Breast reconstruction
Definition
Breast reconstruction is a series of surgical procedures performed to recreate a breast. Reconstructions are commonly begun after portions of one or both breasts are removed as a treatment for breast cancer. A breast may need to be refashioned for other reasons such as trauma or to correct abnormalities that occur during breast development.
Purpose
Many experts consider reconstruction to be an integral component of the therapy for breast cancer. A naturally appearing breast offers a sense of wholeness and normalcy, which can aid in the psychological recovery from breast cancer. It eliminates the need for an external prosthesis (false breast), which many women find to be physically uncomfortable as well as inconvenient.

Demographics
Breast surgery, including reconstruction, is the second most commonly performed cosmetic surgical procedure practiced on women in the United States. It increased by 306% between 1992 and 1998. According to the American Society of Plastic and Reconstructive Surgeons, more than 125,000 breast augmentation or reconstruction procedures are performed each year.
Presently, more than two million, or approximately 8%, of women in the United States have breast implants . The majority of breast implant recipients are Caucasian women (95%), followed by African-American women (4%). The remaining women that have breast implants are Asian (0.5%) and other non-specified races (0.5%).
Description
Breast reconstruction is performed in two stages, with the ultimate goal of creating a breast that looks and feels as natural as possible. It is important to remember that while a good result may closely mimic a normal breast, there will inevitably be scars and some loss of sensation. The reconstructed breast cannot exactly match the original.
The first step is to create a structure called a breast mound. This can be accomplished using artificial materials called breast implants, or by using tissues from other parts of the woman's body. The second step involves creating a balance between the newly constructed breast and the breast on the opposite side. The nipple and areolar complex (darker area around the nipple) are recreated. This is usually done several months after the mound is created, to allow swelling to subside. Other procedures may be necessary, such as lifting the opposite breast (mastopexy) or making it larger or smaller to match the reconstructed breast.
Immediate or delayed reconstruction
While immediate reconstruction (IR) is not recommended for women with breast cancer who need to undergo other, more important treatments, breast reconstruction can be done almost anytime. It can be delayed, or it can be completed during the same procedure as the mastectomy. There are psychological benefits to IR. The ability to return to normal activities and routines is often enhanced when reconstruction follows immediately after mastectomy. A better final appearance may result from IR. There is less skin removal, often resulting in a shorter
The cost of IR is generally lower than the cost of delayed reconstruction (DR). There is one less operation and hospital stay. Surgeon's fees may be lower for a combined procedure than for two separate surgeries.
There are disadvantages of IR as well. The surgery itself is longer, resulting in more time under anesthesia. Postoperative pain and recovery time will be greater than for mastectomy alone.
Other authorities contend that delayed reconstruction (DR) offers different physical and psychological advantages. The initial mastectomy procedure alone takes less time, and has a shorter recovery period and less pain than mastectomy and IR. The woman has more time to adjust to her diagnosis and recover from additional therapy. She is better able to review and evaluate her options and to formulate realistic goals for reconstruction. Some reconstructive surgery requires blood transfusions. With DR, the patient can donate her own blood ahead of time ( autologous blood donation ), and/or arrange to have family and friends donate blood for her use (directed donation).
The psychological stress of living without a breast is a disadvantage of DR. The extra procedure needed to perform DR results in higher costs. Although initial recovery is faster, an additional recuperation period is required after the delayed operation.
Type of reconstruction
There are two basic choices for breast reconstruction. The breast tissue can be replaced with an implant, or the breast is created using some of the woman's own tissues (autologous reconstruction).
ARTIFICIAL IMPLANTS. In general, implant procedures take less time and are less expensive than autologous ones. Implants are breast-shaped pouches. They are made of silicone outer shells, which may be smooth or textured. The inside contains saline (salt water). Implants made prior to 1992 were filled with silicone gel. In 1992, the Food and Drug Association (FDA) discontinued the use of silicone as a filling material.
An implant may be a fixed-volume type, which cannot change its size. Implants that have the capacity to be filled after insertion are called tissue expanders. These may be temporary or permanent.
The initial procedure for any implant insertion uses the mastectomy incision to make a pocket of tissue, usually underneath the chest wall muscle. In DR, the mastectomy scar may be reopened and used for this purpose, or a more cosmetic incision may be made. The implant is inserted into the pocket, the skin is stretched as needed, and sutured closed.
