders may appear in patients of any age but are most common in adults over 50. The red blood cells are destroyed by antibodies produced by the patient's own body (autoantibodies).
- Myelofibrosis. Myelofibrosis is a disorder in which bone marrow is replaced by fibrous tissue. It produces severe and painful splenomegaly. A splenectomy does not cure myelofibrosis but may be performed to relieve pain caused by the swelling of the spleen.
- Thalassemia. Thalassemia is a hereditary form of anemia that is most common in people of Mediterranean origin. A splenectomy is sometimes performed if the patient's spleen has become painfully enlarged.
Demographics
In the United States, splenomegaly affects as many as 30% of full-term newborns and about 10% of healthy children. Approximately 3% of healthy first-year college students also have spleens that are large enough to be felt when a doctor palpates the abdomen. Some specific causes of splenomegaly are more common in certain racial or ethnic groups. For example, splenomegaly is a common complication of sickle cell disease in patients of African or Mediterranean ancestry. In other parts of the world, splenomegaly is frequently caused by malaria, schistosomiasis, and other infections in areas where these diseases are endemic.
Hereditary spherocytosis (HS) is a disorder is most common in people of northern European descent but has been found in all races. A family history of HS increases the risk of developing this disorder.
Immune thrombocytopenic purpura (ITP) is much more common in children, with male and female children being equally afflicted. Female predominance begins at puberty and continues in adult patients. Overall, 70% of patients with ITP are female; 72% of women diagnosed with ITP are over 40 years old.
Description
Complete splenectomy
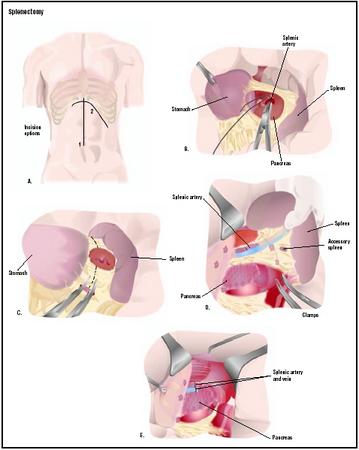
REMOVAL OF ENLARGED SPLEEN. A splenectomy is performed under general anesthesia. The most common technique is used to remove greatly enlarged spleens. After the surgeon makes a cut (incision) in the abdomen, the artery to the spleen is tied to prevent blood loss and reduce the size of the spleen. Tying the splenic artery also keeps the spleen from further sequestration of blood cells. The surgeon detaches the ligaments holding the spleen in place and removes the organ. In many cases, tissue samples will be sent to a laboratory for analysis.
REMOVAL OF RUPTURED SPLEEN. When the spleen has been ruptured by trauma, the surgeon approaches the organ from its underside and ties the splenic artery before removing the ruptured organ.
Partial splenectomy
In some cases, the surgeon removes only part of the spleen. This procedure is considered by some to be a useful compromise that reduces pain caused by an enlarged spleen while leaving the patient less vulnerable to infection.
Laparoscopic splenectomy
Laparoscopic splenectomy, or removal of the spleen through several small incisions, has been performed more frequently in recent years. Laparoscopic surgery, which is sometimes called keyhole surgery, is done with smaller surgical instruments inserted through very short incisions, with the assistance of a tiny camera and video monitor. Laparoscopic procedures reduce the length of hospital stay, the level of postoperative pain, and the risk of infection. They also leave smaller scars.
As of 2003, however, a laparoscopic procedure is contraindicated if the patient's spleen is greatly enlarged. Most surgeons will not remove a spleen longer than 20 cm (as measured by a CT scan) by this method.
Diagnosis/Preparation
The most important part of a medical assessment in disorders of the spleen is the measurement of splenomegaly. The normal spleen cannot be felt when the doctor palpates the patient's abdomen. A spleen that is large enough to be felt indicates splenomegaly. In some cases, the doctor will hear a dull sound when he or she thumps (percusses) the patient's abdomen near the ribs on the left side. Imaging studies that can be used to confirm splenomegaly include ultrasound tests, technetium-99m sulfur colloid imaging, and CT scans . The rate of platelet or red blood cell destruction by the spleen can also be measured by tagging blood cells with radioactive chromium or platelets with radioactive indium.
