Laser iridotomy
Definition
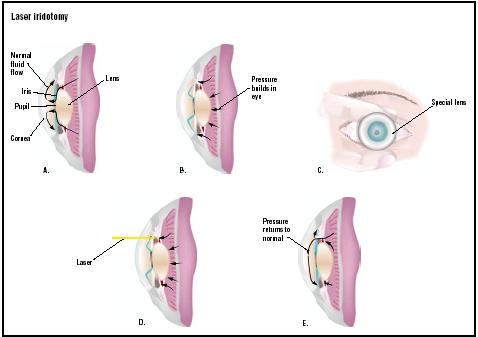
Laser iridotomy is a surgical procedure that is performed on the eye to treat angle closure glaucoma, a condition of increased pressure in the front chamber (anterior chamber) that is caused by sudden (acute) or slowly progressive (chronic) blockage of the normal circulation of fluid within the eye. The block occurs at the angle of the anterior chamber that is formed by the junction of the cornea with the iris. All one needs to do to see this angle is to look at a person's eye from the side. Angle closure of the eye occurs when the trabecular meshwork, the drainage site for ocular fluid, is blocked by the iris. Laser iridotomy was first used to treat angle closures in 1956. During this procedure, a hole is made in the iris of the eye, changing its configuration. When this occurs, the iris moves away from the trabecular meshwork, and proper drainage of the intraocular fluid is enabled.
The angle of the eye refers to a channel in which the trabecular meshwork is located. To maintain the integrity of the eye, fluid must always be present in the anterior (front) and posterior (back) chambers of the eye. The fluid, known as aqueous fluid, is made in the ciliary processes, which are located behind the iris. Released continuously into the posterior chamber of the eye, aqueous fluid circulates throughout the eye. Eventually the fluid returns to the general circulation of the body, first passing through a space between the iris and the lens, then flowing into the anterior chamber of the eye and down the angle, where the trabecular meshwork is located. Finally, the fluid leaves the eye. An angle closure occurs when drainage of the aqueous fluid through the trabecular meshwork is blocked and the intraocular pressure builds up as a result.
For most types of angle closure, or narrow angle glaucoma, laser iridotomy is the procedure of choice. Changes in intraocular pressure (IOP) can alter the name of the condition when the IOP in the eye becomes elevated above 22 mm/Hg as a result of an angle closure. Then,
angle closure becomes angle closure glaucoma. Lowering of the IOP is important because extreme elevations in IOP can damage the retina and the optic nerve permanently. The lasers used to perform this surgery are either the Nd:Yag laser or, if a patient has a bleeding disorder, the argon laser. The majority of patients with glaucoma do not have angle closure glaucoma, but rather have an open angle glaucoma, a type of glaucoma in which the angle of the eye is open.
An angle closure occurs when ocular anomalies (abnormalities) temporarily or permanently block the trabecular meshwork, restricting drainage of the ocular fluid. The anatomical anomalies that make an individual susceptible to an angle closure are, for example, an iris that is bent forward in the anterior chamber (front) of the eye, a small anterior chamber of the eye, and a narrow entrance to the angle of the eye. Some conditions that cause an angle closure are a pupillary block, a plateau iris, phacolytic glaucoma, and malignant glaucoma. The end result of all of these situations is an elevation of the IOP due to a build-up of aqueous fluid in the back part of the eye. The IOP rises quickly when an acute angle attack occurs and within an hour the pressure can be dangerously elevated. The sclera or white of the affected eye becomes red or injected. The patient will usually experience decreased vision and ocular pain with an acute angle closure. In severe cases of acute angle glaucoma, the patient may experience nausea and vomiting. Individuals with neurovascular glaucoma caused by uncontrolled diabetes or hypertension may have similar symptoms, but treatment for this type of glaucoma is very different.
Within a normal eye, the iris is in partial contact with the lens of the eye behind it. Individuals with narrow angles are at greater risk of angle closure by pupillary block because their anterior chamber is shallow; thus, the iris is closer to the lens and more likely to adhere completely to the lens, creating a pupillary block. Patients who experience a pupillary block may have had occasionally temporary blocks prior to a complete angle closure. Pupillary block can be started by prolonged exposure to dim light. Therefore, it not uncommon for an acute angle closure to occur as an individual with a narrow angle emerges from a dark environment such as a theater into bright light. It can also be brought on by neurotransmitter release during emotional stress or by medications taken for other medical conditions. Pupil dilation may be a side effect of one or more of those medications. However, pupillary block is the most common cause of angle closure, and laser iridotomy effectively treats this condition.
The irises of individuals with plateau iris is bunched up in the anterior chamber, and it is malpositioned along the trabecular meshwork. Plateau iris develops into glaucoma when the iris bunches up further; this occurs on dilation of the iris, which temporarily closes off the angle of the eye. Laser iridotomy is often performed as a preventive measure in these patients, but is not a guarantee against future angle closure. This is because changes within the eye, such as narrowing of the angle and increase in lens size can lead to iris plateau syndrome, where the iris closes the angle of the eye even if a laser iridotomy has already been performed. Peripheral laser iridoplasty and other surgical techniques can be performed if the angle still closes after iridotomy.
