Pectus excavatum repair
Definition
Pectus excavatum repair, also called "funnel chest repair" or "chest deformity repair," is a type of surgery performed to correct pectus excavatum, a deformity of the front of the chest wall with depression of the breast-bone
(sternum) and rib (costal) cartilages. It is sometimes associaated with Marfan or Poland syndromes.
Purpose
The chest consists of the rib cage and sternum, which protect the upper-abdominal cavity and its contents. Pectus excavatum, also called "funnel chest" or "depressed sternum" is a deformity that is usually diagnosed shortly after birth. In some people, it is not visible until they are older. The exact cause is not known, but it is believed to be due to overgrowth of the rib cartilage connected to the sternum, which results in the sternum being pushed backward toward the spine. Most people have no symptoms, but if the breastbone is pushed back far enough, heart and lung function may be affected. The purpose of pectus excavatum repair surgery is to correct the deformity to improve physical appearance, posture, and breathing.
Demographics
In the United States, pectus excavatum is the most common chest wall deformity observed in children, occurring more commonly in boys than in girls. Pectus excavatum tends to run in families. The funnel chest usually progresses as the child grows, often showing a dramatic deterioration during the puberty growth spurt.
Pectus excavatum repair is technically easiest to perform in preadolescent children, and the recovery is faster. However, almost half of the patients undergoing the operation are teenagers. Repair is rarely performed on children under eight years of age. In recent years, a large number of adults over the age of 21 years have undergone repair with equally good results as those observed with children.
Description
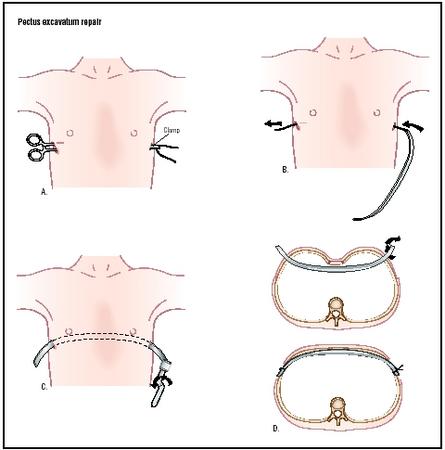
Pectus excavatum repair is always performed with the patient under general anesthesia. An epidural catheter is inserted for the management of pain after the operation. The surgeon makes two incisions over the sternum, on either side of the chest, for insertion of a curved steel bar or strut under the sternum. He or she proceeds to remove the deformed cartilages. The rib lining is left in place to allow renewed cartilage growth. The sternum is then repositioned, and the metal strut is placed behind it and brought out through the muscles and skin for future attachment to a brace, which will stay in place six to 12 weeks. The metal strut is fixed to the ribs on either side, and the incisions are closed and dressed. A small steel grooved plate may be used at the end of the bar to help stabilize and fix the bar to the rib. A blood transfusion is not required during surgery. The surgeon may insert a temporary chest tube to re-expand the lung if the lining of the lung is entered.
A variety of surgical procedures are available to repair pectus excavatum.
Nuss procedure
A common technique is the Nuss procedure, developed in 1987 by Dr. Donald Nuss, a pediatric surgeon at Children's Hospital of the The King's Daughters and Eastern Virginia Medical School in Norfolk, Virginia. The procedure is minimally invasive, and results in very little blood loss and short recovery times.
Leonard procedure
Another surgical approach that drastically reduces the time required for surgery is the Leonard procedure, developed by Dr. Alfred Leonard, a Minneapolis thoracic and pediatric surgeon. This operation does not violate the chest, and is combined with a bracing technique.
Diagnosis/Preparation
A pediatrician diagnoses pectus excavatum after observing a child when he or she inhales, exhales, and rests. The pediatrician also calculates the depth of the chest from front to back using x rays of the chest to determine whether the diameter is shorter than average, as is the case with funnel chest. The heart is usually larger and displaced to the left. The pediatrician also evaluates lung capacity using exercise tests and lung scans that can reveal mismatched lungs.
Other diagnostic tests may include:
- Electrocardiogram (ECG or EKG). This test records the electrical activity of the heart, and shows abnormal rhythms (arrhythmias or dysrhythmias).
- Echocardiogram (echo). This test evaluates the structure and function of the heart by using sound waves recorded on an electronic sensor that yields a moving picture of the heart and its valves.
Before surgery, a bone density test is performed to ensure that the patient does not have soft bones that would deform again right after the surgery. After a complete health history is taken, a patient whose condition is considered severe enough to warrant surgery is sent for a CT scan and further evaluation of his or her pulmonary function.
Because of the great variablity of pectus excavatum among those who have it, custom-made bars (or braces) must be used. The brace is a light vest to which the deformity-correcting wire will be attached at surgery. Patients are fitted with the brace prior to surgery.