Preoperative preparation for a splenectomy procedure usually includes:
- Correction of abnormalities of blood clotting and the number of red blood cells.
- Treatment of any infections.
- Control of immune reactions. Patients are usually given protective vaccinations about a month before surgery. The most common vaccines used are Pneumovax or Pnu-Imune 23 (against pneumococcal infections) and Menomune-A/C/Y/W-135 (against meningococcal infections).
Aftercare
Immediately following surgery, patients are given instructions for incision care and medications intended to prevent infection. Blood transfusions may be indicated for some patients to replace defective blood cells. The most important part of aftercare, however, is long-term caution regarding vulnerability to infection. Patients are asked to see their doctor at once if they have a fever or any other sign of infection, and to avoid travel to areas where exposure to malaria or similar diseases is likely. Children with splenectomies may be kept on antibiotic therapy until they are 16 years old. All patients can be given a booster dose of pneumococcal vaccine five to 10 years after undergoing a splenectomy.
Risks
The main risk of a splenectomy procedure is overwhelming bacterial infection, or postsplenectomy sepsis. This condition results from the body's decreased ability to clear bacteria from the blood, and lowered levels of a protein in blood plasma that helps to fight viruses (immunoglobulin M). The risk of dying from infection after undergoing a splenectomy is highest in children, especially in the first two years after surgery. The risk of postsplenectomy sepsis can be reduced by vaccinations before the operation. Some doctors also recommend a two-year course of penicillin following splenectomy, or long-term treatment with ampicillin.
Other risks associated with the procedure include inflammation of the pancreas and collapse of the lungs. In some cases, a splenectomy does not address the underlying causes of splenomegaly or other conditions. Excessive bleeding after the operation is an additional possible complication, particularly for patients with ITP. Infection of the incision immediately following surgery may also occur.
Normal results
Results depend on the reason for the operation. In blood disorders, the splenectomy will remove the cause of the blood cell destruction. Normal results for patients with an enlarged spleen are relief of pain and the complications of splenomegaly. It is not always possible, however, to predict which patients will respond well or to what degree.
Recovery from the operation itself is fairly rapid. Hospitalization is usually less than a week (one to two days for laparoscopic splenectomy), and complete healing usually occurs within four to six weeks. Patients are encouraged to return to such normal activities as showering, driving, climbing stairs, light lifting and work as soon as they feel comfortable. Some patients may return to work in a few days while others prefer to rest at home a little longer.
Morbidity and mortality rates
The outcome of the procedure varies with the underlying disease or the extent of other injuries. Rates of complete recovery from the surgery itself are excellent, in the absence of other severe injuries or medical problems.
Splenectomy for HS patients is usually delayed in children until the age of five to prevent unnecessary infections; reported outcomes are very good.
Studies of patients with ITP show that 80%–90% of children achieve spontaneous and complete remission in two to eight weeks. A small percentage develop chronic or persistent ITP, but 61% show complete remission by 15 years. No deaths in patients older than 15 have been attributed to ITP.
Alternatives
As of 2003 there are no medical alternatives to removing the spleen.
Splenic embolization is a surgical alternative to splenectomy that is used in some patients who are poor candidates for surgery. Embolization involves plugging or blocking the splenic artery with synthetic substances to shrink the size of the spleen. The substances that are injected during this procedure include polyvinyl alcohol foam, polystyrene, and silicone.
See also Gastroduodenostomy ; Pancreatectomy .
Resources
books
Hiatt, J. R., Phillips, E. H., and L. Morgenstern, eds. Surgical Diseases of the Spleen . New York: Springer Verlag, 1997.
Wilkins, B. S., and D. H. Wright. Illustrated Pathology of the Spleen . Cambridge, UK: Cambridge University Press, 2000.
periodicals
Al-Salem A. H., and Z. Nasserulla. "Splenectomy for Children with Thalassemia." Internal Surgery 87 (October-December 2002): 269-273.