Other causes of narrow angle glaucoma are not as common. Phacolytic glaucoma results when a cataract becomes hypermature and the proteins of the lens with the cataract leak out to block the angle and the trabecular meshwork. Laser iridotomy is not effective for this type of angle closure. Malignant glaucoma exists secondary to prior ocular surgery, and is the result of the movement of anatomical structures within the eye such that the mesh-work is blocked. Patients who have no intraocular lens (aphakic) are at increased risk for angle closure, as well.
Laser iridotomy is also performed prophylactically (preventively) on asymptomatic individuals with narrow angles and those with pigment dispersion. Individuals with a narrow angle are at higher risk of an acute angle closure, especially upon dilation of the eye. Pigment dispersion is a condition in which the iris pigment is shed and is dispersed throughout the anterior part of the eye. If the dispersion occurs because of bowing of the iris (the case in 60% of patients with pigment dispersion) a laser iridotomy will decrease the bowing or concavity of the iris and subsequent pigment dispersion. This decreases the risk of these individuals to develop pigmentary glaucoma, a condition in which the dispersed pigment may clog the trabecular meshwork. Laser iridotomy is also done on the fellow eye of a patient who has had an angle closure of one eye, as the probability of an angle closure in the second eye is 50%.
There are other indications for laser iridotomy. It is performed on patients with nanophthalmos, or small eyes. Laser iridotomy may be also be indicated for patients with malignant glaucoma to help identify the etiology of elevated IOP. Because laser iridotomy changes the configuration of the iris, it is sometimes used to open the angle of the eye prior to performing a laser argon laser trabeculoplasty, if the angle is narrow. Laser trabeculoplasty is another laser procedure used to treat pigmentary and pseudoexfoliation glaucoma.
Laser iridotomy cannot be performed if the cornea is edematous or opacified, nor if the angle is completely closed. If an inflammation (such as uveitis or neovascular glaucoma) has caused the angle to close, laser iridotomy cannot be performed.
Purpose
The purpose of a laser iridotomy is to allow an equalization of pressure between the anterior (front) and posterior (back) chambers of the eye by making a hole in the superior peripheral iris. Once the laser iridotomy is completed, the intraocular fluid flows freely from the posterior to the anterior part of the eye, where it is drained via the trabecular meshwork. The result of this surgery is a decrease in IOP.
When laser iridotomy is performed on patients with chronic angle closure, or on patients with narrow angles with no history of angle closure, the chances of future pupillary blocks are decreased.
Demographics
Acute angle glaucoma occurs in one in 1,000 individuals. Angle-closure glaucoma generally expresses itself in populations born with a narrow angle. Individuals of Asian and Eskimo ancestry appear to be at greater risk of developing it. Family history, as well as age, are risk factors. Older women are more often affected than are others. Laser iridotomy is performed on the same groups of individuals as those likely to experience angle closures due to pupillary block or plateau iris. They are performed more often on females (whose eyes are smaller than those of males), and more often performed on the smaller eyes of farsighted people than on those of the nearsighted because angle closures occur more frequently in those who are farsighted. Most laser iridotomies are performed on those over age 40 with a family history of plateau iris or narrow angles. However, preventative plateau iris laser iridotomies are performed on patients in their 30s. Individuals who are aphakic (have no intraocular lens) are at greater risk of angle closure and undergo laser iridotomy more frequently than phakic patients. Phakic patients are those who either have an intact lens or who are psuedophakic (have had a lens implant after the removal of a cataract removal).
Description
After the cornea swelling has subsided and the IOP has been lowered, which is usually 48 hours after an acute angle closure, laser iridotomy can be performed. Pilocarpine is applied topically to the eye to constrict the pupil prior to surgery. When the pupil is constricted, the iris is thinner and it is easier for the surgeon to form a penetrating hole. If the eye is still edematous (swollen)—often the situation when the IOP is extremely high—glycerin is applied to the eye to enable the surgeon to visualize the iris. Apraclonidine, an IOP-lowering drop, is applied one hour before surgery. Immediately prior to surgery, an anesthetic is applied to the eye.
Next, an iridotomy contact lens, to which methylcellulose is added for patient comfort, is placed on the upper part of the front of the eye. This lens increases magnification and helps the surgeon to project the laser beam accurately. The patient is asked to look downwards as the surgeon applies laser pulses to the iris, until a hole is formed. Once the hole has penetrated the iris, iris material bursts through the opening, followed by aqueous fluid. At this point, the surgeon can also see the anterior part of the lens capsule through the opening. The hole, or iridotomy, is formed on the upper section of the iris at an 11:00 or 1:00 position, so that the hole is covered by the eyelid. In an aphakic eye, the hole may be made on the inferior iris. After performing the laser iridotomy, the surgeon may place a gonioscopy lens on the eye if the angle has been opened. There is no pain associated with this surgery, although heat may be felt at the site of the lasering.