Aftercare
Usual recovery time in the hospital is four to five days. Attention is paid to post-operative pain management . The patient is encouraged to breathe deeply, and receives assistance with movement (to avoid dislodging the bar). After discharge, the patient slowly resumes a normal, but restricted, activity level. Most children are able to return to school in two to three weeks, with exercise restrictions for six weeks (no physical education classes, heavy lifting, or athletics).
The pectus excavatum support bar is removed under general anesthesia two to four years after insertion, usually on an outpatient basis. In most cases, patients are able to leave the hospital within one to two hours after bar removal.
Risks
Risks associated with pectus excavatum repair include those normally associated with the administration of anesthesia (such as adverse reactions to medications and breathing problems), and risks associated with any surgery (such as bleeding and infection). Specific pectus excavatum surgery risks may include lung collapse (pneumothorax) and the recurrence of the funnel chest. Bar displacement may occasionally require repositioning.
Normal results
Pectus excavatum repair, in almost all instances, restores the ability of patients to participate in full activities, even strenuous activities and athletics. Also, there is a marked improvement in the patient's self image.
Morbidity and mortality rates
According to the National Institutes of Health (NIH), excellent results (95–98%) are reported over a lengthy follow-up time of 25 years. Long-term follow-up (over 15 years) shows that the Nuss procedure provides excellent results with less than 5% recurrence of the deformity after the bar is removed.
Alternatives
Mild cases of pectus excavatum may respond to an exercise and posture physiotherapy program. Many patients with rounded shoulders and a slouching posture have benefited from these techniques, with or without additional surgical correction. However, body-building exercises usually result in worsening of cosmetic appearance due to the enhancement of the pectoral muscles.
Resources
books
Pearson, F. G. Thoracic Surgery. Philadelphia: W. B. Saunders Co., 2002.
Ravitch, M. M. Congenital Deformities of the Chest Wall and Their Operative Correction. Philadelphia: W. B. Saunders Co., 1977.
periodicals
Engum, S., F. Rescorla, K. West, T. Rouse, L.R. Scherer, and J. Grosfeld. "Is the Grass Greener? Early Results of the Nuss Procedure." Journal of Pediatric Surgery 35 (2000): 246-51.
Genc, A., and O. Mutaf. "Polytetrafluoroethylene Bars in Stabilizing the Reconstructed Sternum for Pectus Excavatum Operations in Children." Chest 110 (July 2002): 54-7.
Hebra, A., B. Swoveland, M. Egbert, E.P. Tagge, K. Georgeson, H.B. Othersen, and D. Nuss. "Outcome Analysis of Minimally Invasive Repair of Pectus Excavatum: Review of 251 Cases." Journal of Pediatric Surgery 35 (2000): 252-7.
Jacobs, J. P., J.A. Quintessenza, V.O. Morell, L.M. Botero, H.M. van Gelder, and C. I. Tchervenkov. "Minimally Invasive Endoscopic Repair of Pectus Excavatum." European Journal of Cardiothoracic Surgery 21 (2002): 869-83.
organizations
American Pediatric Surgical Association (APSA). 60 Revere Drive, Suite 500, Northbrook, IL 60062. (847) 480-9576. http://www.eapsa.org .
Southern Thoracic Surgical Association. 633 N. Saint Clair St., Suite 2320, Chicago, IL, 60611-3658. (800) 685-7872. http://www.stsa.org/ .
other
"Pectus Excavatum Repair." BestHealth. http://www.besthealth.com/surgery/PectusExcavatumRepair_1.html .
Monique Laberge, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Pectus excavatum repair is performed in a hospital by experienced thoracic surgeons who specialize in pectus excavatum repair.
QUESTIONS TO ASK THE DOCTOR
- Can exercises correct pectus excavatum?
- How is pectus excavatum surgery performed?
- Should everyone with pectus excavatum have surgery?
- What surgical procedures does the doctor use?
- How many pectus excavatum surgeries does the physician perform each year?
what would determine which prodecure a patient should undergo?
Thanks
i have a sternum that is also pushed in about 3/4 inch down. What could I do to make it go away...exercises? surgery? I am 14 years old and I noticed it only about a year ago. Thank you, and please contact me.
I have pectus excavatum as well..I first noticed it in puberty and I am 22 right now. I never worried about it because I always thought I would be able to 'fix' through exercise, since I am in to weightlifting and combat sports. But the truth of the matter is that the disorder only got worse.. I'm now thinking of getting surgery, but I am not sure because there is no physical need for it..it would be just for me to feel better in my own skin..Cheers
Thank you,
Many Thanks
James
Regards
Ray Flores
thanks for any resources or info u can supply me!!!
hanxx
He needs to find a surgeon that is experienced and preferably in Colorado but willing to go elsewhere for a more experience Doctor in repairing pectus excavatum. Please help us find the right procedure and the best Doctor for this procedure. Thanks so much for your advice. If anyone has any ideas or advice, I would love to hear from you. My email is: koalamsa@yahoo.com Thanks again.