Duperier, T., J. Felsherm, and F. Brody. "Laparoscopic Splenectomy for Evans Syndrome." Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 13 (February 2003): 45-47.
Schwartz, J., M. D. Leber, S. Gillis, et al. "Long-Term Follow-Up After Splenectomy Performed for Immune Thrombocytopenic Purpura (ITP)." American Journal of Hematology 72 (February 2003): 94-98.
Svarch, E., I. Nordet, J. Valdes, et al. "Partial Splenectomy in Children with Sickle Cell Disease." Haematologica 88 (February 2003): 281-287.
organizations
American College of Gastroenterology. 4900 B South 31st St., Arlington, VA 22206. (703) 820-7400. http://www.acg.gi.org
American Gastroenterological Association (AGA). 4930 Del Ray Avenue, Bethesda, MD 20814. (301) 654-2055. http://www.gastro.org
National Cancer Institute (NCI). NCI Public Inquiries Office, Suite 3036A, 6116 Executive Boulevard, MSC8322 Bethesda, MD 20892-8322. (800) 422-6237. http://www.cancer.gov
other
The Body Homepage. Spleen Cancer . http://www.thebody.com/Forums/AIDS/Cancer/Archive/othertypes/Q141422.html .
Yoursurgery.com . Splenectomy . http://www.yoursurgery.com/ProcedureDetails.cfm?BR=1&Proc=46 .
Teresa Norris, RN Monique Laberge, Ph. D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
A splenectomy is performed by a surgeon trained in gastroenterology, the branch of medicine that deals with the diseases of the digestive tract. An anesthesiologist is responsible for administering anesthesia and the operation is performed in a hospital setting.
QUESTIONS TO ASK THE DOCTOR
- What happens on the day of surgery?
- What type of anesthesia will be used?
- How long will it take to recover from the surgery?
- When can I expect to return to work and resume normal activities?
- What are the risks associated with a splenectomy?
- How many splenectomies do you perform in a year?
- Will I have a large scar?
I went into college to study Nursing( that's on 2007 to help manage my condition. I'd be graduating this year by November. I am managing myself better by now but I still get sick every now and then especially when I get involved in theatre work(s).
Asplenia is a big issue but most people don't know.
Please if you are taking pills for complications and all, check with your doctor and do research on your own before you take them because EVERY DRUG is a POTENTIAL POISON.
I went into college to study Nursing( that's on 2007 to help manage my condition. I'd be graduating this year by November. I am managing myself better by now but I still get sick every now and then especially when I get involved in theatre work(s).
Asplenia is a big issue but most people don't know.
Please if you are taking pills for complications and all, check with your doctor and do research on your own before you take them because EVERY DRUG is a POTENTIAL POISON.
I want to ask some questions what happen after surgery or what are we expected will happen after the surgery and what shoul we do if we got complication.
Thanks
ARE THERE ANY ABSOLUTE CONTRAINDICATIONS FOR THE SAME ?
Can my kidney be crawling into where my spleen used to be? Can doctors tell if my organs are moving around and if they are, can they do anything about it? Its starting to worry me a lot. I think exercise makes it worse.
The question I have now is should I still be having bad stomache pains as well as a terrible headache ? Chest and neck pain and absolutely no appetite.
I dont see the doctor for 4 more days to have the staples removed but wondering if i should try to get in sooner because of the above.
since the procedure. I take my pain pills every 8 hours to prevent
the pain from getting worse. My procedure went well my platelets
increased from 29,000 to over 200,000 and and my white blood cells
Increased to normal rate within 2 to 3 days. The doctor only stopped
the blood to half of my spleen. But it hurts what are your thoughts?
Thank you
Jim Monserrate
Please respond thanks
One is tempted to avoid contact with others to avoid infection but you have to live.
I am interested to know if there are any useful strategies - ie foods drugs etc that anyone has found beneficial post splenectomy? Daily antibiotics are recommended in the UK but I find they make me feel nauseous.