If a patient has a tendency to bleed, the argon laser will be used to pre-treat the patient prior to completing the procedure with an Nd:Yag laser, or the argon laser alone may be used. The argon laser is capable of photo-coagulation, and, thus, minimizes any bleeding that occurs as the iris is penetrated. Formation of a hole is more difficult with the argon laser because it operates with a decreased power density and the tissue response to the argon laser has greater variability. The argon laser can be used with more patients who have medium-brown irises, however, since the energy of this laser is readily absorbed by irises of this color.
Diagnosis/Preparation
To determine if laser iridotomy is indicated, the surgeon must first determine if and how the angle is occluded. The eye is anesthetized and the aonioscopic lens, which enables the surgeon to see the interior of the eye, is placed on the front of the eye. This is done at the slit lamp biomicroscope in a dark room. In cases of prophylactic surgery, an image of the eye is taken with a ultra-sound biomicroscope in both dim and bright light; this shows the doctor how the patient's iris moves with dilation and constriction, and how this movement can close an angle if the patient has ocular features that predispose the eye to an angle closure.
When an angle is completely occluded (blocked), the elevated IOP usually causes corneal edema (swelling). Because this swelling can obscure the surgeon's view of the iris, prior to performing a laser iridotomy, the IOP must be lowered. One technique to lower the IOP is corneal indentation, in which the gentle pressure is applied several times to the cornea with a lens or hook to open the angle. This pressure on the cornea causes a shift in the internal structures of the eye, enhances aqueous drainage, and lowers the IOP.
The doctor can attempt to lower the IOP medically, as well. One drug that lowers the pressure is acetazolamide, which is given either orally or by intravenous(IV) to decrease aqueous production in the eye. This may be administered up to four times a day, until the adhesion is broken. Another method of lowering the IOP, if acetazolamide is not effective, is with the use of hyperosmotic agents, which through osmosis causes drainage of the aqueous fluid from the eye into the rest of the body. Hyperosmotic agents are given orally; an example of such an agent is glycerine. Given by IV (intravenous administration), mannitol can be used. As the fluid drains from the eye, the vitreous—the jelly-like substance behind the lens in the posterior chamber—shrinks. As it shrinks, the lens in the eye pulls away from the vitreous, creating an opening to the anterior chamber such that aqueous fluid can flow to the anterior chamber. The success of this procedure is increased, due to gravity, if the patient is laying supine.
Once the IOP has begun to decrease, the pressure is further decreased using topical glaucoma medications, such as pilocarpine, or beta blockers. Any inflammation that occurs because of the iridotomy must be controlled with steroid eye drops.
If glaucomatous-like visual field is present prior to surgical intervention, the prognosis for the patient is not as good as if the visual field were completely intact. Thus, a visual field test may be done prior to surgery.
Aftercare
Immediately after the procedure, another drop of aproclonidine is applied to the eye. The IOP is checked every hour for a several hours postsurgery. If the IOP increases dramatically, then the increased IOP is treated until lowered. Because of inflammation is inherent in this procedure, corticosteroids are applied to the eye every five minutes for 30 minutes, then hourly for six hours. This therapy is then continued four times a day for a week. Thereafter, the patient is seen by the surgeon at one week post-surgery and again at two to six weeks post-surgery. If there are complications, the patient is seen more frequently.
After the pressure has been stabilized, a visual field test to determine the extent of damage to the optic nerve may be performed again.
Risks
The greatest risk of laser iridotomy is an increase in intraocular pressure. Usually, the IOP spike is transient and of concern to the surgeon only during the first 24 hours after surgery. However, if there is damage to the trabecular meshwork during laser surgery , the intraocular pressure may not be lowered enough and extended medical intervention or filtration surgery is required. Patients who undergo preventative laser iridotomy do not experience as great an elevation in IOP.
The second greatest risk of this procedure is anterior uvetis, or inflammation within the eye. Usually the inflammation subsides within several days, but can persist for up to 30 days. Thus, the follow-up care for laser iridotomy includes the application of topical corticosteroids. A posterior synechia, in which the iris may again adhere to the lens, may occur if intraocular inflammation is not properly managed.
Other risks of this procedure include the following: swelling of, abrasions to, or opacification of the cornea; and damage to the corneal endothelium (the part of the cornea that pumps oxygen and nutrients into the iris); bleeding of the iris during surgery, which is controlled during surgery by using the iridotomy lens to increase pressure on the eye; and macular edema, which can be avoided by careful aim of the laser during surgery to avoid the macula. The macula is the part of the eye where the highest concentration of photoreceptors is found. Perforations of the retina are rare. Distortion of the pupil and rupture of the lens capsule are other possible complications. Opacification of the anterior part of the lens is common, but this does not increase the risk of cataract formation when compared with the general population.
