Lumpectomy
Definition
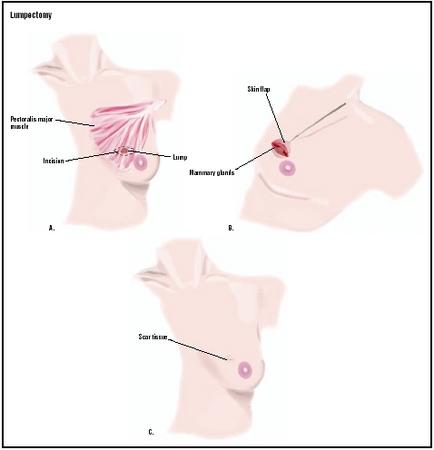
Lumpectomy is a type of surgery for breast cancer. It is considered "breast-conserving" surgery because only the malignant tumor and a surrounding margin of normal breast tissue are removed. Lymph nodes in the armpit (axilla) may also be removed. This procedure is also called lymph node dissection.
Purpose
Lumpectomy is a surgical treatment for newly diagnosed breast cancer. It is estimated that at least 50% of women with breast cancer are good candidates for this procedure. The location, size, and type of tumor are of primary importance when considering breast cancer surgery options. The size of the breast is another factor the surgeon considers when recommending surgery. The patient's psychological outlook, as well as her lifestyle and preferences, should also be taken into account when treatment decisions are being made.
The extent and severity of a cancer is evaluated, or "staged," according to a fairly complex system. Staging considers the size of the tumor and whether the cancer has spread (metastasized) to adjacent tissues, such as the chest wall, the lymph nodes, and/or to distant parts of the body. Women with early stage breast cancers are usually better candidates for lumpectomy. In most cases, a course of radiation therapy after surgery is part of the treatment. Chemotherapy or hormone treatment may also be prescribed.
In some instances, women with later stage breast cancer may be able to have lumpectomies. Chemotherapy may be administered before surgery to decrease tumor size and the chance of metastasis in selected cases.
Contraindications to lumpectomy
There are a number of factors that may prevent or prohibit a breast cancer patient from having a lumpectomy. The tumor itself may be too large or located in an area where it would be difficult to remove with good cosmetic results. Sometimes several areas of cancer are found in one breast, so the tumor cannot be removed as a single lump. A cancer that has already attached itself to nearby structures, such as the skin or the chest wall, needs more extensive surgery.
Certain medical or physical circumstances may also eliminate lumpectomy as a treatment option. Sometimes lumpectomy may be attempted, but the surgeon is unable to remove the tumor with a sufficient amount of surrounding normal tissue. This may be termed "persistently positive margins," or "lack of clear margins." Lumpectomy is suitable for women who have had previous lumpectomies and have a recurrence of breast cancer.
Because of the need for radiation therapy after lumpectomy, this surgery may be medically unacceptable. A breast cancer discovered during pregnancy is not amenable to lumpectomy because radiation therapy is part of the treatment. Radiation therapy cannot be administered to pregnant women because it may injure the fetus. If, however, delivery would be completed prior to the need for radiation, pregnant women may
The need for radiation therapy may also be a barrier due to nonmedical concerns. Some women simply fear this type of treatment and choose more extensive surgery so that radiation will not be required. The commitment of time, usually five days a week for six weeks, may not be acceptable for others. This may be due to financial, personal, or job-related constraints. Finally, in geographically isolated areas, a course of radiation therapy may require lengthy travel and perhaps unacceptable amounts of time away from family and other responsibilities.
Demographics
The American Cancer Society estimated that in 2003, 211,300 new cases of breast cancer would be diagnosed in the United States and 39,800 women would die as a result of the disease. Approximately one in eight women will develop breast cancer at some point in her life. The risk of developing breast cancer increases with age: women aged 30 to 40 have a one in 252 chance of developing breast cancer; women aged 40 to 50 have a one in 68 chance; women aged 50 to 60 have a one in 35 chance; and women aged 60 to 70 have a one in 27 chance—and these statistics do not even account for genetic and environmental factors.
In the 1990s, the incidence of breast cancer was higher among white women (113.1 cases per 100,000 women) than African-American women (100.3 per 100,000). The death rate associated with breast cancer, however, was higher among African American women (29.6 per 100,000) than white women (22.2 per 100,000). Rates were lower among Hispanic women (14.2 per 100,000), American Indian women (12.0), and Asian women (11.2 per 100,000).
