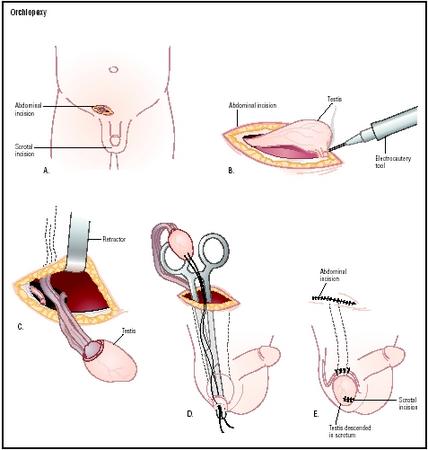
Orchiopexy
Definition
Orchiopexy is a procedure in which a surgeon fastens an undescended testicle inside the scrotum, usually with absorbable sutures. It is done most often in male infants or very young children to correct cryptorchidism, which is the medical term for undescended testicles. Orchiopexy is also occasionally performed in adolescents or adults, and may involve one or both testicles. In adults, orchiopexy is most often done to treat testicular torsion, which is a urologic emergency resulting from the testicle's twisting around the spermatic cord and losing its blood supply.
Other names for orchiopexy include orchidopexy, inguinal orchiopexy, repair of undescended testicle, cryptorchidism repair, and testicular torsion repair.
Purpose
To understand the reasons for performing an orchiopexy in children, it is helpful to have an outline of the normal pattern of development of the testes in a male infant. The gubernaculum is an embryonic cord-like ligament that attaches the testes within the inguinal (groin) region of a male fetus up through the seventh month of pregnancy. Between the 28th and the 35th week of pregnancy, the gubernaculum migrates into the scrotum and creates space for the testes to descend. In normal development, the testes have followed the gubernaculum downward into the scrotum by the time the baby is born. The normal pattern may be interrupted by several possible factors, including inadequate androgen (male sex hormone) secretion, structural abnormalities in the boy's genitals, and defective nerves in the genital region.
Orchiopexy is performed in children for several reasons:
- To minimize the risk of infertility. Adult males with cryptorchidism typically have lower sperm counts and produce sperm of poorer quality than men with normal testicles. The risk of infertility rises with increasing age at the time of orchiopexy and whether both testicles are affected. Men with one undescended testicle have a 40% chance of being infertile; this figure rises to 70% in men with bilateral cryptorchidism.
- To lower the risk of testicular cancer. The incidence of malignant tumors in undescended testes has been estimated to be 48 times the incidence in normal testes. Men with cryptorchidism have a 10% chance of eventually developing testicular cancer.
- To lower the risk of traumatic injury to the testicle. Undescended testicles that remain in the patient's groin area are vulnerable to sports injuries and pressure from car seat belts.
- To prevent the development of an inguinal hernia. An inguinal hernia is a disorder that occurs when a portion of the contents of the abdomen pushes through an abnormal opening in the abdominal wall. It is likely to occur in a male infant with cryptorchidism because a sac known as the processus vaginalis, which connects the scrotum and the abdominal cavity, remains open after birth. In normal development, the processus vaginalis closes shortly after the testes descend into the scrotum. If the sac remains open, a section of the child's intestine can extend into the sac. It may become trapped (incarcerated) in the sac, forming what is called a strangulated hernia. The portion of the intestine that is trapped in the sac may die, which is a medical emergency.
- To prevent testicular torsion in adolescence.
- To maintain the appearance of a normal scrotum. Orchiopexy is considered a necessary procedure for psychological reasons, as boys with only one visible testicle are frequently subjected to teasing and ridicule after they start school.
The primary reason for performing an orchiopexy in an adolescent or adult male is treatment of testicular torsion, rather than cryptorchidism. Testicles that have not descended by the time a boy reaches puberty are usually removed by a complete orchiectomy .
Demographics
Cryptorchidism
Cryptorchidism is the most common abnormality of the male genital tract, affecting 3–5% of full-term male infants and 30–32% of premature male infants. In most cases, the condition resolves during the first few months after delivery; only 0.8% of infants over three months of age still have undescended testicles. Because of the potentially serious consequences of cryptorchidism, however, doctors do not advise watchful waiting once the child is over six months old. Undescended testicles
Cryptorchidism is a frequent occurrence in prune belly syndrome (PBS) and a few other genetic disorders characterized by structural abnormalities of the genitourinary tract.