When the iridotomy hole is large, or if the eyelid does not completely cover the opening, some patients report such side effects as glare and double vision. The argon laser produces larger holes. Patients may also complain of an intermittent horizontal line in their vision. This may occur when the eyelid is raised just enough such that a small section of the inferior part of the hole is exposed, and disappears when the eyelid is lowered. Blurred vision may occur as well, but usually disappears 30 minutes after surgery.
Normal results
In successful laser iridotomy, the IOP differential between the anterior and posterior chambers is relieved and IOP is decreased, and the pupil is able to constrict normally. These are the results of the flatter configuration of the iris after laser iridotomy. If an angle closure is treated promptly, the patient will have minimal or no loss of vision. This procedure is successful in up to 44% of patients treated.
Morbidity and mortality rates
For up to 64% of patients, one to three years after laser iridotomy, the IOP will rise above 21 mmHg, and long-term medical treatment is required. One-third of argon laser iridotomies will close within six to 12 weeks after surgery and will require a repeat laser iridotomy. Approximately 9% of Nd:Yag laser iridotomies must be redone for this reason. Closure of the iridotomy site is more likely if a uveitis presented after surgery. Up to 45% of patients will have anterior lens opacities after laser iridotomy, but these opacifications do not put the patient at an increased risk of cataracts.
Alternatives
An alternative to laser iridotomy is surgical iridectomy , a procedure in which part of the iris is removed surgically. This was the procedure of choice prior to the development of laser iridotomy. The risks for iridectomy are greater than for the laser iridotomy, because it involves an incision through the sclera, the white tunic covering of the eye that surrounds the cornea. The most common complication of an iridectomy is cataract formation, occurring in more than 50% of patients who have had a surgical iridectomy. Since an incision in the eye is required for surgical iridectomy, other procedures, such as filtration surgery—if needed in the future—will be more difficult to perform. Studies comparing the visual outcomes and IOP control of laser iridotomy with surgical iridectomy show equivalent results.
In the case of acute angle closures that occur because of reasons other than, or in addition to pupillary block, argon laser peripheral iridoplasty is performed. During this procedure, several long burns of low power are placed in the periphery of the iris. The iris contracts and pulls away from the angle, opening it up and relieving the IOP.
Resources
books
Albert, Daniel M., M.D. Ophthalmic Surgery Principles and Techniques. Oxford, England: Blackwell Science, 1999.
Albert, Daniel M., M.D. Principles and Practice of Ophthalmology, 2nd ed. Philadelphia, PA: W. B. Saunders Company, 2000.
Azuara-Blanco, Augusto, M.D, Ph.D., et. al. Handbook of Glaucoma. London, England: Martin Dunitz Ltd, 2002.
Kanski, Jack J. M. D., et. al. Glaucoma A Colour Manual of Diagnosis and Treatment. Oxford, England: Butterworth-Heinemann, 1996.
Ritch, Robert, M. D., et. al. The Glaucomas. St. Louis, MO: 1996.
periodicals
Breingan, Peter J. M. D., et. al. "Iridolenticular Contact Decreases Following Laser Iridotomy For Pigment Dispersion Syndrome." Archives of Ophthalmology 117 (March 1999): 325-28.
Brown, Reay H.,M. D., et. al. "Glaucoma Laser Treatment Parameters and Practices of ASCRS Members–1999 Survey." Journal of Cataract and Refractive Surgery 26 (May 2000): 755-65.
Nolan, Winifred P., et. el. "YAG Laser Iridotomy Treatment for Primary Angle Closure in East Asian Eyes." British Journal of Ophthalmology 84 (2000): 1255-59.
Wu, Shiu-Chen, M. D., et. al. "Corneal Endothelial Damage After Neodymium: YAG Laser Iridotomy." Ophthalmic Surgery and Lasers 31 (October 2000): 411-16.
other
"Narrow Angle Glaucoma and Acute Angle Closure Glaucoma." http://www.M.D.eyedocs.com/edacuteglaucoma.htm .
"Laser Iridotomy and Iridoplasty." http://cuth.cataegu.ac.kr/~jwkim/glaucoma/doctor/LI.htm .
"Lasers in the Treatment of Anterior Segment Disorders." http://http:www.tnoa.net/articles/1.HTM .
"Plateau Iris Glaucoma." http://emedicine.com/OPH/topics574.htm .
Martha Reilly, OD
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
A laser iridotomy is performed in an office setting by an ophthalmologist, a doctor or osteopahic doctor with residency training in the treatment of eye diseases. The doctor who performs a laser iridotomy may have advanced fellowship training in the treatment of glaucoma, after completing his or her three-year residency.
QUESTIONS TO ASK THE DOCTOR
- Will this procedure successfully lower the pressure in my eye indefinitely, or will I need further surgery or medication?
- What is the probability that my other eye will also need surgery?