If there is inadequate tissue to achieve the desired size, or a naturally sagging breast is desired, a tissue expander is used. It resembles a partially deflated balloon, with an attached valve or port through which saline can be injected. After the initial surgical incision is healed, the woman returns to the doctor's office on a weekly or bi-weekly basis to have small amounts of saline injected. Injections can continue for about six to eight weeks, until the preferred size is obtained. In some cases, it may initially be overfilled and later partially deflated to allow for a more pliable, natural result. A temporary tissue expander is removed after several months and replaced with a permanent implant.
IR surgery using an implant takes approximately two to three hours, and usually requires up to a three-day hospital stay. Implant insertion surgery that is accomplished as part of DR takes one to two hours and can sometimes be done as an outpatient procedure. Alternatively, it may entail overnight hospitalization.
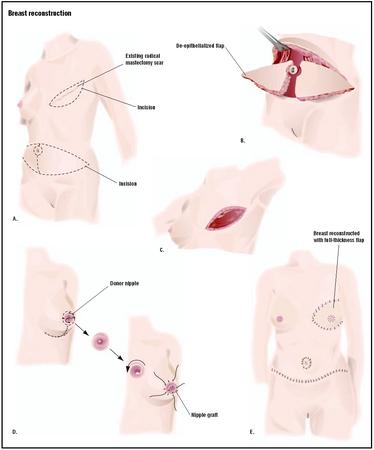
AUTOLOGOUS RECONSTRUCTION. Attached flap and free flap are two types of surgery where a woman's own tissue is used in reconstruction. An attached flap uses skin, muscle, and fat, leaving blood vessels attached to their original source of blood. The flap is maneuvered to the reconstruction site, keeping its original blood supply for nourishment; this is also known as a pedicle flap. The second kind of surgery is called a free flap, which also uses skin, muscle, and fat, but the surgeon severs the blood vessels and reattaches them to other vessels where the new breast is to be created. The surgeon uses a microscope to accomplish the delicate task of sewing blood vessels together (anastomosis). Sometimes, the term microsurgery is used to refer to free flap procedures. Either type of surgery may also be called a myocutaneous flap. This refers to the skin and muscle used.
The skin and muscle used in autologous reconstruction can come from one of several possible places on the body, including the abdomen (tummy tuck flap), the back (latissimus dorsi flap), or the buttocks (gluteus maximus free flap).
Finishing the reconstruction
Other procedures may be necessary to achieve the goal of symmetrical breasts. It may be necessary to make the opposite breast larger (augmentation), smaller (reduction), or higher (mastopexy). These, or any other refinements, should be completed before the creation of a nipple and areola. Tissue to form the new nipple may come from the reconstructed breast itself, the opposite breast, or a more distant donor site such as the inner thigh or behind the ear. The nipple and areolar construction is usually accomplished as an outpatient procedure. A final step, often done in the doctor's office, is tattooing the new nipple and areola to match the color of the opposite nipple and areola as closely as possible.
Insurance
Insurance coverage varies widely for breast reconstruction. Some policies will allow procedures on the affected breast, but refuse to pay for alterations to the opposite breast. Other plans may cover the cost of an external prosthesis or reconstructive surgery, but not both. The Women's Health and Cancer Rights Act of 1998 requires group health plans and health issuers to provide medical and surgical benefits with respect to mastectomy and to cover the cost of reconstructive breast surgery for women who have undergone a mastectomy.
Implants may pose additional insurance concerns. Some companies will withdraw coverage for women with implants, or add a disclaimer for future implant-related problems. Careful reading of insurance policies, including checking on the need for pre-approval and a second opinion , is strongly recommended.
Diagnosis/Preparation
The diagnosis for breast reconstruction is almost always made on a visual basis. The underlying medical reasons include replacing all or part of breast tissue that has been removed during the course of cancer treatment, replacing breast mass that has been lost due to injury, or equalizing otherwise normal breasts that are markedly different in size. Underlying cosmetic reasons include personal preference for larger breasts among genetic females or the creation of breasts in male-to-female transsexuals.
Routine preoperative preparations, such as having nothing to eat or drink the night before surgery, are needed for reconstructive procedures. Blood transfusions are often necessary for autologous reconstructive surgeries. The patient may donate her own blood and/or have family and friends donate blood for her use several weeks prior to the surgery.