No variation in the incidence of cryptorchidism among different racial and ethnic groups has been reported.
Testicular torsion
Most American males suffering from testicular torsion are below age 30, with the majority between the ages of 12 and 18. The peak ages for an acute episode of testicular torsion are the first year of life and age 14. Testicular torsion occurs on the left side of the body slightly more often than on the right side, about 52% versus 48% of cases.
Description
Cryptorchidism
Some orchiopexies in children are relatively simple procedures; however, others are complicated by the location of the undescended testicle. In general, an orchiopexy for an undescended testicle that lies in front of the scrotum or just above it is a less complicated operation than one done to treat a non-palpable testicle. The procedure is usually done under general anesthesia.
If the undescended testis is in the groin area, the surgeon will make a small incision in the groin and a second small incision in the scrotum. The testis is moved downward from the groin without complete separation from the gubernaculum. It is then placed inside a small pouch created by the surgeon between the skin of the scrotum and a layer of muscle in the scrotum called the dartos muscle. The testicle is held in place with sutures that are eventually absorbed by the body.
The Fowler-Stephens technique is often used when the undescended testicle is located high above the scrotum or in the abdomen. It may be done in two stages scheduled several months apart. In the first stage, the surgeon moves the testicle downward and attaches it temporarily to the inside of the thigh. In the second stage, the testicle is transferred into the scrotum itself and sutured into place.
A third type of orchiopexy is called testicular auto-transplantation. The surgeon removes the undescended testicle completely from its present location and re-implants it in the scrotum by reattaching its surrounding tissues and blood vessels to nearby blood vessels. This technique minimizes the risk of an inadequate blood supply to the re-implanted testicle.
Testicular torsion
An orchiopexy done to treat testicular torsion is usually done under general or epidural anesthesia. The surgeon makes an incision in the patient's scrotum and untwists the spermatic cord. The affected testicle is inspected for signs of necrosis, or tissue death. If too much tissue has died due to loss of blood supply, the surgeon will remove the entire testicle. If the tissue appears to be healthy, the surgeon sutures the testicle to the wall of the scrotum and then closes the incision. In most cases, the surgeon will also attach the unaffected testicle to the scrotal wall as a preventive measure.
Diagnosis/Preparation
Cryptorchidism
The diagnosis of cryptorchidism is usually made when a pediatrician examines the newborn baby, although the condition can occur at any time before the boy reaches puberty. The first stage in diagnosis is an external physical examination of the child's genitals. If either testicle does not appear to be in the scrotum, the doctor will palpate, or touch, the groin area and abdomen to determine whether a testicle can be felt in any of those locations. If the testicle can be felt, the doctor will decide on the basis of its location whether it is an undescended testicle, a so-called ectopic testicle, or a retractile testicle. An ectopic testicle is one that has developed in a location outside the normal path of development in the inguinal canal. Ectopic testicles are most often discovered along the inner part of the thigh near the groin, at the base of the penis, or below the scrotum in the perineum (the area between the scrotum and the rectum). A retractile testicle is one that is readily pulled back out of the scrotum by an overly sensitive reflex called the cremasteric reflex; it is not a genuinely undescended testicle. It is important for the doctor to distinguish a retractile testicle from genuine cryptorchidism because retractile testicles do not need surgical treatment. At this point in the diagnostic workup, a general pediatrician will often consult a specialist in pediatric urology.
In about 20% of male infants with cryptorchidism, the missing testicle cannot be felt at all. It is known as a non-palpable testicle. The child may be given a hormone challenge test to help determine whether the testicle is located in the abdomen or whether it has failed to develop fully. If the testosterone level in the blood rises in response to the test, the doctor knows that there is a testis present somewhere in the child's body. In other cases, the testis has atrophied, or shriveled up due to an inadequate blood supply before birth. If neither testicle can be felt, the child should be examined further for evidence of inter-sexuality. The doctor may order an ultrasound to check for the presence of a uterus, particularly if the child's external genitals are ambiguous in appearance.