- What will my vision be like after surgery?
- Which laser will you use for my surgery?
- How many laser iridotomies have you performed?
Thanking you in advance, Lori
Before the iridotomy the visual field test was completely normal. A week after the surgery I did a test again and learned that because of the high pressure for two days my visual field had deteriorated by 40%!
I can hardly see with my right eye (which had 100% vision before the iridotomy), I have severe blurred and double vision which, as I was told, is a very common side effect of iridotomy (Nobody told me before, though). Because of the double vision I frequently have to vomit.
I now wear a patch over my right eye, only then can I prevent vomitting.
I can no longer drive a car, I lost my job and have barely enough money for a living. But I can't find a job with just one eye working. I often think of suicide.
My doctor said the iridotomy was a complete success, as it finally lowered the pression. He is very proud of himself.
Please, think twice before letting a doctor perform an iridotomy to your eyes.
Kate
So I have to take more drops than before it was done.
Now the doctor wants to do my right eye, but for what purpose?
Anne
Nobody had ever told me that I had this problem this problem before. I am a women and 45 years old, my blood plessure is alittle high, I am on pills for it. Does anyone know how common of a procedure this is. Thanks for any information Adele.
how was your surgery? I hope it was successful and you had no side-effects.
I had iridotomies 1 year ago and I am still suffering from glare, double vision and other visual aberrations. The inflammation hasn't subsided. I will certainly not have the other eye done!
unfortunately there is no cure for this side effect. The problem will not be removed after implementing the Phakic IOL.
The only possibility might be to suture the iris holes. But there are few doctors who can do that.
Go to
http://198.170.234.66/cgi-local/discus/discus.cgi
Then click on 'Glaucoma' and then on 'Iridotomy'. There are others with your problem The doctor who moderates the forum can give you names of doctors who can perform such surgery if you tell him where you live.
Glare and other visual aberrations after an iridotomy cannot otherwise be cured.
nobody can answer your questions, not even an ophthalmologist. There are many different sorts of narrow angles. The iris may bulge forward and close the trabecular meshwork, it may obstruct
schlemm's canal, it may be too close to the lens, so that posterior synechiae develop, there may be a plateau iris syndrom, etc. For some narrow angles an iridotomy is necessary, for others it should not be done.
All in all, iridotomies have quite a lot of side effects and are not harmless. Go to at least two glaucoma specialists and if you decide for that surgery have it performed by someone who has great experience in doing it. It is a tricky surgery and not all eye doctors know how to do it.
Thank you for your reply (in advance).
you have had your iridotomy by now. I hope everything went well! It is a standard procedure but carries risks, as all surgery does. Most patients have glare, double vision, see strange flashes of light after this surgery. Some cope, others don't. About 20% have severe side effects like a rise in IOP, inflammation, uveitis, cataract development etc.
I do hope you are among those who have only mild symptoms and aberrations. If not, don't have the other eye done. So you can still see normal with one eye.
My optometrist could not think of a reason other than the opthamologist must have hit a nerve. Have you heard of similar outcomes and can anything be done to determine if this is the cause, and how to rectify it? Could the laser have harmed any other area?
Reading your comments, I thought I should really think carefully about going through the operation. The specialist said there are risks, but really didn't give as much detail as I have found here. Thanks to all of you for sharing your experiences.
I have two question:
1- Is there a higher/lower risk associated with the operation depending on the type of the glaucoma you have? (most of you had mentioned narrow angle, and a few said preventative)
2- Is there a higher/lower risk associated with the operation depending on the type of laser used? (such as YAG vs. Argon vs. any other type)
Thanks
1. An iridotomy only makes sens if you have narrow angle glaucoma or if you are in danger of having it.
Opinions are dicides about doing this surgery for patients with pigment dispersion glaucoma. As the iris debris cut out by the laser remains in the eye (doctors have found that debris even 12 years after iridotomy on enucleated eyes)it might obstruct the trabecular meshwork and increase pressure so that you have to have filtering surgery.
2. Argon laser makes larger holes and consequently risks like glare, white line and double vision are very high.
Yag laser has more energy and consequently risks like retinal detachment due to the shock waves and bleeding are very high.
But with either laser you will have serious side effects.
In any case iridotomy has many, many very severe side effects and can ruin your vision forever.
Test your doctor. Ask him what the side effects are. If he says there are none or if he says the risks are low, then go and get a second opinion, because a doctor who says risks of this surgery are low is a liar.
I've just been told I need laser iridotomy for narrow angles. Reading all these comments about side effects is pretty scary. Has anyone had a good experience with this surgery?
After readding that success rate of this procedure are 44% and what I've read here, I'm not so sure of wanting to do it. The procedure looks quite riskey and to my opinion not worth the risk. Besides, in some cases the procedure must be repeated after a few years.
I want to thank the people who shared their information here and helped me to come and make my decision.