Description
Any amount of tissue, from 1–50% of the breast, may be removed and called a lumpectomy. Breast conservation surgery is a frequently used synonym for lumpectomy. Partial mastectomy, quadrantectomy , segmental excision, wide excision, and tylectomy are other, less commonly used names for this procedure.
The surgery is usually done while the patient is under general anesthetic. Local anesthetic with additional sedation may be used for some patients. The tumor and surrounding margin of tissue is removed and sent to a pathologist for examination. The surgical site is then closed.
If axillary lymph nodes were not removed before, a second incision is made in the armpit. The fat pad that contains lymph nodes is removed from this area and is also sent to the pathologist for analysis. This portion of the procedure is called an axillary lymph node dissection; it is critical for determining the stage of the cancer. Typically, 10 to 15 nodes are removed, but the number may vary. Surgical drains may be left in place in either location to prevent fluid accumulation. The surgery may last from one to three hours.
Diagnosis/Preparation
Routine preoperative preparations, such as having nothing to eat or drink the night before surgery, are typically ordered for a lumpectomy. Information about expected outcomes and potential complications is also part of preparation for lumpectomy, as it is for any surgical procedure. It is especially important that women know about sensations they might experience after the operation, so the they are not misinterpreted as signs of further cancer or poor healing.
If the tumor is not able to be felt (not palpable), a pre-operative localization procedure is needed. A fine wire, or other device, is placed at the tumor site, using x ray or ultrasound for guidance. This is usually done in the radiology department of a hospital. The woman is most often sitting up and awake, although some sedation may be administered.
Aftercare
The patient may stay in the hospital one or two days, or return home the same day. This generally depends on the extent of the surgery, the medical condition of the patient, and physician and patient preferences. A woman usually goes home with a small bandage. The inner part of the surgical site usually has dissolvable stitches. The skin may be sutured or stitched; or the skin edges may be held together with steristrips, which are special thin, clear pieces of tape.
After a lumpectomy, patients are usually cautioned against lifting anything which weighs over five pounds for several days. Other activities may be restricted (especially if the axillary lymph nodes were removed) according to individual needs. Pain is often enough to limit inappropriate motion. Women are often instructed to wear a well-fitting support bra both day and night for approximately one week after surgery.
Pain is usually well controlled with prescribed medication. If it is not, the patient should contact the surgeon, as severe pain may be a sign of a complication, which needs medical attention. A return visit to the surgeon is normally scheduled approximately ten days to two weeks after the operation.
Radiation therapy is usually started as soon as possible after lumpectomy. Other additional treatments, such as chemotherapy or hormone therapy, may also be prescribed. The timing of these is specific to each individual patient.
Risks
The risks are similar to those associated with any surgical procedure. Risks include bleeding, infection, breast asymmetry, anesthesia reaction, or unexpected scarring. A lumpectomy may also cause loss of sensation in the breast. The size and shape of the breast will be affected by the operation. Fluid can accumulate in the area where tissue was removed, requiring drainage.
If lymph node dissection is performed, there are several potential complications. A woman may experience decreased feeling in the back of her armpit. She may also experience other sensations, including numbness, tingling, or increased skin sensitivity. An inflammation of the arm vein, called phlebitis, can occur. There may be injury to the nerves controlling arm motion.
There is a risk of developing lymphedema (swelling of the arm) after axillary lymph node dissection. This swelling can range from mild to very severe. It can be treated with elastic bandages and specialized physical therapy, but it is a chronic condition, requiring continuing care. Lymphedema can arise at any time, even years after surgery.
Normal results
When lumpectomy is performed, it is anticipated that it will be the definitive surgical treatment for breast cancer. Other forms of therapy, especially radiation, are often prescribed as part of the total treatment plan. The expected outcome is no recurrence of the breast cancer.
Morbidity and mortality rates
Approximately 2–10% of patients develop lymphedema after axillary lymph node dissection. Five percent of women are unhappy with the cosmetic effects of the surgery. The rate of cancer recurrence after five years is about 5–10%, and 10–15% after 10 years.
Alternatives
A procedure in which the entire affected breast is removed, called a mastectomy, has been shown to be equally effective in treating breast cancer as lumpectomy, in terms of rates of recurrence and survival. Some women may choose to have a mastectomy because they strongly fear a recurrence of breast cancer, and may consider a lumpectomy too risky. Others may feel uncomfortable with a breast that has had a cancer, and would experience more peace of mind with the entire breast removed.
