Nephrolithotomy, percutaneous
Definition
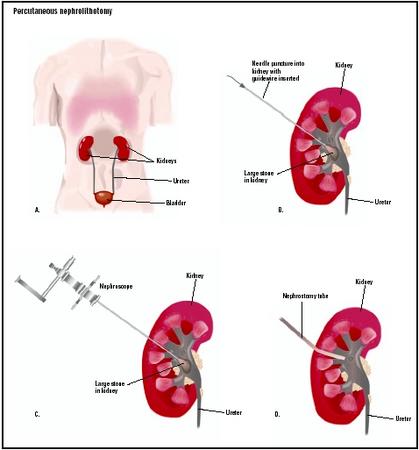
Percutaneous nephrolithotomy, or PCNL, is a procedure for removing medium-sized or larger renal calculi (kidney stones) from the patient's urinary tract by means of an nephroscope passed into the kidney through a track created in the patient's back. PCNL was first performed in Sweden in 1973 as a less invasive alternative to open surgery on the kidneys. The term "percutaneous" means that the procedure is done through the skin. Nephrolithotomy is a term formed from two Greek words that mean "kidney" and "removing stones by cutting."
Purpose
The purpose of PCNL is the removal of renal calculi in order to relieve pain, bleeding into or obstruction of the urinary tract, and/or urinary tract infections resulting from blockages. Kidney stones range in size from microscopic groups of crystals to objects as large as golf balls. Most calculi, however, pass through the urinary tract without causing problems.
Renal calculi are formed when the urine becomes supersaturated (overloaded) with mineral compounds that can form stones. This supersaturation may occur because the patient has low urinary output, is excreting too much salt, or has very acid urine. Urolithiasis is the medical term for the formation of kidney stones; the word is also sometimes used to refer to disease conditions associated with kidney stones.
There are several different types of kidney stones, in terms of chemical composition:
- Calcium oxalate calculi. About 80% of calculi found in patients in the United States are formed from calcium combined with oxalate, which is a salt formed from oxalic acid. Some foods, such as rhubarb and spinach, are high in oxalic acid. Oxalic acid is also formed in the body when vitamin C is broken down. Oxalic acid is ordinarily excreted through the urine but may be absorbed in large amounts due to chronic pancreatic disease or surgery involving the small intestine.
- Uric acid calculi. These stones develop from crystals of uric acid that form in highly acidic urine. Uric acid calculi account for about 5% of kidney stones. In addition, some kidney stones are a combination of calcium oxalate and uric acid crystals.
- Cystine calculi. Cystine calculi represent about 2% of kidney stones. Cystine is an amino acid found in proteins that may form hexagonal crystals in the urine when it is excreted in excessive amounts. Kidney stones made of cystine indicate that the patient has cystinuria, a hereditary condition in which the kidneys do not reabsorb this amino acid.
- Struvite calculi. Struvite is a hard crystalline form of magnesium aluminum phosphate. Kidney stones made of this substance are formed in patients with urinary tract infections caused by certain types of bacteria. Struvite calculi are also known as infection calculi for this reason.
- Staghorn calculi. Staghorn calculi are large branched calculi composed of struvite. They are often discussed separately because their size and shape complicate their removal from the urinary tract.
Some people are more likely than others to develop renal calculi. Risk factors for kidney stones include:
- Male sex.
- Family history. Having a first-degree relative with urolithiasis increases a person's risk of developing kidney stones.
- Age over 30.
- Diet. People whose diet is high in protein or who eat foods rich in oxalate are more likely to develop kidney stones.
- Dehydration. People who do not drink enough fluid each day to replace what is lost through perspiration and excretion produce very concentrated urine. It is easier for crystals to form in concentrated than in dilute urine, and to grow into kidney stones.
- Metabolic disorders affecting the body's excretion of salt or its absorption of calcium or oxalate. Most cases of urolithiasis in children are related to metabolic disorders.