My mother lost sight in one eye many years ago due to an acute attack of low-angle glaucoma that she never told anyone about. By God's grace, my youngest sister was in the hospital to have corrective surgery. The eye surgeon noticed my mom's eye and immediately had her admitted for emergency surgery that saved that eye.
I have high hypermetropia (+8.25, +8.5 glasses which do not allow me to see as basic people do)
Following a UBM exam, I was told I might have a closed angle glocauma, and as prevention, I should make the irodotomy operation to my eyes.
Right eye done without problems. Left eye done 2 weeks later (3 weeks ago)
One hour before the operation, I put three kind of drops in my eyes : (1. to lower the pressure of my eye, 2. to shrink the iris 3. anti-inflammatory)
And then for 2 weeks, I put two anti-inflammatory drops 3 times a day. (I stopped putting the drops last week.)
The problem is that, since the operation of my left eye :
• When I wake up, I have to wait something like 6 seconds to see clearly with my left eye. During the 6 seconds, it usually starts by complete dark. Or only a round is clear and the rest is black, then this clear round becomes bigger to see "normally". During the day, the alteration is mainly by dark or light splotches everytime I move.
• And when I close my left eye during the day or before sleeping, I keep seeing some light. As if I looked to a high source of light before.
• I feel also that my lateral vision has been significantly altered. (I did not have an increase in the pressure of my eye during the operation, nor a week after)
Although my doctor asked me to "wait", I don't feel my eye will come back to normal. Did anybody have a similar problem before ?
Besides, I was surprised that my doctor did not make the exams corresponding to my description : turn off the light, then turn it on to see the reaction of my eye, check my lateral vision ...etc
Are there well known exams to check such deficiencies ?
Is there anything I can do to get my eye come back to normal or to avoid worsen this situation ? Example avoid light changes shocks and start wearing sun glasses ?
Thanks in advance.
I do not know what a "stressed nerve" means and now I am stressed worst than before my surgery I would appreciate to hear you opinion. Thanks
should i be concerned if my doctor wanting to perform a 4th time iridotomy?
i am however not plannig to go ahead for the fourth surgery!!
thank you in advance for your reply
The procedure itself was no more than a bit uncomfortable with a slight headache which quickly subsided.
My eyes are now a little achy with some on and off blurriness when administering drops every hour. I have to go back to the consultant in 10 days time for a check up.
The following day when I woke up in the morning, my vision was absolutely fine. Just great. No Pain at all. I went to my office and did my daily chores. In between only for 2/3 times, I experienced a very mild pain that lasted for some few seconds only which was not an issue at all following the laser surgery that I had undergone. Today is the second day and I am just like before. Nothing abnormal. I am very happy with my condition.I was told before hand by my doctor that 90% of Iridotomies are always successful and the ones that fail may require a filtering or incisional surgery.But your specialist doctor is the best judge to look whether Iridotomy is necessary in your case or not.
Friends,I also had done my research on the net before undergoing Iridotomy and ran in to many horrific comments made by some people whose iridotomies went haywire, but believe me mine was absolutely perfect. No trouble at all. No white line, no glare,no double images,nothing at all.I can not see the holes in my eyes.That’s the result of the YAG laser,absolutely perfect.
What I would suggest to people who are suggested Iridotomies by some doctor is:-
1)Go to a top notch surgeon who is a Master of Surgery with years of experience in the laser department. It would be more better if he is a Glaucoma specialist too(Mine was a M.S who is proficient in doing laser surgeries as well as a renowned Glaucoma Specialist)
2)Check how many laser surgeries he has performed in the past and his success ratio.Discuss everything with him that you want to know about the procedure etc.
3)Ask that specialist if your eye condition can be treated without the iridotomy (whether another alternative is possible)
4)If the specialist tells you to undergo the Iridotomy and if he possesses all the above required criteria then don't hesitate to get this procedure done as the specialist is the best one to judge your condition.
5) If at all you are not satisfied by the response you get to your queries, take a second opinion of another renowned surgeon. (I did take a second opinion and that doctor also told me to get the Iridotomy done)
6)Friends,never defer your Iridotomy just by reading the negative comments on the Internet on some forums or blogs etc.I don't mean to say that the ones who had the side effects are fake or wrong, but there are many factors that may have resulted in the Iridotomy going haywire for them.The reasons may be the ones that I have already explained above.
The main reason of my posting the comments here is that not much people who have had the iridotomies done to their eyes care to report their success stories,but the ones who were unsuccessful do voice their concern, but some of them scare people to death and in this way they are doing huge dis-service to mankind and causing wrong fear in the minds of people who are suggested this procedure. If someone's Iridotomy failed due to some reason, it doesn't mean that everyone will suffer. By causing wrong fear such people are pushing others into an abyss of blindness.Iridotomies have never caused serious side effects unless not done properly and in cases where it was not required at all,that's it.
- history of dental and ceasarean hemmorage and both times I was given vitamin K injections. Blood work showed high risk of hemmorage. Currently on daily dose of 81 mg ASA.
