Retropubic suspension
Definition
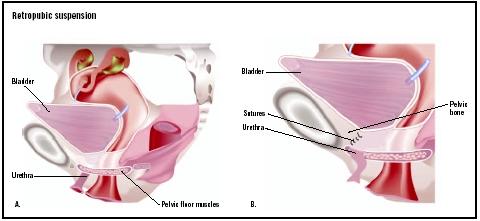
Retropubic suspension refers to the surgical procedures used to correct incontinence by supporting and stabilizing the bladder and urethra. The Burch procedure, also known as retropubic urethropexy procedure or Burch colosuspension, and Marshall-Marchetti-Krantz procedure (MMK) are the two primary surgeries for treating stress incontinence. The major difference between these procedures is the method for supporting the bladder. The Burch procedure uses sutures to attach the urethra and bladder to muscle tissue in the pelvic area. MMK uses sutures to attach these organs to the pelvic cartilage. Laparoscopic retropubic surgery can be performed with a video laparoscope through small incisions in the belly button and above the pubic hairline.
Purpose
The urinary system expels a quart and a half of urine per day. The amount of urine produced depends upon diet and medications taken, as well as exercise and loss of water due to sweating. The ureters, two tubes connecting the kidneys and the bladder, pass urine almost continually and when the bladder is full the brain sends a signal to the bladder to relax and let urine pass from the bladder to the urethra. People who are continent control the release of urine from the urethra via the sphincter muscles. These two sets of muscles act like rubber bands to keep the bladder closed until a conscious decision is made to urinate. The intrinsic sphincter or urethral sphincter muscles keep the bladder closed and the extrinsic sphincter muscles surround the urethra and prevent leakage. Incontinence is common when either the urethra lacks tautness and stability (genuine stress urine incontinence, SUI) and/or the sphincter muscles are unable to keep the bladder closed (intrinsic sphincter deficiency, ISD).
Incontinence occurs in many forms with four primary types related to anatomic, neurological, dietary, or disease, or injury.
Stress incontinence
The most frequent form of incontinence is stress incontinence. This relates to leakage of the urethra with activity that puts stress on the abdominal muscles. The primary sign of stress incontinence is this leakage at sneezing, coughing, exercise, or other straining activities, which indicates a lack of support for the urethra due to weakened muscles, fascia, or ligaments. Pressure from the abdomen with movement, like exercising, uncompensated by tautness or stability in the urethra, causes the urethra to be displaced or mobile leading to leakage. Essentially, this hypermobility of the urethra is an indication that it is moving down or herniating through weakened pelvic structures.
To diagnose incontinence and determine treatment, three grades of severity for stress incontinence are used.
- Type I: Moderate movement of the urethra, with no hernia or cystocele.
- Type II: Severe or hypermobility in the urethra of more than 0.8 in (2 cm), with or without decent of the urethra into pelvic structures.
- Type III: Hypermobility of the urethra where the primary source of incontinence is the inability of the sphincter muscles to keep the bladder closed. This is due to weakness or deficiency in the intrinsic sphincter muscles.
Urge incontinence
Urge incontinence relates to the frequent need to urinate and may involve going to the bathroom every two hours. Accidents are common when not reaching a bathroom
Mixed incontinence
Mixed incontinence is a combination of stress incontinence and urge incontinence, especially in older women. Since each form of incontinence pertains to different functions or anatomy, it is very important to distinguish which part of the incontinence is to be treated by surgery.
Overflow incontinence
Overflow incontinence results in leakage from a bladder that never completely empties due to weakened bladder muscles. Overflow incontinence is involuntary and not accompanied by the urge to urinate. Many causes exist for overflow incontinence, including weak bladder muscles due to diabetes, nerve damage, or a blocked urethra. Men are more frequently affected than women.
Demographics
Over 15 million Americans have urinary incontinence and women comprise 85% of all cases. It affects 25% of women of reproductive age and 50% of women past menopause. Due to the female anatomy, women have twice the risk for stress incontinence compared to men. In addition, childbirth places pressure and burden on the pelvic muscles that often weaken with age, thereby weakening urethra stability. Women are more prone to surgeries for urological changes than men and severe urinary incontinence is often associated with these surgeries as well as hysterectomies. The majority of women with incontinence have stress incontinence or mixed incontinence. Male incontinence occurs primarily in response to blockage in the prostate or after prostate surgery. It is usually treated with implants and/or an artificial sphincter insert.