Emotional preparation is also important. Breast reconstruction will not resolve a psychological problem the woman had before mastectomy, nor make an unstable relationship strong. An expectation of physical perfection is also unrealistic. A woman who cites any of these reasons for reconstruction shows that she has not been adequately informed or prepared. Complete understanding of the benefits and limitations of this surgery are necessary for a satisfactory result.
Not all women are good candidates for breast reconstruction. Overall poor physical health, or specific problems such as cigarette smoking, obesity, high blood pressure, or diabetes, will increase the chance of complications. Also, a difficult or prolonged recovery period or failure of the reconstruction may be a result. A woman's physical ability to cope with major surgery and recuperation should also be considered.
Aftercare
The length of the hospital stay, recovery period, and frequency of visits to the doctor after surgery vary considerably with the different types of reconstruction. In general, autologous procedures require longer hospitalization and recovery times than implant procedures. For all surgical procedures, bandages and drainage tubes remain in place for at least a day. Microsurgical or free flap procedures are most closely monitored in the first day or two after surgery. The circulation to the breast may be checked as often as every hour. Complete breast reconstruction requires at least one additional surgery to create a nipple and areola. Scars may remain red and raised for a month or longer. They will fade to their final appearance within one to two years. The true, final appearance of the breasts usually will not be visible for at least one year.
Risks
Some women have reported various types of autoimmune-related connective tissue disorders, which they attribute to their implants—usually involving silicone gel implants. Lawsuits have been filed against the manufacturers of these implants. Food and Drug Administration (FDA) guidelines, issued in 1992, now greatly restrict their use, primarily to women who need to replace an existing silicone gel-filled implant. In addition, recipients must sign a consent form that details the potential risks of silicone gel-filled implants and become enrolled in a long-range study. Saline is now the filling of choice for breast implants. Saline-filled implants are permitted for all uses, although manufacturers must continue to collect data on possible risks.
The FDA issued a status report on Breast Implant Safety in 1995, and revised it in March 1997. It noted that studies to date have not shown a serious increase in the risk of recognized autoimmune diseases in women with silicone gel-filled breast implants. It also addressed concerns about other complications and emphasized the need for further study of this issue.
There are a number of risks common to any surgical procedure, such as bleeding, infection, anesthesia reaction, or unexpected scarring. Hematoma (accumulation of blood at the surgical site), or seroma (collection of fluid at the surgical site) can delay healing if they are not drained. Any breast reconstruction also poses a risk of asymmetry and the possible need for an unplanned surgical revision. Persistent pain is another potential complication of all types of breast reconstruction.
Implants have some unique problems that may develop. A thick scar, called a capsule, forms around the implant as part of the body's normal reaction to a foreign substance. Capsular contracture occurs when the scar becomes firm or hardened. This may cause pain accompanied by changes in the texture or appearance of the breast. Implants can rupture and leak, deflate, or become displaced. The chances of capsular contracture or rupture increase with the age of the implant. These complications can usually be remedied with outpatient surgery to loosen the capsule and remove or replace the implant as needed. There is some evidence that using implants with textured surfaces may decrease the incidence of these problems. An implant tends to remain firm indefinitely. It will not grow larger or smaller as a woman's weight changes. Asymmetry can develop if a woman gains or loses a large amount of weight.
The autologous procedures all carry a risk of flap failure, which is a loss of blood supply to the tissue forming the new breast. If a large portion of the flap develops inadequate blood supply, another reconstructive technique may be necessary. Tummy tuck flap procedures can result in decreased muscle tone and weakness in the abdomen, or lead to an abdominal hernia. Arm weakness may occur after latissimus dorsi flap surgery.
Normal results
A normal result of breast reconstruction depends on the woman's goals and expectations. It will not be the same as the breast it replaces. In general, the reconstructed breast should be similar in size and shape to the opposite breast, but will have less sensation and be less mobile than a natural breast. A reconstruction using an implant will usually be firmer and rounder than the other breast. It may feel cooler to the touch, depending on the amount of tissue over it. Scars are unavoidable, but should be as inconspicuous as possible.