- had severe allergic reaction to naprosyn for a frozen shoulder treatment.
Is it advisable for me to go through the YAG iridotomy treatment as a preventive measure for glaucoma.
Before the op the pressure was 25 and after it came down to 17. It was uncomfortable and I definitely felt the six hits but nothing too bad. After a couple of days of mild discomfort my eye felt normal and has done ever since, I also had perfect vision in that eye (which I didn't have before) for a day!
I went back to the hospital last week as I am scheduled to have my right eye done on Thursday, and they told me that the pressure in both eyes was 38!!! They're still recommending I go ahead with the procedure this week on my right eye, but have now given me drops for both eyes to administer twice a day (I assume for the rest of my life) to try to reduce the pressure. They still say that I should go ahead and have the other eye done as the pressure is very high. I would rather do that than go blind though. I too had mine done on the NHS in the UK.
Just thought that this site needs some positive feedback.
Good luck and wishes to you all
the success rate of lasergrodotomy is only 40% and in face of so many adverse comments of patients why the
eye sergons are still insisting upon lasergrodotomy is beyound understanding.
I know that the risk of an acute attack is getting greater as my angle constricts further, but my fear of ruining my good eye is intense.
Since I reported the bad news, I wanted to report the good news. I'm so grateful to have the second eye spared the distortion of the first that I am "over the moon." I'm also glad that I don't have three eyes!
How long did you have to stay at the Dr's office after you had the surgery?
As promised... this morning I had a Laser Iridotomy procedure done in my left eye. I would like to say, that so far everything has gone smoothly. I see my Ophthalmologist again tomorrow morning for a follow-up. During the procedure I experienced no real pain, some discomfort as I don't like anyone near my eyes to begin with. However, I coped with that because I had built up a relationship with the doctor before hand. This doctor also performed cataract surgery on my father last year and I went to all of his appointments. I was well prepared (research wise) having made my decision to have this preventative procedure performed on my left eye.
I will follow-up with another posting in a day or two to let you know my progress. I do feel sorry for those who have had a bad experience with their surgeries/procedures. I am not dismissing your claims. I just think there needs to be some non biased posting on the internet. At the end of the day, no one should enter into a medical procedure of any kind without some of their own personal research. If you don't know how to research your procedure visit your local public library. The library staff will be glad to help.
Good health to all!
Ray
Here I am again with a ten day post procedure update. As I am posting this I have had absolutely no discomfort or pain in the eye, nor have I had any white line distortion that others have reported. I know each case will differ, but I am just sharing my experiences.
I did see the Ophthalmologist the following day and he was very pleased with how everything was looking. With this appointment we discussed having the same procedure performed on my right eye. I will probably be getting that done later in the spring - for the same reason a preventative procedure.
Anne, if your experience is anything like mine, you will probably end up kicking yourself in the butt for putting it off. I wish you all the best health when you do eventually have the procedure.
Warmest regards,
Ray
Thanks to everyone who posts their successes. It is true that these posts lean toward those who have had negative experiences, as we humans are more vocal about our unhappiness than our happiness!
I wish there were more definitive research completed on the position of the iridotomy holes and vision problems. Comments, anyone?
On 16th of January this year I went through iridotomy. I was told that I have narrow drainage angles. However, I have not been told about any side effects that might follow this procedure. I am seeing a horizontal white line across my left eye. It looks like a glare from light and I see it when I look from darker space into lighter (like in a day light, looking at the window, computer screen). I have been examined twice after the procedure by NHS doctors and have described to them what I see. They both seem do not really pay any attention to it and said that what I see it is floaters and nothing to worry about. It is not floaters as I know what floaters are look like. I did not have any problems with my vision before in my life. This white line is quite disturbing, especially when I am driving or working at the computer. It makes me wanting to rub my eye and take the distraction away. I went on-line and have read about such an effect as the opening in my iris was done too high and is not covered by my eye lid. Apparently it is impossible to see during examination. I could not find the answer if this effect will go away and if so then when?
I would appreciate very much if you could answer to my question.
Tanya W.
I had an iridotomy done in my left eye 2 years ago, the hole was made in the 3 o'clock position, and my eyelid does not cover it, I have extreme cloudiness, glare, and double vision in that eye, I had the other eye done in the 12 o'clock position and have had no problems at all. I complained and complained about this to my doctors and they kept telling me that my brain would get used to it and I wouldn't notice after awhile, I had one doctor tell me that I should ignore it, and that it was always going to be with me and that I should name it, he asked me if I liked the name Oscar for it? Very professional, right? I have tried colored contact lenses, and they did not work for me, one doctor recommended a tatoo over it, but fda doesn't approve that procedure any longer. They talked about suturing it, but that is a risky procedure and most doctors will not do it. They are now talking about cataract surgery, and I don't have a cataract, so I don't know how that will help. I hope you are doing better, but in my experience, this is something that has to be lived with and it is very dibilitating and more then that very frustrating that no help can be given.
problems whatsoever
best wishes any one about to have it.
