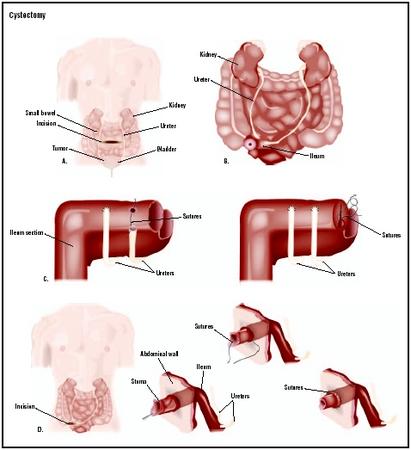
Cystectomy
Definition
Cystectomy is a surgical procedure that removes all or part of the urinary bladder, the muscular organ that collects urine from the kidneys for excretion at a later time. Partial or segmental cystectomy removes part of the bladder; simple cystectomy removes the entire bladder; and radical cystectomy removes the bladder as well as other pelvic organs or structures.
Purpose
Cystectomy is most commonly performed to treat cancer of the bladder. Once a patient has been diagnosed with bladder cancer, a staging system is used to indicate how far the cancer has spread and determine appropriate treatments. Superficial tumors isolated to the inner lining of the bladder (stage 0 or I) may be treated with non-surgical therapies such as chemotherapy or radiation, or with partial or simple cystectomy. Radical cystectomy is the standard treatment for cancer that has invaded the bladder muscle (Stage II, III, or IV). Muscle-invasive cancer accounts for 90% of all bladder cancers.
Other conditions that may require cystectomy include interstitial cystitis (chronic inflammation of the bladder), endometriosis that has spread to the bladder, severe urinary dysfunction, damage to the bladder from radiation or other treatments, or excessive bleeding from the bladder.
Demographics
Approximately 56,500 cases of urinary bladder cancer are diagnosed in the United States annually, with approximately 12,600 men and women dying of the disease each year. Men are more often diagnosed with bladder cancer (2.6 men for each woman diagnosed), and they also have a higher mortality rate (two men for each woman that dies). The average age that the disease is diagnosed is 65 years.
More cases of bladder cancer are found among white men and women. The Centers for Disease Control and Prevention (CDC) reported that from 1992–1999, whites were diagnosed with bladder cancer at a rate of 21.9 per 100,000 persons, while African Americans had a rate of only 12.4 per 100,000. The mortality rate, however, is similar among white and African-American patients (4.5 and 4.1 per 100,000 persons), respectively.
Description
Partial cystectomy
During partial or segmental cystectomy, only the area of the bladder where the cancer is found is removed. This allows for most of the bladder to be preserved. Because the cancer must not have spread to the bladder muscle and must be isolated to one area, partial cystectomy is only used infrequently for the patients who meet these select criteria.
The patient is first placed under general anesthesia. After an incision is made into the lower abdomen, the bladder is identified and isolated. The surgeon may choose to perform the operation with the bladder remaining inside the abdominal cavity (transperitoneal approach) or with the bladder lifted outside of the abdominal cavity (extraperitoneal approach). The cancerous area is excised (cut out) with a 0.8 in (2 cm) margin to ensure that all abnormal cells are removed. The bladder is then closed with stitches. The pelvic lymph nodes may also be removed during the procedure. After the cancerous tissue is removed, it is examined by a pathologist to determine if the margins of the tissue are clear of abnormal cells.
Simple or radical cystectomy
While partial cystectomy is considered a bladder-conserving surgery, simple and radical cystectomy involves the removal of the entire bladder. In the case of radical cystectomy, other pelvic organs and structures are also removed because of the tendency of bladder cancer to spread to nearby tissues. After the patient is placed under general anesthesia, an incision is made into the lower abdomen. Blood vessels leading to and from the bladder are ligated (tied off), and the bladder is divided from the urethra, ureters, and other tissues holding it in place. The bladder may then be removed.
The surgical procedure for radical cystectomy differs between male and female patients. In men, the prostate, seminal vesicles, and pelvic lymph nodes are removed with the bladder. In women, the uterus, fallopian tubes, ovaries, anterior (front) part of the vagina, and pelvic lymph nodes are removed with the bladder. If the surgery is being performed as a treatment for cancer, the removed tissues may be examined for the presence of abnormal cells.
Urinary diversion
Once the bladder is removed, a new method for excreting urine must be created. One commonly used approach is the ileal conduit. A piece of the small intestine is removed, cleaned, and tied at one end to form a tube. The other end is used to form a stoma, an opening through the abdominal wall to the outside. The ureters are then connected to the tube. Urine produced by the kidneys flows down the ureters, into the tube, and through the stoma. The patient wears a bag to collect the urine.
For continent cutaneous diversion, a pouch is constructed out of portions of the small and large intestine; the ureters are connected to the pouch and a stoma is created through the abdominal wall. Urine is removed by inserting a thin tube (catheter) into the stoma when the pouch is full. Alternatively, a similar pouch called a neobladder may be created, attached to both the ureters and the urethra, in an attempt to preserve as close to normal bladder function as possible.