A new technique that may eliminate the need for removing many axillary lymph nodes is being tested. Sentinel lymph node mapping and biopsy is based on the idea that the condition of the first lymph node in the network, which drains the affected area, can predict whether the cancer may have spread to the rest of the nodes. It is thought that if this first, or sentinel, node is cancer-free, then there is no need to look further. Many patients with early-stage breast cancers may be spared the risks and complications of axillary lymph node dissection as the use of this approach continues to increase.
Resources
books
Love, Susan M., with Karen Lindsey. Dr. Susan Love's Breast Book, 3rd ed. Cambridge: Perseus Publishing, 2000.
Robinson, Rebecca Y. and Jeanne A. Petrek. A Step-by-Step Guide to Dealing With Your Breast Cancer. New York: Carol Publishing Group, 1999.
periodicals
Apantaku, Leila. "Breast-Conserving Surgery for Breast Cancer." American Family Physician 66, no. 12 (December 15, 2002): 2271–8.
Dershaw, D. David. "Breast imaging and the conservative treatment of breast cancer." Radiologic Clinics of North America 40, no. 3 (May 2002): 501–16.
organization
American Cancer Society. 1599 Clifton Rd. NE, Atlanta, GA 30329-4251. (800) 227-2345. http://www.cancer.org .
National Cancer Institute (NCI) http://cancertrials.nci.nih.gov/types/breast/treatment/sentnode .
National Lymphedema Network. 2211 Post St., Suite 404, San Francisco, CA 94115-3427. (800) 541-3259 or (415) 921-1306. http://www.wenet.net/~lymphnet .
Ellen S. Weber, MSN
Stephanie Dionne Sherk
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Lumpectomy is usually performed by a general surgeon or surgical oncologist. Radiation therapy is administered by a radiation oncologist, and chemotherapy by a medical oncologist. The procedure is frequently done in a hospital setting (especially if lymph nodes are to be removed at the same time), but specialized out-patient facilities are sometimes preferred.
QUESTIONS TO ASK THE DOCTOR
- Why is a lumpectomy recommended?
- What method of anesthesia/pain relief will be used?
- Will radiation or chemotherapy be administered?
- Will a lymph node dissection be performed?
- Am I a candidate for sentinel node biopsy?
What does this mean?
im not sure how she can determine that certainty just by seeing it on an ultrasound screen, but i have to believe she knows what she is talking about and i have prepared myself for the worst news. i have 4 days before getting my results and terrified. i am 49. she told me that it is treatable and will need an operation (lumpectomy i think), sent me home and told me not to worry! (yeah right)that its ONLY 11mm. its 11mm i dont want inside my body thank you very much. one thing i would advise though, as much as you might not want to, tell your loved ones as soon as possible, cos you cant rely on there support if they dont know, and this waiting period is horrendous, and you DO need to talk.
Should I go for the lumpectomy as I risk killing a good piece of my breast tissues..
Pls help me understand better..
I had my lumpectomy 7 days ago,all went well.But Saw the surgeon yesterday and she wandered how long I have had the infection,my breast is sooo sore,swollen and red,I said I didn't know ,thought it was all apart of it..??She has put me on keflex for 10 days.Went for my walk tonight,and had to come home after half a block to painful even to walk.I have been told by others to put ice on to relieve the pain??Anyone know??
on Mon. unless things get worse.
This made the job of the 2nd surgeon more difficult to determine which lymph nodes corresponded to the ducts (?) to test for nodes that were non-cancerous. The 2nd surgery was very, very beneficial as he had the pathology dept test the tissue results before I was finished with my lumpectomy. I recently (approximately a month ago) had a battery of tests performed on me (mammograms, ultrasound, bone scans, MRI's on my brain as my "chemobrain" is just NOWo starting to improve and my breasts as i have been experiencing excrutiating pain in rt. breast (sometimes both), a bone scan (? I had so many tests it's hard to keep track) and ultimately I had a Pet/ct scan that detected abnormal activity in lymph node #18. My BC surgeon is looking into a needle biopsy done thru my ribs/chest area to diagnose the "abnormal activity" as reflected in the PET/CT ONLY & my oncologist said my bloodwork was normal.
If the dr is unable to perform a needle biopsy due to it's location either I wait 2-3 months & have another PET at that time to see if the "abnormal activity" is still detectable in node #18 OR attempt a risky, painful thoracic surgery to remove ??? from behind my chest wall.