- Intestinal bypass surgery and ostomies. People who have had these surgical procedures lose larger than average amounts of water from the digestive tract.
Demographics
Calculi in the urinary tract are common in the general United States population. Between seven and 10 in every 1,000 adults are hospitalized each year for treatment of urolithiasis; in addition, kidney stones are found in about 1% of bodies at autopsy. An estimated 10% of the population will suffer from kidney stones at some point in life. For reasons that are not yet known, the percentage of people with kidney stones has been rising in North America since 1980. In addition, the gender ratio is changing as more women are developing kidney stones. In 1980, the male:female ratio was 4:1; as of 2002, it was 3:1. Although more men develop renal calculi in general than women, more women develop infection calculi than men.
In terms of age groups, most people with urolithiasis are between the ages of 20 and 40; kidney stones are rare in children. A person who develops one kidney stone has a 50% chance of developing another.
With regard to race, Caucasians are more likely to develop kidney stones than African Americans.
Description
Standard PCNL
A standard percutaneous nephrolithotomy is performed under general anesthesia and usually takes about three to four hours to complete. After the patient has been anesthetized, the surgeon makes a small incision, about 0.5 in (1.3 cm) in length in the patient's back on the side overlying the affected kidney. The surgeon then creates a track from the skin surface into the kidney and enlarges the track using a series of Teflon dilators or bougies. A sheath is passed over the last dilator to hold the track open.
After the track has been enlarged, the surgeon inserts a nephroscope, which is an instrument with a fiberoptic light source and two additional channels for viewing the inside of the kidney and irrigating (washing out) the area. The surgeon may use a device with a basket on the end to grasp and remove smaller kidney stones directly. Larger stones are broken up with an ultrasonic or electrohydraulic probe, or a holmium laser lithotriptor. The holmium laser has the advantage of being usable on all types of calculi.
A catheter is placed to drain the urinary system through the bladder and a nephrostomy tube is placed in the incision in the back to carry fluid from the kidney into a drainage bag. The catheter is removed after 24 hours. The nephrostomy tube is usually removed while the patient is still in the hospital but may be left in after the patient is discharged.
Mini-percutaneous nephrolithotomy
A newer form of PCNL is called mini-percutaneous nephrolithotomy (MPCNL) because it is performed with a miniaturized nephroscope. MPCNL has been found to be 99% effective in removing calculi between 0.4 and 1 in (1 and 2.5 cm) in size. Although it cannot be used for larger kidney stones, MPCNL has the advantage of fewer complications, a shorter operating time (about one and a half hours), and a shorter recovery time for the patient.
Diagnosis/Preparation
Diagnosis
Kidney stones may be discovered during a routine x ray study of the patient's abdomen. These stones, which would ordinarily pass through the urinary tract unnoticed, are sometimes referred to as silent stones. In most cases, however, the patient seeks medical help for sudden intense pain in the lower back, usually on the side of the affected kidney. The pain is caused by the movement of the stone in the urinary tract as it irritates the tissues or blocks the passage of urine. If the stone moves further downward into the ureter (the tube that carries urine from the kidney to the bladder), pain may spread to the abdomen and groin area. The patient may also have nausea and vomiting, blood in the urine, pain on urination, or a need to urinate frequently. If the stone is associated with a UTI, the patient may also have chills and fever. The doctor will order both laboratory studies and imaging tests in order to rule out such other possible causes of the patient's symptoms as appendicitis, pancreatitis, peptic ulcer, and dissecting aneurysm.
The imaging studies most commonly performed are x ray and ultrasound. Pure uric acid and cystine calculi, however, do not show up well on a standard x ray, so the doctor may also order an intravenous pyelogram, or IVP. In an IVP, the radiologist injects a radioactive contrast material into a vein in the patient's arm, and records its passage through the urinary system in a series of x ray images. Blood and urine samples will be taken to test for indications of a urinary tract infection. If the patient passes the kidney stone, it is saved and sent to a laboratory for analysis.