Diagnosis/Preparation
The medical team will discuss the procedure and tell the patient where the stoma will appear and what it will look like. The patient will receive instruction on caring for a stoma and bag. A period of fasting and an enema may be required.
Aftercare
After the operation, the patient is given fluid-based nutrition until the intestines begin to function normally again. Antibiotics are given to prevent infection. The nature of cystectomy means that there will be major lifestyle changes for the person undergoing the operation. Men may become impotent if nerves controlling penile
Patients are fitted with an external bag that connects to the stoma and collects the urine. The bag is generally worn around the waist under the clothing. It takes a period of adjustment to get used to wearing the bag. Because there is no bladder, urine is excreted as it is produced. The stoma must be treated properly to ensure that it does not become infected or blocked. Patients must be trained to care for their stoma. Often, there is a period of psychological adjustment to the major change in lifestyle created by the stoma and bag. Patients should be prepared for this by their physician.
Risks
As with any major surgery, there is a risk of infection; in this case, infection of the intestine is especially dangerous as it can lead to peritonitis (inflammation of the membrane lining the abdomen). In the case of partial cystectomy, there is a risk of urine leakage from the bladder incision site. Other risks include injury to nearby organs, complications associated with general anesthesia (such as respiratory distress), excessive blood loss, sexual dysfunction, or urinary incontinence (inadvertent leakage of urine).
Normal results
During a successful partial cystectomy, the cancerous or damaged area of the bladder is removed and the patient retains urinary control. A successful simple or radical cystectomy results in the removal of the bladder and the creation of a urinary diversion, with little or no effect on sexual function. Intestinal function returns to normal and the patient learns proper care of the stoma and bag. He or she adjusts to lifestyle changes and returns to a normal routine of work and recreation.
Morbidity and mortality rates
The overall rate of complications associated with radical cystectomy may be as high as 25–35%; major complications occur at a rate of 5%. The rate of radical cystectomy-related deaths is 1–3%. Partial cystectomy has a complication rate of 11–29%. Some studies have placed the rate of cancer reoccurrence after partial cystectomy at 40–80%.
Alternatives
Transurethral resection (TUR) is one method that may be used to treat superficial bladder tumors. A cystoscope (a thin, tubular instrument used to visualize the interior of the bladder) is inserted into the bladder through the urethra and used to remove any cancerous tissue. Non-surgical options include chemotherapy and radiation.
Resources
books
Walsh, Patrick C., et al., editors. Campbell's Urology, 8th edition. Philadelphia: Elsevier Science, 2002.
periodicals
"Bladder Cancer, Part III: Treatment Approaches in Current Practice and in Evaluation." Future Oncology 6, no. 5 (April 30, 2001): 1322–40.
Carrion, Rafael, and John Seigne. "Surgical Management of Bladder Carcinoma." Cancer Control: Journal of the Moffitt Cancer Center 9, no. 4 (October 31, 2002): 284–92.
organizations
American Cancer Society. 1599 Clifton Road NE, Atlanta, GA 30329. (800) ACS-2345. http://www.cancer.org .
Cancer Information Service, National Cancer Institute. Building 31, Room 10A19, 9000 Rockville Pike, Bethesda, MD 20892. (800) 4-CANCER. http://www.nci.nih.gov/cancerinfo/index.html .
other
"All About Bladder Cancer." American Cancer Society, 2003 [cited April 4, 2003] http://www.cancer.org/docroot/CRI/CRI_2x.asp .
"Cancer Facts and Figures, 2002." American Cancer Society, 2002 [cited April 4, 2003] http://www.cancer.org/downloads/STT/CancerFacts&Figures2002TM.pdf .
Eggner, Scott, and Steven Campbell. "Cystectomy, Radical." eMedicine, August 1, 2001 [cited April 4, 2003] http://www.emedicine.com/med/topic3061.htm .
Feng, Adrian H. "Cystectomy, Partial." eMedicine, February 8, 2002 [cited April 4, 2003] http://www.emedicine.com/med/topic3043.htm .
Ries, L. A. G., et al., eds. "SEER Cancer Statistics Review." National Cancer Institute, 2002 [cited April 4, 2003] http://seer.cancer.gov/csr/1973_1999 .
John T. Lohr, PhD Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Cystectomy is performed in a hospital operating room by a urologist, a medical doctor who has completed specialized training in the diagnosis and treatment of diseases of the urinary tract and genital organs.
QUESTIONS TO ASK THE DOCTOR
- Why is cystectomy recommended in my case?
- In the case of radical cystectomy, what other organs/structures will be removed?
- What method of urinary diversion will be performed?
- What non-surgical options are available to me?
- How long after surgery may I resume normal activity?
What is all this, will I be able to concive and carry a full pregnancy.
Meanwhile, my Prolactin levels are 29.9ng/ml with a normal TSH. so am already on treatment for this.
What are the side effects.
In view of all the above, what can you explain in a layman term