Growing up I was always getting respitory infections, I would have broncittis atleast twice a year. In high school I started heavy into sports and even though I was busting my butt I could never keep up and worn down easy. When I was sick breathing would be hard. I actually grew up thinking my chest was supposed to be sunk in I never noticed it until I was changing in the locker room and other noticed. I also used to get severe chest pains.
We finally looked into a solution when I failed my sports physical for cross country. That's when we found i had a severe case, my sternum was centimeters away from my spine and my heart was displaced and one lung slightly collapsed. I had the surgery and it took well over a year to be able to play sports again, but never contact sports. It's now eight years later and my chest is stil stiff. But I can breather easier and I'm not sick nearly as much. I never regained my running endurance back so it all depends what you want to get out of surgery. I still have the bar in they never took it out or told me to take it out. I will say it took a few years but I'm getting chest pains again, not as severe though so I'm dealing with it.
My advice, if it's not physically bothering you don't fix it!! This is no walk in the park surgery. If you can live with the way you look don't fix it. This is a major surgery.
Now I can't tell you what procedure I had, all I know is they compared it to open heart surgery but without touching the heart. I know I have a Titanium bar in me, I think it's the Ravitch Procedure but I have a very long verticle inscion down my chest. They broke my sternum and some ribs to reset it in the correct position. But I was a high schooler and all I cared about was being able to look better, not be sick, and play sports again. So I wasn't always listening.
Hope this gives some insight on my experience.
It wasn't until I was around 15 when I started to feel a difference, although I had been able to see one for a while. I had what was commonly known as pigeon chest, where the sternum was actually raised a bit and protruding from my chest. As a member of my high school track team I noticed breathing problems, slight pains, and shortness of breath was above normal. When I went to the doctor, I was told the chest deformity might be the cause of these slight heart palpitations, and that It could cause me problems down the line.
I found a surgeon who acted like this was standard practice and although I was slightly out of her age range 8-16 (I was now 19) It was decided that this would be the best solution. Immediately after coming out of the anesthesia my family and I noticed the extreme beating of my heart right through my skin as if the two were separated only by a thin piece of paper. When asked about this, the doctor said it was completely normal. It wasn't for another couple months, when the pain didn't seem to go away I started asking questions. The doctor became very hard to reach all of the sudden. She was short and distant when I did talk to her, almost realizing the mistake. She advised me that we wouldn't know anything for at least a year, which low and behold to me was when the statue of limitations would run out, releasing her of most liability.
Doctor's aren't always as we might like to believe they are. Like your mechanic, they too make mistakes and may try to cover them up.
I'm not writing this to warn you of crooked doctors although it is to be noted especially by some of the younger crowd on here looking for a cosmetic fix, but instead to share with you what my like is like now.
I have had three repair operations to fix this mistake. A standard "bar" procedure was not used in my case. She left me with whats called a flayed chest. The sternum not connected to the ribs by cartilage leaves two separated pieces which move freely of one another and cause me a significant amount of pain constantly. I have learned to sleep again over the years, and how to sit in cars.
I am by normal standards physically disabled, and still looking for a fix. I have juggled jobs, and school unsuccessfully up until now. I am on high doses of pain medicine and sleep very little. I write to inform the uninformed of what kind of complications and risk are involved in this surgery. My recommendation is to do a lot of research to find the very top doctor money can buy if you decide to undertake this surgery. This isn't a walk in the park. If the surgery is successful I would plan on being in bed for at least a couple months and expect serious pain. Good luck, and remember that if this is strictly cosmetic, it is probably not worth the risk. Besides, our differences are what set us apart and give us character.
Noah
i have Pectus excavatum and it goes in about one inch is that considered minor or severe and it hasn't effected me in any way such as sports and breathing and i don't want to go through all the surgeries ad pain just to make it normal if i doesn't effect my health thanks please reply
1. Is it possible for me to still get corrective surgery at my age
2. Which procedure would be the best option?
3. Is there a surgeon in South Africa that can perform the surgery
4. What would the cost involved be?
Hope to get a reply soon.
Thanks
I am sorry to hear. God bless all of you, I wish you the BEST!
I had a stress test done a few years back that they said didn't show anything. I have become frustated trying to find a doctor that even knows anything about pectus. From previos xrays it looks as if my heart is located pretty much center between my breast bone and spine, I can pretty much fit my fist in the concave area, so I wouldn't call it mild. I had one instance where I was prescribed a anti depressant that made my heart race all day, which in turn caused brusing that made me suffer for 2 weeks. (they told me the lining of my heart was bruised from beating against my sternum all day) This was from 1 pill! Can you help with finding a knowledgeable doctor in Ohio, I know that the Cleveland Clinc has them, but I was hoping for someone maybe closer to Columbus, OH. Thanks
A bit conerned Mother, not keen for surgery. He dosn't like it and is embarrassed about it.