Surgery is the next step in searching for a non-palpable testicle. The surgeon may perform either an open inguinal procedure or a laparoscopic approach. In an open inguinal exploration, the surgeon makes an incision in the child's groin; if nothing is found, the incision may be extended into the lower abdomen. In a laparoscopic approach, the surgeon uses an instrument that looks like a small telescope with a light attached in order to see inside the groin or the abdominal cavity through a much smaller incision. If the surgeon is able to find the testicle, he or she may then proceed directly to perform an orchiopexy.
Testicular torsion
Testicular torsion is usually diagnosed in the emergency room. The doctor will usually suspect testicular torsion on the basis of sudden onset of severe pain on one side of the scrotum; it is unusual for pain to develop gradually in this disorder. The patient's history often indicates recent hard physical work, vigorous exercise , or trauma to the genital area; however, testicular torsion can also occur without any apparent reason. Other symptoms may include swelling of the scrotum, blood in the semen, nausea and vomiting, pain in the abdomen, and fever. A few patients feel the need to urinate frequently. When the doctor examines the patient's scrotum, the affected testicle is usually enlarged and is painful when the doctor touches it. It usually lies higher in the scrotum than the unaffected testicle and may be lying in a horizontal position.
Since testicular torsion is a medical emergency, most doctors will not risk permanent damage to the testicle by taking the time to perform imaging studies. If the diagnosis is unclear, however, the doctor may order a radionuclide scan or a color Doppler ultrasound to determine whether the blood flow to the testicle has been cut off. The patient will be given a mild pain medication and referred to a urologist for surgery as soon as possible.
Aftercare
Cryptorchidism
Aftercare in children depends partly on the complexity of the procedure. If the child has an uncomplicated orchiopexy, he can usually go home the same day. If the surgeon had to make an incision in the abdomen to find a non-palpable testicle before performing the orchiopexy, the child may remain in the hospital for two or three days. The doctor will usually prescribe a pain medication for the first few days after the procedure.
After the child returns home, he should not bathe until the day after surgery. In addition, he should not ride a bicycle, climb trees, or do anything else that requires straddling for two or three weeks. An older boy should avoid sports or rough games that might result in injury to the genitals until he has a post-surgical checkup.
Most surgeons will schedule the child for a checkup one or two weeks after the orchiopexy, with a second checkup three months later.
Testicular torsion
Aftercare is similar to that for orchiopexy in a child. The area around the incision should be washed very gently the next day and a clean dressing applied. Medication will be prescribed for postoperative pain. The patient is advised to rest at home for several days after surgery, to remain in bed as much as possible, to drink extra fluids, and to elevate the scrotum on a small pillow to ease the discomfort. Vigorous physical and sexual activity should be avoided until the pain and swelling go away.
Risks
Cryptorchidism
The risks of orchiopexy in treating cryptorchidism include:
- infection of the incision
- bleeding
- damage to the blood vessels and other structures in the spermatic cord, leading to eventual loss of the testicle
- failure of the testicle to remain in the scrotum (This problem can be repaired by a second operation.)
- difficulty urinating for a few days after surgery
Testicular torsion
The risks of orchiopexy as a treatment for testicular torsion include:
- infection of the incision
- bleeding
- loss of blood circulation in the testicle leading to loss of the testicle
- reaction to anesthesia
Normal results
In a normal orchiopexy, the testicle remains in the scrotum without re-ascending. If the procedure has been successful, there is no damage to the blood vessels supplying the testicle, no loss of fertility, and no recurrence of torsion.
Morbidity and mortality rates
Cryptorchidism
Orchiopexy is most likely to be successful in children when the undescended testicle is relatively close to the scrotum. The rate of failure for orchiopexy performed as a treatment for cryptorchidism is 8% if the testicle lies just above the scrotum; 10–20% if the testicle is located in the inguinal canal; and 25% if the testicle lies within the abdomen.