Morbidity and mortality rates
Normal scar formation should be expected. With any silicone prosthesis, a capsule usually forms around it. However, in some instances a mild form of capsular contraction may develop. Mild ridges that can be felt under the skin categorize this condition. If the capsule contracts, as occasionally occurs, it results in a hardening of the breast. There is no way to predict who will excessively scar. Other risks include infection, excessive bleeding, problems associated with anesthesia, rupturing of the implant, and leakage. There have been a total of 120,000 reports of ruptured silicone implants. Approximately 50,000 reports of breakage have been received for saline implants.
Deaths associated with breast reconstruction are extremely rare. Most post-surgical mortality has been attributed to anesthesia errors or overdoses of pain medications.
Alternatives
Alternatives to breast reconstruction surgery include using external breast forms that fit into brassiere cups or are attached to the skin of the chest. Creams that allege to increase breast size usually produce no noticeable results. The use of creams containing hormones can lead to long-term hormonal imbalances. Reputable experts do not generally recommend these preparations for breast enlargement.
Resources
books
Ball, Adrian S., and Peter M. Arnstein. Handbook of Breast Surgery. London: Edward Arnold, 1999.
Berger, Karen J., and John Bostwick. A Woman's Decision: Breast Care, Treatment & Reconstruction, 3rd edition. St. Louis: Quality Medical Publshers, 1998.
Bostwick, John. Plastic and Reconstructive Breast Surgery, 2nd edition. St. Louis: Quality Medical Publishers, 1999.
Engler, Alan M. BodySculpture: Plastic Surgery of the Body for Men and Women, 2nd edition. London: Hudson Pub., 2000.
periodicals
Colville, R. J., N. R. McLean, C. A. Mallen, and L. McLean. "The Impact of Breast Augmentation on the Breast-screening Programme." British Journal of Plastic Surgery, 55, no. 7 (2002): 592–593.
Hudson, D. A. "Submuscle Saline Breast Augmentation: Are We Making Sense in the New Millenium?" Aesthetic and Plastic Surgery 26, no. 4 (2002): 287–290.
Jejurikar, S. S., J. M. Rovak, W. M. Kuzon Jr, K. C. Chung, S. V. Kotsis, and P. S. Cederna. "Evaluation of Plastic Surgery Information on the Internet." Annals of Plastic Surgery 49, no. 5 (2002): 460–465.
Smith, M., and K. Kent. "Breast Concerns and Lifestyles of Women." Clinics in Obstetrics and Gynecology 45, no. 4 (2002): 1129–1139.
organizations
American Board of Plastic Surgery. Seven Penn Center, Suite 400, 1635 Market Street, Philadelphia, PA 19103-2204. (215) 587-9322. http://www.abplsurg.org/ .
American College of Plastic and Reconstructive Surgery. http://www.breast-implant.org .
American College of Surgeons. 633 North Saint Claire Street, Chicago, IL 60611. (312) 202-5000. http://www.facs.org/ .
American Society for Aesthetic Plastic Surgery. 11081 Winners Circle, Los Alamitos, CA 90720. (800) 364-2147 or (562) 799-2356. http://www.surgery.org/ .
American Society of Plastic Surgeons. 444 E. Algonquin Rd., Arlington Heights, IL 60005. (888) 475-2784. http://www.plasticsurgery.org/ .
other
American Society of Cosmetic Breast Surgery. Information about Breast Surgery. [cited February 24, 2003] http://www.breast-implant.org .
National Library of Medicine. Breast Implants. [cited February 24, 2003] http://www.nlm.nih.gov/medlineplus/breastimplantsbreastreconstruction.htm .
Public Broadcasting System Breast Implants on Trial. [cited February 24, 2003] http://www.pbs.org/wgbh/pages/frontline/implants/cron.html .
U.S. Food and Drug Administration. Breast Implants. [cited February 24, 2003] http://www.fda.gov/cdrh/breastimplants/labeling/mentor_patient_labeling_5900.htm .
L. Fleming Fallon, Jr., MD, DrPH
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Breast reconstruction is normally performed by a surgeon with advanced training in plastic and reconstructive procedures. It is commonly, but not exclusively, performed as an outpatient procedure.
QUESTIONS TO ASK THE DOCTOR
- What will be the resulting appearance?
- Is the surgeon board certified in plastic and reconstructive surgery?
- How many procedures has the surgeon performed?
- What is the surgeon's complication rate?