Description
There are a variety of retropubic suspension surgeries available to treat stress incontinence. The variations differ by the types of structures used to support the urethra and bladder. In all procedures, parts of the pelvic anatomy (pubic bone, ligaments) serve as an anchor or wall upon which the urethra is tacked for stability. The surgery is called a suspension surgery because it stabilizes the urethra from tilting by suspending it against a part of the pelvic anatomy. The Burch procedure is often performed when other surgery is needed such as repair of the urethra for cystoceles and urethral reconstruction. However, this procedure is the most difficult of the anti-incontinent surgeries and is more common in mild forms of stress incontinence where intrinsic sphincter deficiency is not present.
The Burch procedure can be done through open abdominal surgery, which requires a long incision at the bikini line, or surgery performed through the vagina. The patient, in stirrups, receives general anesthesia. Within the retropubic area, the anterior vaginal wall is separated from the bladder manually. The bladder neck is identified and old adhesions or fatty tissues are removed. The neck of the bladder is sutured to pubic ligaments where it will form adhesions and thereby gain stability. The surgeon examines for bladder injury and the surgery is completed. Urethral position is tested by placing a cotton-tipped swab in the urethra and measuring the angle. With abdominal surgery or vaginal surgery a catheter may be put in place by the surgeon for postoperative voiding and to decrease the risks of infection. A suction drain may be placed in the retropubic space for bleeding. The drain is removed one to three days after surgery.
Recently, laparoscopic surgery has been used to perform retropubic suspensions. Laparoscopic surgery requires only three or four 0.25-in (0.6-cm) incisions in the belly button, pubic hairline, or groin area and uses small instruments without opening the abdominal cavity. Shorter healing time is involved with this procedure, the hospital stay is usually not more than 24 hours and recovery to normal activities takes about seven to 14 days. However, the Burch procedure performed using laparoscopic techniques requires great skill on the part of the surgeon and research indicates that the results may not be as long lasting as those developed with abdominal or vaginal surgery.
Diagnosis/Preparation
A patient with incontinence may have multiple factors that induce transient or chronic incontinence. It is crucial that the physician obtain a complete history, physical, clinical, neurological, and medication evaluation of the patient, as well as a radiographic assessment before continuing urological tests aimed at a surgical solution. The specific indications for the Burch colosuspension procedure or its variants is the correction of stress urinary incontinence. This can be a patient who also requires abdominal surgery that cannot be performed vaginally, like hysterectomy or sigmoid surgery, as well as patients who have SUI without ISD.
A urodynamic study with a point pressure leak test will allow a diagnosis to be made that can distinguish the patient who has a hypermobile urethra from the patient who also has ISD. The point pressure leak test, also known as the Valsalva leak test, measures the amount of abdominal pressure required to induce leakage. The patient is asked to cough or strain in order to encourage leakage. The point at which the patient leaks helps determine if stress incontinence with ISD contribution is present. Obese patients and patients that engage in high impact exercise regimens are not considered good candidates for retropubic suspension.
Aftercare
Patients with open retropubic procedures are given pain medication postoperatively that is tapered down over the next two days. A suprapubic catheter stays in place for approximately five days with voiding difficulties encountered initially in many patients. Patients with laparoscopic suspensions are reported to have less blood loss during surgery, less postoperative narcotic requirements, and shorter hospital stays. Patients are expected to refrain from strenuous activity for three months and to have a follow-up visit within three weeks after surgery.
Risks
As with any major abdominal or pelvic surgical procedures, complications that may occur after a retropubic suspension include bleeding; injury to the bladder, urethra, and ureters; wound infection; and blood clots. Specific to the Burch procedure are complications that involve urethral obstruction because of urethral kinking due to elevation of the vagina or bladder base. Postoperative voiding difficulties are common and depend upon the suture tension of the urethral axis. Corrective surgery and the release of the urethra to a more anatomic position resolves voiding issues with a very high rate of success. Vaginal prolapse is also a risk of this procedure.
Normal results
The patient can expect more than 80–90% cure or great improvement in their incontinence. There is a large body of literature documenting the success of the Burch procedure. Published research shows a cure rate ranging from 63–93%, according to the actual version of colosuspension used. Laparoscopic surgery has not produced the long term results that open surgery has and there is the possibility that the fibrosis (adhesion) necessary for a successful outcome does not occur as easily with the laparoscopic procedure. Patients not carefully screened out for ISD will not have a high level of success with the Burch procedure since the source of the incontinence will not have been treated. Sling procedures are recommended for patients with ISD instead of colosuspension surgery.