Preparation
Most hospitals require patients to have the following tests before a PCNL: a complete physical examination ; complete blood count ; an electrocardiogram (EKG); a comprehensive set of metabolic tests; a urine test; and tests that measure the speed of blood clotting.
Aspirin and arthritis medications should be discontinued seven to 10 days before a PCNL because they thin the blood and affect clotting time. Some surgeons ask patients to take a laxative the day before surgery to minimize the risk of constipation during the first few days of recovery.
The patient is asked to drink only clear fluids (chicken or beef broth, clear fruit juices, or water) for 24 hours prior to surgery, with nothing by mouth after midnight before the procedure.
Aftercare
A standard PCNL usually requires hospitalization for five to six days after the procedure. The urologist may order additional imaging studies to determine whether any fragments of stones are still present. These can be removed with a nephroscope if necessary. The nephrostomy tube is then removed and the incision covered with a bandage. The patient will be given instructions for changing the bandage at home.
The patient is given fluids intravenously for one to two days after surgery. Later, he or she is encouraged to drink large quantities of fluid in order to produce about 2 qt (1.2 l) of urine per day. Some blood in the urine is normal for several days after PCNL. Blood and urine samples may be taken for laboratory analysis of specific risk factors for calculus formation.
Risks
There are a number of risks associated with PCNL:
- Inability to make a large enough track to insert the nephroscope. In this case, the procedure will be converted to open kidney surgery.
- Bleeding. Bleeding may result from injury to blood vessels within the kidney as well as from blood vessels in the area of the incision.
- Infection.
- Fever. Running a slight temperature (101.5°F; 38.5°C) is common for one or two days after the procedure. A high fever or a fever lasting longer than two days may indicate infection, however, and should be reported to the doctor at once.
- Fluid accumulation in the area around the incision. This complication usually results from irrigation of the affected area of the kidney during the procedure.
- Formation of an arteriovenous fistula . An arteriovenous fistula is a connection between an artery and a vein in which blood flows directly from the artery into the vein.
- Need for retreatment. In general, PCNL has a higher success rate of stone removal than extracorporeal shock wave lithotripsy (ESWL), which is described below. PCNL is considered particularly effective for removing stones larger than 1 in (0.5 cm); staghorn calculi; and stones that have remained in the body longer than four weeks. Retreatment is occasionally necessary, however, in cases involving very large stones.
- Injury to surrounding organs. In rare cases, PCNL has resulted in damage to the spleen, liver, lung, pancreas, or gallbladder.
Normal results
PCNL has a high rate of success for stone removal, over 98% for stones that remain in the kidney and 88% for stones that pass into the ureter.
Morbidity and mortality rates
Standard PCNL has a higher rate of complications than extracorporeal shock wave lithotripsy; however, it is more successful in removing calculi. The overall rate of complications following PCNL is reported as 5.6% in one recent study and 6.5% in a second article. About 20% of patients scheduled for PCNL require a blood transfusion during the procedure, with 2.8% needing treatment for bleeding after the procedure. The rate of fistula formation is about 2.5%.
Alternatives
Patients with kidney stones may be treated with one or more of the following procedures in addition to PCNL, depending on the size of their renal calculi and possible complications. One frequently used combination, known as sandwich therapy, is extracorporeal shock wave lithotripsy for smaller stones followed by PCNL to remove larger calculi.
Conservative approaches
Conservative forms of treatment include the following:
- Watchful waiting.
- Hydration. Increasing the patient's fluid intake (to seven or more glasses of fluid each day) is a major component of treatment intended to prevent the formation of kidney stones. At least half of the fluid should be water.
- Dietary modification. Depending on the type of stone that has formed, the patient may benefit from eating less animal protein, avoiding vegetables with high oxalate content, cutting down on table salt and vitamin C intake, etc.