End results: left eye done, I did feel the last two "shots" a bit but no real pain. Right eye, have to come back in 4 weeks' time to get it redone, as my iris is dark and thicker than normal, max number of shots done for the session.
My eyes were a little bit irritated but after I put the prescribed cortisone drops, they were fine.
So far my vision is still fine, no stray light, no floaters, no blurry, no pain.
I do however experienced light constant headaches around the temples, forehead & back of the head. I took Tylenol and it did the trick. The headaches seemed to have subsided after 2 days. Maybe it was from me stressing out.
I recommend wearing a good pair of sunglasses when you go outside into natural sunlight after the surgery, it minimizes the discomfort to your eyes.
Good luck to those about to have the procedure done.
Susana
10/17/12
I'll be seeing my guy again next week, but I have absolute confidence that iridotomy was the right op and that the surgeon who did it was competent. Unfortunately, I don't live in NYC, but all I can say is don't be nervous. The alternative is too awful to contemplate really (blindness). I live in the UK, but I'm sure your practitioners have the same kinds of certification and medico-legal obligations as anywhere else in the world, don't they?
I thank you, Kate, for posting your story and your experience following LPI. Kate, your story has touched me.
I truly hope that you are well. My prayers are with you.
Each person who has posted
Thank you for sharing with me and others of your experiences. You are in my prayers for God's healing hand upon your life.
You have all helped me by sharing your stories, some terrible, some hopeful, all revealing and heartfelt.
May God keep us all in the palm of His Hand.
In Love,
N
Doctor says I need YAG lesser hole drilling to prevent possible severe problems (blindness) with overpressure due to drainage.
Sounds like a plumber job ?
I have only one "good" eye, the other is what they call "lazy eye" syndrome (out of focus).
Surgery set for March 2013.
I like the Doctor but he has no experience with Laser, since his office does not have the apart us, he shares it with other Doctors, so gets it every few months or so.
ShouldI look for a more experienced Doctor or laser surgery center where they do this on more routine basis.
I coud let him practice on my lazy eye first !
I saw your post and just wanted to say that I did not have the cataract surgery, because my insurance wouldn't pay for it, my eye did not warrant cataract surgery, so I ended up having the iridotomy hole sutured in Sept. I will say that do not have the glare in that part of my eye any longer, but while doing the surgery the doctor put a tear in my iris accidentally and I have since developed a cataract in that eye, so i am basically back to square one, having a difficult time seeing out of that eye. I see the eye doctor again in February and we are going to discuss cataract surgery again and when he does that he will repair the tear in the iris. This has been a nightmare, and I have lived with it for over 2 1/2 years since I had the iridotomy done. Good luck to all.
I am 32 years old and last month it turned out that my IOP is too high. It was expected as my father and his father have glaucoma. So i was recommended to perform iridotomy. It was done 6 days ago. There were no discomfort on the next day. Intervention itself just was not so pleasant, but it was quick. Yesterday doctors checked my IOP and it seems at it was before the intervention. They said that this is normal as the intervention was so soon. They expect IOP values to drop next few weeks.
I wanted to ask people done the same procedure how long after the intervention there were noticeable drop in IOP values?
Thanks in advance!
Best regards.
Glaucoma is a serious eye disease that steals sight. Listen to your doctor.
I was not told of any risks my right eye suffered a retina detachment many years ago which I lost alot of sight out of, now my good eye (the left one) has now got a white horizontal line in it.
Is there nothing that can be done about this? Surely they can cover it and reposition it?
Any help truly appreciated, I am lost with what to do next, as I live in New Zealand, we are limited to options, but I need to do something as I can't handle it the way it is!!
Help please!
What I would like to know is what type of laser surguries you folks have had. I was told I need Argon laser because I have brown eyes, thicker iris are harder to penetrate. I've read that Argon laser makes a bigger hole with an increased chance of having glare, ghosting or double vision. Then I'm told it will be done at 3 and 9 o'clock. When I explained that I read 12 o'clock was the preferred placement my doctor said not anymore. it used to be thought that was the best placment but new studies show otherwise, with less undesired side effects at 3 and 9.
I had 4 opinions and 3 out of 4 say I need this done and she comes highly recommended, yet I am having a very difficult time making a decison. I've read that only about 1/4 percent of people diagnoised with this go on to have an accute attack... what to do?
Only I can make this decision but I sure would appreciate a pep talk.
I definitely understand how everyone feels. I was a big chicken when they told me I needed the iridotomies, but went through with the first one then so that I did not have time to get all nervous and I am glad I did.
Hopefully these procedures will help me to avoid IOP issues for the long run.
Good luck to all!
My husband had 20 surgeries for retinal detachment, lost the vision on his left eye.
After all this comments I will wait for a second and third opinion before I get it done.
Freaking out now!
Thanks.