What is the best option for long-term survivability as 3 months seems a LONG time to wait especially if it could be spreading to other lymph nodes. I want to live a long, healthy, meaningful life as I'm only 41 & have a lot of living to do.
Thank you for your attention & sorry so long.
Melissa Callans
Los Angelesl
However I had a lumpectomy 5 years ago, had lymph nodes removed they said as a precaution but there was no cancer in the nodes, I have lymphodema which is annoyingly painful I have been numb down my right side to my waist back and front and down to my elbow and my armpit since the operation, I have damaged breast tissue due to the radiotherapy and so far have had seven breast infections, I am now allergic to penicillin which is more than annoying so I have been suffering for five bloody years with pain to the point where I sometimes feel suicidal. My last two infections were October and the present time and quite frankly I have had enough and am now close to seeing my surgeon to tell him I want my breast removed immediately, no one has looked into why I keep getting infections in the breast and sometimes I have been told this pin is simply something I have to live with, no flaming wonder I have felt suicidal. pretty sick of all this. Hope no-one else suffers this way.
I sent my biopsy samples to Dr. Lagios back in 2001. He then studied them and agreed with Dr. Melvin Silverstein that my diagnosis should be LCIS, not DCIS or DCIS with invasion. However, since there was so much confusion surrounding my case, Dr. Lagios advised me to get an excisional biopsy in order to see more tissue and make certain the surrounding area was the same as the small amount of tissue he looked at in the needle biopsy samples. I did get the excisional biopsy done as a surgery. It was painless and healed very quickly without hardly a trace. Dr. Lagios verified the diagnosis of LCIS. I had no further treatment for ten years other than regular checkups every six months---once with my local OBGYN and another manual checkup from the surgeon who did my biopsy. This year I was diagnosed with invasive lobular cancer. It seems I was the one of 5-10% who got it with a diagnosis of LCIS. So in March I had a lumpectomy to my right breast and I'm now taking an aromatase inhibitor to block the estrogen and getting ready to receive radiation therapy. I refused chemo and later was tested with what is called an Oncotype DX test and discovered I did not need chemo even though my surgeon in Seattle, WA was pretty much threatening me to get it.
From my experience there is a great deal of over treatment and fear surrounding the big "C" word. I don't like to act in fear!!! I would prefer to glean all the knowledge I can and educate myself as well as pray and received my guidance from my Creator.
of brast cancer. My surgery for a Lumpectomy is Friday the
18th of January, very scare. What I wanted to be able to
thank you for your support.
IT IS MY RIGHT ARM AND I AM CONCERN AS TO WHAT AND WHAT I CANNOT DO FOR WHAT PERIOD
OF TIME.. I AM GOING TO START RADATION IN TWO WEEKS.
I did everything I could to avoid this. I was so careful so as not to get an infection that it really upsets me. I'm sure everything will be fine from here on in. Will see an oncologist soon and learn more about my radiation treatment. Trying very hard to be optimistic.
Kate ðŸ€
Up. I thought to myself that my questions have been answered, yet I never once mentioned the dreaded word CANCER,! Has anyone else been in a similar situation as myself. I would love to hear from you.
I had stage 1 ductal invasive carcinoma. had lumpectomy, and snlb. Have clear margins and clear node. cancer was 1.3 cm. I am 72 and active and healthy. I was taking HRT for 30 years until a surprise yeary mammo showed something. was core biopsied and found to be ER PR+, Her2neg. Since everything is out and all went well, I don't understand why I would have radiation and I don't want to take tamoxifen because of side effects or armidex which is recommended because I already have osteoporotic dangers. that was always my concern genetically. no cancer in family, but lots of osteoporosis. I feel like I don't want either radiation because I don't see for what and don't want these pills which will affect my quality of life with minimal positive effect based on probabilties for future. Confused. What did you decide to do? thanks
I was very surprised to find the worse part of this has been the balloon that was inserted. It wasn't particularly painful but was irritating. I am done with surgery and radiation now.
I wish you all the best, hearing you have cancer, even stage 0 is terrifying. Continue fighting.
I never wore a bra before my surgery, but have perservered this past week, have been told i have to wear one for 6 weeks night and day, whatcwill happen if i stop wearing it, or just wear it in the day, its not painful if i dont wear it, any advise will be very welcomed, I wish all you ladies coping with your cancer diagnosis and surgery all the best, we can overcome this, lets not let cancer beat us, xoxo