- Medications. Patients who tend to form uric acid stones may be given allopurinol, which decreases the formation of uric acid; those who form calcium oxalate stones may be given thiazide diuretics ; and those who develop infection stones can be treated with oral antibiotics.
Open surgery
Open surgery is the most invasive form of treatment for urolithiasis. As of 2003, it is performed primarily to remove very large and complex staghorn calculi or extremely hard stones that cannot be broken down by lithotripsy. Other indications for open surgery are extreme obesity, an anatomically abnormal kidney, or an infected and nonfunctioning kidney requiring complete removal. Patients are usually hospitalized for a week after open kidney surgery and take about six weeks to recover at home.
Extracorporeal shock wave lithotripsy (ESWL)
ESWL is a noninvasive procedure that was developed in the 1980s as a less invasive alternative to PCNL. It is presently used more often than PCNL to treat smaller renal calculi. In ESWL, the patient is given a local anesthetic and placed in a water bath or on a soft cushion while shock waves are transmitted through the tissues of the back to the stones inside the kidney. The shock waves cause the calculi to break up into smaller pieces that can be passed easily in the urine.
Although patients need less time to recuperate from ESWL, it has several disadvantages. It has lower success rates (50–90%) than PCNL. Moreover, it cannot be used to treat cystine calculi or calculi larger than 1.2 in (3 cm). An additional concern with shock wave lithotripsy is its safety in treating small or anatomically abnormal kidneys; it has been reported to cause temporary damage to kidney tubules in smaller-than-average kidneys.
Ureteroscopy
Ureteroscopy refers to removal of calculi that have moved downward into the ureter with the help of a special instrument. A ureteroscope is a small fiberoptic endoscope that can be passed through the patient's urethra and bladder into the ureter. The ureteroscope allows the surgeon to locate and remove stones in the lower urinary tract without the need for an incision.
Complementary and alternative (CAM) approaches
Vegetarian and other low-protein diets have been found helpful in preventing kidney stone formation. In addition, recent ethnobotanical studies of ammi visnaga (toothpick weed), a plant belonging to the parsley family, and Phyllanthus niruri , a traditional Brazilian folk remedy for kidney stones, indicate that extracts from these plants are effective in increasing urinary output and inhibiting the development of calcium oxalate calculi.
See also Urologic surgery .
Resources
books
Pelletier, Kenneth R., MD. "CAM Therapies for Specific Conditions: Kidney Stones." In The Best Alternative Medicine. New York: Simon & Schuster, 2002.
"Urinary Calculi." In The Merck Manual of Diagnosis and Therapy , edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
periodicals
Battino, B. S., W. DeFoor, F. Coe, et al. "Metabolic Evaluation of Children with Urolithiasis: Are Adult References for Supersaturation Appropriate?" Journal of Urology 168 (December 2002): 2568–2571.
Chan, D. Y., and T. W. Jarrett. "Mini-Percutaneous Nephrolithotomy." Journal of Endourology 14 (April 2000): 269–272.
Freitas, A. M., N. Schor, and M. A. Boim. "The Effect of Phyllanthus niruri on Urinary Inhibitors of Calcium Oxalate Crystallization and Other Factors Associated with Renal Stone Formation." BJU International 89 (June 2002): 829–834.
Jin, Chua Wei, and Chin Chong Min. "Management of Staghorn Calculus." Medical Progress (February 2003): 1–6.
Khan, Z. A., A. M. Assiri, H. M. Al-Afghani, and T. M. Maghrabi. "Inhibition of Oxalate Nephrolithiasis with Ammi Visnaga (Al-Khillah)." International Urology and Nephrology 33 (2001): 605–608.
Kim, S. C., R. L. Kuo, and J. E. Lingeman. "Percutaneous Nephrolithotomy: An Update." Current Opinion in Urology 13 (May 2003): 235–241.