Testicular torsion
The mortality rate for orchiopexy in adults is very low because almost all patients are young males in good health. The procedure has a 99% rate of success in saving the testicle when the diagnosis is made promptly and treated within six hours. After 12 hours, however, the rate of success in saving the testicle drops to 2%. The average rate of testicular atrophy following orchiopexy for testicular torsion is about 27%.
Alternatives
Cryptorchidism
Hormonal therapy using gonadotropins to stimulate the production of more testosterone is effective in some children in causing the testes to descend into the scrotum without surgery. This approach, however, is usually successful only with undescended testes that are already close to the scrotum; its rate of success ranges from 10–50%. Undescended testes that are located higher almost never respond to hormonal therapy. In addition, treatment with hormones has several undesirable side effects, including aggressive behavior.
Some surgeons will, however, prescribe hormonal treatment before an orchiopexy in order to increase the size of the undescended testis and make it easier to identify during surgery.
Testicular torsion
Pain caused by testicular torsion can be relieved temporarily by manual detorsion. To perform this maneuver, the doctor stands at the patient's feet and gently rotates the affected testicle toward the outside of the patient's body in a sidewise direction. Manual detorsion is effective in relieving pain in 30–70% of patients; however, it is not considered an alternative to orchiopexy in preventing a recurrence of the torsion or loss of the testicle.
See also Orchiectomy ; Urologic surgery .
Resources
books
"Congenital Anomalies: Renal and Genitourinary Defects." Section 19, Chapter 261 in The Merck Manual of Diagnosis and Therapy, edited by Mark H. Beers and Robert Berkow. Whitehouse Station, NJ: Merck Research Laboratories, 1999.
periodicals
Baker, L. A., et al. "A Multi-Institutional Analysis of Laparoscopic Orchidopexy." BJU International, 87 (April 2001): 484–489.
Chang, B., L. S. Palmer, and I. Franco. "Laparoscopic Orchidopexy: A Review of a Large Clinical Series." BJU International, 87 (April 2001): 490–493.
Docimo, S. G., R. I. Silver, and W. Cromie. "The Undescended Testicle: Diagnosis and Management." American Family Physician, 62 (November 1, 2000): 2037–2044, 2047–2048.
Dogra, Vikram S., and Hamid Mojibian. "Cryptorchidism." eMedicine, June 21, 2002 [April 4, 2003]. http://www.emedicine.com/radio/topic201.htm .
Franco, Israel. "Prune Belly Syndrome." eMedicine, August 24, 2001 [April 4, 2003]. http://www.emedicine.com/med/topic3055.htm .
Jawdeh, Bassam Abu, and Samir Akel. "Cryptorchidism: An Update." American University of Beirut Surgery, (Summer 2002) [April 3, 2003]. http://www.staff.aub.edu.lb/~websurgp/sc0a.html .
Nair, S. G., and B. Rajan. "Seminoma Arising in Cryptorchid Testis 25 Years After Orchiopexy: Case Report." American Journal of Clinical Oncology, 25 (June 2002): 287–288.
Rupp, Timothy J., and Mark Zwanger. "Testicular Torsion." eMedicine, March 25, 2003 [April 4, 2003]. http://www.emedicine.com/EMERG/topic573.htm .
Sessions, A. E., et al. "Testicular Torsion: Direction, Degree, Duration, and Disinformation." Journal of Urology, 169 (February 2003): 663–665.
Shekarriz, B., and M. L. Stoller. "The Use of Fibrin Sealant in Urology." Journal of Urology, 167 (March 2002): 1218–1225.
Tsujihata, M., et al. "Laparoscopic Diagnosis and Treatment of Nonpalpable Testis." International Journal of Urology, 8 (December 2001): 692–696.
organizations
American Academy of Pediatrics (AAP). 141 Northwest Point Boulevard, Elk Grove Village, IL 60007. (847) 434-4000. http://www.aap.org .
American Board of Urology (ABU). 2216 Ivy Road, Suite 210, Charlottesville, VA 22903. (434) 979-0059. http://www.abu.org .
National Organization for Rare Disorders (NORD). 55 Kenosia Avenue, P. O. Box 1968, Danbury, CT 06813-1968. (203) 744-0100. http://www.rarediseases.org .