Morbidity and mortality rates
The Burch procedure may aggravate vaginal wall weakness or vaginal prolapse. This incident varies between 3% and 17%. Research on the Marshall-Marchetti-Krantz procedure pertaining to 2,712 patients found a complication rate of 21%, with wound complications and infections making up the majority, 5.5% and 3.9% respectively. Direct wound injury occurred in 1.6% and obstructions in 0.3% overall.
Alternatives
General or simple severe stress incontinence related primarily to weakening of the urethral support can be remedied with changes in diet, weight loss, and certain behavioral and rehabilitative measures. These include:
- Regular, daily exercising of the pelvic muscles called Kegel exercises, requiring 30–200 contractions a day for eight weeks.
- Biofeedback to gain awareness and control of pelvic muscles.
- Vaginal weight training in which small weights are inserted in the vagina to tighten vaginal muscles.
- Mild electrical stimulation to increase contractions in pelvic muscles.
- Bladder retraining in which the patient is taught how to resist the urge to urinate and expand the intervals between urinations.
There are also medications that can facilitate continence for those experiencing stress or urge incontinence. These include some kinds of antidepressants, although the mechanism of action is not quite understood, as well as antispasmodic medication and estrogen therapy. Finally, should behavioral, rehabilitative, and surgical procedures fail, there remain alternatives through the use of vaginal cones and urethral plugs that can be inserted and removed by the patient.
See also Needle neck suspension ; Sling procedure .
Resources
books
Walsh, Patrick. Campbell's Urology. 8th ed. Elsevier Science, 2000.
periodicals
Liu, C. Y. "Laparoscopic Treatment of Stress Urinary Incontinence." Obstetrics and Gynecology Clinics of North America 26, no. 1 (March 1999): 149-67.
Melton, Lisa. "Targeted Treatment for Incontinence Beckons." Lancet 359, no. 9303 (January 2002): 326.
Smoger, S. H., T. L. Felice, and G. H. Kloecker. "Urinary Incontinence Among Male Veterans Receiving Care in Primary Care Clinics." Annals of Internal Medicine 132, no. 7 (April 4, 2000): 547-551.
Stoffel, J. T., J. Bresette, and J. J. Smith. "Retropubic Surgery for Stress Urinary Incontinence." Urologic Clinics of North America 29, no. 3 (August 2002).
Weber, A. M., and M. D. Walters. "The Burch and Sling Procedures are Similarly Effective for Surgical Treatment of Genuine Stress Urinary Incontinence." Evidence-based Obstetrics & Gynecology 4, no. 1 (March 2002).
organizations
American Foundation for Urologic Diseases. The Bladder Health Council, 1128 North Charles Street, Baltimore, MD 21201. (410) 468-1800. http://www.afud.org/education/bladder.html .
National Kidney and Urologic Diseases Information Clearinghouse. 3 Information Way, Bethesda, MD 20892-3580.
(800) 891-5390 or (301) 654-4415. http://www.niddk.nih.gov .
The Simon Foundation for Continence, P.O. Box 835, Wilmette, IL 60091. (800) 23-SIMON or (847) 864-3913. http://www.simonfoundation.org .
other
Bladder Control in Women. National Kidney and Urologic Disease Information Clearinghouse. NIH Publication no. 97-4195. May 2002 [cited May 12, 2003]. http://www.niddk.nih.gov/health/urolog/uibcw/bcw/bcw.htm .
Ginsberg, David. "Trends in Surgical Therapy for Stress Urinary Incontinence." American Urological Association 97th Annual Meeting, WebMD Conference Coverage. 2002 [cited May 12, 2003]. http://www.medscape.com/viewarticle/437091 .
Hendrix, Susan L., and S. Gene McNeeley. "Urinary Incontinence and Menopause: Update on Evidence-Based Treatment." Medscape, October 28, 2002 [cited May 12, 2003]. http://www.medscape.com/viewprogram/2052 .
Nancy McKenzie, PhD
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Retropubic suspension procedures are performed by a urological surgeon specially trained in incontinence surgeries. Surgery is performed in a general hospital.
QUESTIONS TO ASK THE DOCTOR
- Which retropubic suspension procedure is recommended?
- What is your cure rate with this procedure?
- What is your injury rate for this procedure?
- Could my incontinence be treated just as well with the sling procedure?
- Do you perform laparoscopic surgeries to treat incontinence?