A sister on intensive care warned me that from getting a sore throat to deceased can be as quick as 48 hours so its very important to keep your antibiotics at the ready. Also get good advice before travelling as some bugs are resistant to penicillin. Another frustration is the lack of understanding and consideration for this disability and the frustration of explaining how you are incapacitated by a cold or tummy bug that everyone else shrugs off in a few days.
Has enlarged and giving pain , verified thru MRI & cat scans -- I've put off approving spleen
Removal due to impending infections and future complications to my already compromised lymph system by NHL .ps: ( radiation & surgery only -have not done any chemo yet)
What is the estimate quantity of life after a spleen is removed ? Thanks
I had ITP in 1985. After massive daily doses of prednisone & two different chemo drugs (cytoxin & vincristin) I had a spleenectomy. I lead a perfectly normal life but if I get sick (flu, cold, etc) it takes a long time to recover. I get yearly flu shot & pneumacocal (not sure of spelling) shots & any other necessary innoculation.
After multiple spleen scans being performed before my surgery you would have thought my doctor would have realized my spleen was not where it should be. The first thing I remember after waking up is my doctor telling me "I cut you extra big." My incision starts below my left breast at a downward angle for about 5 inches. Then it continues straight down my belly almost to my hysterectomy bikini scar. It looks like a slightly distorted "L" on my chest. Since my last name starts with "L" I joke that I am marked with my initial like Lavern (Lavern & Shirley TV show) wore an "L" on all her clothes.
sets in. Mt life is basically nil. I am or was a very healthy young 72. I spend most of my life in a recliner no appetite high white and platelet counts.After going through this week after week, I became very depressed. No MD seems to have an inkling what the problem is. I am really concerned the docs will start or haven't already see me as a flake. I do not know where to turn, I have even thought there is no purpose to this SUFFERING.Infectious disease found their studies neg, as did my oncologist. What type of physician can I appeal to. I think the lymphoma ia in remission, my gut tells me its something gastric related to the huge spleen and rearrangement of all my abdominal and chest cavities. Does anyone share any of this. I want to live but passing on seems like a welcome reprieve. I have also been RX'D for a mac lung disease--and 9 months of horrible antibiotics, also for a staph infection in lungs--both after the thorocotomy
You can live just fine after a splenectomy; you just have to get vaccines and follow a few extra precautions. You'll probably catch a few more colds and get bronchitis a bit more than before, but that's about it. I have not heard one word from my medical team about not being allowed to drink, eat fast food, etc. If you are being given that advice, it's not coming from a doctor or you are misunderstanding what you are being told.
Be glad you're just having a splenectomy and move on with your life in a calm and mature fashion. You could have had pancreatic cancer like me, and had a distal pancreatectomy, a splenectomy, a pancreatic fistula, a staph infection, a stomach perforation, a broken JP Drain, and urine retention requiring self-cathing and a Foley. And *I'M* still walking around smiling, working, and not feeling sorry for myself ... and this was about 5 months ago.
If you find you can't calm down about a simple thing like a splenectomy, and it makes you want to "kill yourself", my advice is to call emergency services or see a psychiatrist as you obviously need meds and therapy of some kind.
Best of luck.
And when it is necessary to to splenectomy at what enlargement
Myaunt is suffering from swelling in spleen and she got hyper fever sometimes and some times she not able to control urination and do at there plz suggest me correct diagnosis thank u
I was chronic with ITP for 2years after the splenectomy, went into a 4 year remission. In that window of time I had two children, then ITP came back when my middle child was 4 months old.
I was chronic for 7 years. I eventually was put on IViG treatments and I became pregnant with my last child. I went into remission that has lasted so far 22 years.
Did the pregnancy help the splenectomy due it's job? Who knows.
I have since lived a full and active life with out a spleen. I usually do not have problems with infection. My platelet count sometimes is high but it always corrects itself. I have been on an aspirin the last couple of years tab for a-fib, so that has helped with the counts.
This is my experience. Not everyone is the same, but I can only give what mine is.
Cheers!