Prune Belly Syndrome Network. P. O. Box 2125, Evansville, IN 47728-0125. http://www.prunebelly.org .
Rebecca Frey, PhD
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
A pediatric surgeon or pediatric urologist is the specialist most likely to perform an orchiopexy in an infant or small child. In an adult patient, the procedure is usually performed by a urologist after referral from the patient's primary physician or the emergency care physician.
An orchiopexy can be performed in the surgical unit of a children's hospital or an ambulatory surgical center. Most orchiopexies in adults are performed as outpatient procedures.
QUESTIONS TO ASK THE DOCTOR
- How often have you treated a child for cryptorchidism?
- What are the chances that the treatment will be successful?
- What should I tell my son about the operation?
- Are there likely to be any long-term aftereffects?
My son have one side undcended testies and doctor performed opration when he was 5 months old ,,,now i want to know when the size will be same ,
please reply
waiting for your reply
thanks
Could somebody explain to me or assure to me that the surgery well be alright.
thanks
Could you explain me the risk of infertility for a person who had the surgery of 2 sides undescended testicles (the inguinal canal) as an adult?
i had 2 side undecended testicles but i have been oporated very late when i was 25 now i am 27 years old, tel now my testicles size small and have azoosperma, could someone tell me the fact and advise me in this regard. i shall be thankfull to him
I write as a fellow patient, not a medical professional, but since no one else is answering questions here, I will give my best approximation, based on my understanding as an educated layman:
1)Freeha - The size may or may not be the same at some point. Ask your boy's doctor about this, and tell any new doctor about the issue so he will be aware of the medical history. My own testicles are obviously different sizes, and when I was in my twenties I was offered a cosmetic implant, which I declined.
2)Z. Angel - You may want a simpler explanation of what the problem is and what they will do about it than this article provides. The surgery is medically necessary. Performed by trained and experienced surgeons, the risks are small. The risks of not doing anything, or waiting too long, are larger - sterility (as I have experienced personally) or testicular cancer.
3)na - My orchiopexy was too late to save my fertility. Once a boy who has had an orchiopexy has begun to produce sperm, they can be examined to evaluate his chances to have children. If your orchiopexy was as an adult, you are probably infertile. You should have a fertility evaluation to settle this.
4) Ryan - You should see a doctor, and probably have the undescended testicle either surgically brought down or removed. Chances are your fertility is not affected, but this can be checked.
5)William - Yes, complications are possible.
6)Ali - Like commenter number 3, you are in a similar position to me. You will not be able to have biological children. Adoption or sperm donation for your wife's pregnancy are options. You may also (like me) be prescribed supplemental male hormones.
7) Josie, depending on the location of the testicles, medication may bring them down, or surgery may be necessary. Have this dealt with promptly.
I started to notice this about three week after surgury.
My son is 4 years old. He has 2 side undescended testicles. When he was 5 months he had a surgery but it seems that it wasn't sucssesful. I don't know what to do now. I can't see any changes even if we tried to help him when he was baby. His testicles are still in lower part of abdomen because when I try to make him a simple massage I can't find any sign that the surgery could help.
so, please tell me what to do.
I'm from Kosovo and our health services and examination are not meeting even minimum standards.
I really need your help
sincerely
Myrvete Haxholli
i am 34 years of age and have diagnosed with ultrasound that two of them (testicles) are undescended, right one measures 4.1cm x 2.1cm and left of measures 2.3cm x 1.3cm. i also diagnosed as azoopsermia patient.
with surgery (orchiopexy) both of them can be brought normal and my azoospermia can be treated like this or some hormonal medicines be used.
regards,
Aslam o Alaikum,
We have been married since October 2007 and have no kids yet. We gone through some medical test of both and found that I have azoospermia. After that an ultrasound and hormone test is also carried out.
I am 34 years of age and my wife is 36 years of age.
Ultrasound says that I have both testicles undescended, left one is little deep and measures 2.1cm x 1cm and right one is 4.2cm x 2cm.
Hormone report of testosterone is about 219 points and FSH is 46 points.
Kindly let me know what is possible to have kids.