Thanks
Karen
I am 15 and was born with Pectus Excavatum. i was wondering how much it is to get any of the surgery's? i live in Australia. I never had breathing problems before when i had it but now i am starting to get breathing problems with it and sometimes i think it gives me pain in my chest next to the heart. i am also scared to take my shirt off when i am at the beach or pool because of Pectus Excavatum. Any advice really appreciated.
im living testament the Dr Nuss precedure does work , i too used to get funny looks when on the beach people contantly telling me to not bend my back, football coaches telling me im to skinny ,
but this process really does work and is worth the pain i wont lie it did hurt but in the long run is so much better i feel i now have a normal life ( not that it affected my breathing or health)
but it was purely cosmetic , since having it done when i was 18 now 27 i have gained more confidence in myself go gym regularly and have bulk up considerably only showing 4 small scars on my body
looking at these pictures its easy to forget how far we all can come you just have to trust and beleive .. i was monents away from pulling out as they didnt have a bed at great ormond street and got so upset .. but im now so glad i went through with it
so anybody out there doubting if its the right thing to do from my expereince i would say go for it !
I would appreciate any comments while she is going through this.
It goes in about 1-2 inches and well im not sure if it's effecting me yet, im no doctor. Looking though these comments and page made me think of getting the surgery and it sounds good, i was just wondering about the details and such for the picture at the top of the page, the one where the male i think gets a brace to hold up/support his chest/breast plate on the inside?
My questions are:
1) How much would it cost for this surgery?
2) As i live in Australia-Wa, does anyone know of a doctor that could perform this operation ? Rather it be in one of these places "Perth" "Bunbury" "Busselton"
3) I play Football (AFL) would this effect me in anyway after the operation?
4) Besides the surgery is their anyway i can get this pigeon chest to go away? return to normal?
5)Cost? (asking again because i need to know this one)
Email any answers or questions to me, i'm very keen for this abnormal chest to go away
email address: l7aniel@hotmail.com
Instead of using less invasive Nuss procedure (my surgeons claims such a strategy is not safe), he applied Ravitch procedure on my chest. My chest was opened up, four pairs of deformed cartilages were removed, the lower part of my sternum was bent outward. However, rather than placing a metal bar under my sternum, he used stitches to fixate it.
Shortly after the operation, a bit of the cartilages grew quickly, while the majority was still stagnant. At this stage, two years have gone, and none of the cartilages (fully) re-grows. Consulting the advice from my own surgeon and other doctors, they quite unanimously state that my cartilages are not likely to grow back, which is fairly devastating to me.
A doctor suggests that by placing two Nuss bars in my chest, and biological patches if necessary, my floating sternum will be stabilized and the cartilages will grow back once my chest wall remains steady. Yet, some other doctors cast doubts on such a way and play down the chance of cartilages regrowth.
Since my surgeon claims that even without the cartilages I can still live my life as usual as normal people, I don’t think he would do anything more to help with my full recovery. Therefore, I would like to consult your advice on my situation, as I am willing to give it a bet for any possible ways of cartilages regrowth.
I hope you get your chest sorted out soon and with as little pain as possible.
Im 15 year old male,
I have went through a pectus excavatum repair during the summer but at this point i was 14 and everything was fine, was put on a morphine drip so i didnt feel any pain. The result is unbelievable and im so happy i went through it. The down side is that about a month after i had the opperation done 2 lump started to develope on my chest, they bleed constantly and puss even comes out, there really really sore, iv been to my GP and they gave me a week of anitbiotics but it didnt help, they had 3 different doctors in looking at my chest because they never came across it before so it had to be something to do with the operation. I went back to hospital to my surgeon and he said it was very rare and that he never came across it before and again he had 3 other surgeons in with him. I was suppose to get them removed today to see whats causing them but the ward i was suppose to be staying in had all of its beds tooken up. The lumps are really painful and i was just wondern is there anyone else that has experienced this after they had a pectus excavatum repair.
thanks sinead
I made a surgery for P.E. 10 years ago.I had a severe deformation for my chest. I made it in Romania. I do not know what procedure they used but I have a scar (22 cm long) on my chest. My pectus was fixed 70%. Still is not perfect but is much better than it was before. Curentlly I'm practicing dance and I am plannig to do kickboxing this year. I am curious if I get a punch in my chest could that be dangerous for me?
I am 26 years old and now I noticed that my chest is little bit out ward and today I felt pain in the chest and right behind it..i don't know what is this.. what should I do?
bennyman2301@hotmail.com if anyone can help me
my one side rib is depressed inside, i noticed it 3 years ago
i dont have any idea to recover it please give me any suggestion