Kinn, A. C., I. Fernstrom, B. Johansson, and H. Ohlsen. "Percutaneous Nephrolithotomy—The Birth of a New Technique." Scandinavian Journal of Urology and Nephrology Supplement 138 (1991): 11–14.
Lahme, S., K. H. Bichler, W. L. Strohmaier, and T. Gotz. "Minimally Invasive PCNL in Patients with Renal Pelvic and Calyceal Stones." European Urology 40 (December 2001): 619–624.
Parsons, J. K., T. W. Jarrett, V. Lancini, and L. R. Kavoussi. "Infundibular Stenosis After Percutaneous Nephrolithotomy." Journal of Urology 167 (January 2002): 35–38.
Ugras, M., A. Gunes, and C. Baydinc. "Severe Renal Bleeding Caused by a Ruptured Renal Sheath: Case Report of a Rare Complication of Percutaneous Nephrolithotomy." BMC Urology 2 (September 18, 2002): 10.
organizations
American Foundation for Urologic Disease (AFUD). 1128 North Charles Street, Baltimore, MD 21201. (800) 242-2383. http://www.afud.org .
American Urological Association (AUA). 1120 North Charles Street, Baltimore, MD 21201. (410) 727-1100. http://www.auanet.org .
National Kidney Foundation. 30 East 33rd Street, Suite 1100, New York, NY 10016. (800) 622-9010 or (212) 889-2210. http://www.kidney.org .
National Kidney and Urologic Diseases Information Clearing-house (NKUDIC). 3 Information Way, Bethesda, MD 20892-3580.
other
National Kidney and Urologic Diseases Information Clearing-house (NKUDIC). Kidney Stones in Adults. February 1998 [cited April 30, 2003]. NIH Publication No. 94-2495. http://www.niddk.nih.gov/health/urolog/pubs/stonadul/stonadul.htm .
Rebecca Frey, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
A PCNL or mini-PCNL is performed under general anesthesia in a hospital by a urologist, who is a surgeon with specialized training in treating disorders of the urinary tract. ESWL may be done as an outpatient procedure in an ambulatory surgery facility.
QUESTIONS TO ASK THE DOCTOR
- Am I a candidate for a mini-PCNL?
- Do you consider the higher success rate of a PCNL a greater advantage than the lower rate of complications with ESWL?
- What can I do to prevent recurrence of kidney stones?
- What are the chances of my needing another operation?
Thank you.
Please advise.
Thanks.
Ada Co
Thanx!
This is the procedure I'm going to have on January/27/2012
Rick
Hope you heal up nicely and quickly. these surgeries have always been miserable for me, but I realize things could be worse than kidney stones. Stay well.
Thanks
Sardool
For anyone who wants to know this surgery is a pain in the butt. For at least 1 1/2 to 2 weeks after the surgery I was not able to be comfortable in any position. The drain out of my back leaked constantly no matter how much we bandaged it up so i ruined a lot of shirts and had to have our couch cleaned from leaking all over it.
I am feeling pretty good now after 3 weeks still get wiped out if i do to much in a day.
At least I have the 1 1/2 inch kidney stone gone.
I'm a 63-year-old woman in otherwise good health, so I hope that my story is encouraging to anyone reading this thread who may be about to undergo this surgery. I certainly don't mean to sugarcoat this: I was absolutely miserable the first day and I was scared to death they were going to kick me out of the hospital that first day after surgery--after all, I had been told it was a "23-hour observational hospital stay." They pulled the first nephrostomy tube Thursday morning after surgery but were planning to send me home with the other one still attached, with instructions to return TO THE DOCTOR'S OFFICE ON MONDAY! That would have meant walking around with that tube hanging out of my body for an entire weekend. I still think it was insane that this wasn't initially approved as a 2-night stay.
Now I have to heal up & look forward to more lytho or other treatments, to get that staghorn! I am only 45,but had lytho 5your ago. Been having infections since I was 20.
What do I do?