Kindly reply fast, and if possible give me appointment if u are available in Pakistan.
Regards,
Mian Zahid
Still sometimes the pain comes after sometime a while.
I am 31 years of age, and have bilateral undescendent testicles, both of them are indise,
one near the inguinal ring and the other is hiding due to hernia.
I am married with no chidlren, I am in london, uk, Can you suggest me please any good doctor
who can do this operation carefully to bring them down.
Please let me know
Many thanks
You should imediately see a urologist, and bring both testes down.There is a higher risk for cancer if you let them up and inside.Usually this is done with a surgery.Don't waste more time.
I wish you luck
Alma
but currently my right testicle is swollen to about three qaurters the volume of my scrotum,
my doctor told me it may just be an infection, but im just wondering, what its my risk now of losing a testicle later in life? or how could my fertility have been affected? cause after reading a lot of this im starting to get very worried, my doctor never told me that i could be at risk of losing a testicle, and i feel a bit wronged since hearing that there is the possibility i could lose one in the future. please someone who knows, email me directly jzzulu@hotmail.com
my son going to do orchiopexy SURGERY and his age 8 years i am so scaring about this surgery because the doctor inform me that i am so late this surgery if it done in age 6m-2y it will be safe and may be in 8 years Testicular damage or it will not grow after the surgery
i would like to know a.s.a.p.
1- how i know that testicular damage or not damaged
2- how i know that testicular grow or infected
3- relation between the age for orchiopexy surgery and efficiency of testicular
please help me i lost all my personal peace
Thanks
I am Abhay Had orchiopexy in age of 20th and still the testes are brought from superficial ring of kidney to inguinal canal and now my age is 26 and i want to perform another one orchiopexy and ultrasound is normal in vascularity and echotexture of testes.
so please suggest me whether i should go for surgery or not
and what are the complication i can have after surgery..
im waiting for your reply soon.
I was 11.6 yrs when I had to have urgent surgery as internal bleeding nearly cost me my life.(1957)
I had been diagnosed with bilateral (both) undescended since age 3.6 yrs. I have welfare doctors medical reports.
My Results: experiences.
1. Do not wait to long to get the operation. The older the maore the mind and emotions hang onto the pain.
n those days kept in hospital for 9 days.
Nowadays in and out. Especially as a child its easy.
2. I have fathered 5 children. # males 2 Females. Now 10 Grandchildren.
3. at age 48 had to get vasectomy as the surgeon in those days did not allow for me being a six foot adult in later life.Therefore did not free-up the growth of the tubes well as it is done nowadays.So for the males the procedure is fine, great. get the child done early in lifre.
For prospective mothers. Don't drink alcohol. Alcohol is the cause of the undescended testicles.
remember the featus is female then changes to male. so huge internal changes HAPPENING AND ALCOHOL AFFECTS THE CHANGING.
FEMALES: You ARE RESPONSIBLE FOR THE PAIN IN BOYS when you drink during the first three months !.
Johnnd
Thx in advance
Esays absence of any significant vascular flow to either testicle. What are he chances of having children or any type of sexual problems. Any recommendations. Wondering if i had taken him to the er if it would have made a difference.
sujest me .
At 6 months my sons doc told us we need to show him to an urologist as most likely he will have to be operated since he still had one Undescended testicle. At 7 months the urologist saw him and his right side testicle was not too far off from his scrotum, it was in the groin. The doctor confirmed that he needs to go through orchiopexy before he turns one. This is so that the testicle is not damaged and will not cause any fertility issues for him later in life. We were also very nervous but getting the orchiopexy done was the best decision for my son. We scheduled his procedure for when he was going to turn 9 months just so that he is a bit older.
I was super nervous but at the same time was anxious to get done with the procedure and move on. Then came the day of the procedure. The nurse had instructed that he can have formula only till 1am the night before and only clear liquids until 4:30am and then nothing until 7:30 which is when he was scheduled to go into OR. The night went ok. My son used to sleep through the night but that night I gave him 2oz at 1am And some water at 4am. We had to be there at 6:15 and so left the house at 5 am. I was very very nervous that my son just in a couple of hours will be struggling with pain. We were there in time. The nurse checked us in. The doctor came and spoke to us. My son was with us in this outpatient room. Then I changed him in his gown. And we waited in that room till it was time. Then the OR nurse came and we had to hand him off. This was the toughest moment of the whole procedure by far. We said bye and off he went. We waited in that room the whole while and he was brought back to us in the nurses arms trying to wake up at 9am. He seemed to be in pain as I took him in my arms. He was fighting for a few minutes just then the nurse gave him pain killer prescription by mouth. He continued to sleep and wake up uncomfortable. Went on for half hour and then he fell asleep for like half hour. Then when he woke up he was grouchy but not crying in pain. He then accepted some water in his favorite sippy. We checked out and put him in his car seat and left. He was fast asleep in the car. An hour later we reached home.
He was quite sleepy and slow the rest of the day had some more water. At around 3 pm had 2oz formula. I was alternating prescription pain med and ibuprofen every 3 hours. He had no problem falling asleep. So kept alternating little milk, sleep, some baby food fruit and the day ends. At night he slept well, we just woke him up for his meds.
Today I am glad we did it and it's over. He was back to himself wanting to crawl everywhere and jump the next day. He is still on Tylenol and Ibuprofen but every 8 hrs. His scrotum swelling reduced 50 percent and if someone dint know can't tell he has had a surgery 4 days back. All is well that ends well. No major issues with diapering as well just keep doing normal cleaning. Hope this helps.
I have a question regarding an orchiopexic surgery I had when I was young regarding a problem with testicular torsion. Everything turned out fine since it was caught in time. The problem I'm having and always had is that my testicle has always remained sensitive to touch compared to my other one. I'm 32 now and sexually active but I always makes sure my partner is super gentle with my boys, especially the one I had issues with going on 25 years ago now. Should I consider having it looked at again or should I just live with the sensitivity?
Thanks
nt to know will it affect my futute or sex life
My son had an undescented testical and went in to surgery at 1 1/2 yrd and then the doctors realize it was too high and was going to need a second stage we would have to come back months later to see if it survive. So months later we went back and it was still too short so he said it would drop as he grew his tendent would grow. His now 3 and its still not in its scrotum.. Is this bad??help!!!
i m 18+ year old and i haves examined by a urologist that i have both testicles undescended
can these are treated at this age?
And can i be able to reproduce ?
Please give me replies because i m too much worried
Any thoughts? Why does this happen?
please if you can help thanks doctors
am 25yes old i have a problem with my left testical if looks like there is fluid in it what should i do
I have done my orchidopexy operation when i was 12 year...now i am 26 year guy..i was having bilateral undescended testicle..doctors told me to remove my one testies...my semen analysis clearly shows that i am not able to produce sperms now(zero sperm count)...and chances to have tumor in my testies are also increasing...can you please help me...is there any medicine or medical treatment available??? is this infertility is permanent and can't be solved by treatment?
Belive in God never lost hope.
I was diagnosed with dual (both) testis undescended since of birth and performed a surgery when my age was 30 year.
My three doctors recommend me not to perform any surgery bcz your testis are no more active and should be removed.
I request to the doctor that plz do a surgery I believe in God wl help me.
After surgery doctor said me that you have zero hope and should adopt a baby.
After two year of surgery I performed a samen test which shows zero, TESE also shown zero sperm.
Taken tablets clomid for a three month again my report was zero.
I Never lost hope and after one year I performed a samen test which miracally shown two live and three dead spermetozooa with abnormal shape and morphology . Taken one month vitamin course now my samen is 5mil count with good shape and 50% morphology .
When I checked the report to my doctor he was very shocked and said to perform again it is really a miracale.
So don't give hope believe in God, good food, no tension wil give u every thing.
God can create us also can give us good health.
Doctor is not perfect in every thing.
Thanks
Im 29 years old and discovered this around when i was 18. My wrist has bumped into it a few times but i have been to shy about admitting this to anyone and getting a opinion from a doctor.
What risk can i face i live like this without telling.
Me and wife intend to hv more kids. Pls advise
I had an Orchiopexy around the age of 12. What are the chanves I will be infertile in the future.