Bunionectomy
Definition
A bunionectomy is a surgical procedure to excise, or remove, a bunion. A bunion is an enlargement of the joint at the base of the big toe and is comprised of bone and soft tissue. It is usually a result of inflammation and irritation from poorly fitting (narrow and tight) shoes in
Purpose
A bunionectomy is performed when conservative means of addressing the problem, including properly fitting, wide-toed shoes, a padded cushion against the joint, orthotics, and anti-inflammatory medication, are unsuccessful. As the big toe moves sideways, it can push the second toe sideways as well. This can result in extreme deformity of the foot, and the patient may complain not only of significant pain, but of an inability to find shoes that fit.
Demographics
Bunion formation can be hereditary, which means that if the individual's mother or father had the condition, he or she is at an increased risk of developing one as well. Bunions can also be a result of a congenital deformity, which means that the individual was born with an anatomical condition that made the development of a bunion more likely. Women are nine to 10 times more likely to develop bunions than men. The American Orthopaedic Foot & Ankle Society reports a study estimating that about 88% of women wear shoes that are too small and that 55% have developed bunions. The condition may begin to form in adolescence. Other conditions that contribute to bunion formation include flat-footedness, a tight Achilles tendon, and rheumatoid arthritis. The earlier the diagnosis, the better the chance that significant deformity will be avoided.
Description
Bunions become more common later in life. One reason is that with age the foot spreads and proper alignment is not maintained. In addition, the constant friction of poorly fitting shoes against the big toe joint creates a greater problem over time. Ignoring the problem in its early stages leads to a shifting gait that further aggravates the situation.
Once surgery has been decided on, the extent of the procedure will depend on the degree of deformity that has taken place. There are several different surgical techniques, mostly named after the surgeons who developed them, such as McBride, Chevron, and Keller. The degree and angle of deformity as well as the patient's age and physical condition play a significant role in the surgeon's choice of technique, which will determine how much tissue is removed and whether or not bone repositioning will occur. If bone repositioning is done, that part of the surgery is referred to as an osteotomy ( osteo means bone). The type of anesthesia, whether ankle block (the most common, in which the foot is numb but the patient is awake), general, or spinal, will depend on the patient's condition and the anticipated extent of the surgery. For surgery done on an ambulatory basis, the patient will usually be asked to arrive one to two hours before the surgery and stay for about two to three hours after the procedure. The procedure itself may take about an hour.
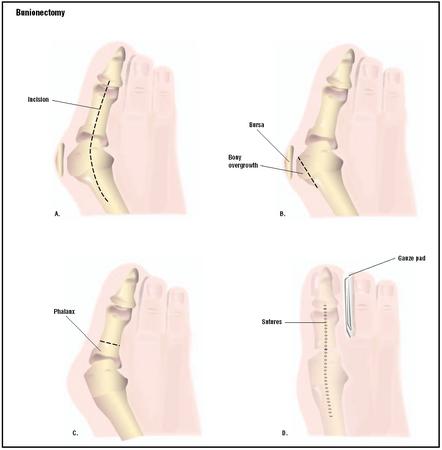
The surgeon will make an incision over the swollen area at the first joint of the big toe. The enlarged lump will be removed. The surgeon may need to reposition the alignment of the bones of the big toe. This may require more than one incision. The bone itself may need to be cut. If the joint surfaces have been damaged, the surgeon may hold the bones together with screws, wires, or metal plates. In severe cases, the entire joint may need to be removed and a joint replacement inserted. If pins were used to hold the bones in place during recovery, they will be removed a few weeks later. In some mild cases, it may be sufficient to repair the tendons and ligaments that are pulling the big toe out of alignment. When finished, the surgeon will close the incision with sutures and may apply steri-strips as an added reinforcement. A compression dressing will be wrapped around the surgical wound. This helps to keep the foot in alignment as well as help reduce postoperative swelling.
Diagnosis/Preparation
Intense pain at the first joint of the big toe is what most commonly brings the patient to the doctor. Loss of toe mobility may also have occurred. Severe deformity of the foot may also make it almost impossible for the patient to fit the affected foot into a shoe. The condition may be in either foot or in both. In addition, there may be a crackling sound in the joint when it moves. Diagnosis of a bunion is based on a physical examination , a detailed history of the patient's symptoms and their development over time, and x rays to determine the degree of deformity. Other foot disorders such as gout must be ruled out. The patient history should include factors that increase the pain, the patient's level of physical activity, occupation, amount of time spent on his or her feet, the type of shoe most frequently worn, other health conditions such as diabetes that can affect the body's ability to heal, a thorough medication history, including home remedies, and any allergies to food, medications, or environmental aspects. The physical exam should include an assessment while standing and walking to judge the degree to which stability and gait have been affected, as well as an assessment while seated or lying down to measure range of motion and anatomical integrity. An examination of the foot itself will check for the presence of unusual calluses, which indicate abnormal patterns of friction. Circulation in the affected foot will be noted by checking the skin color and temperature. A neurological assessment will also be conducted.
Conservative measures are usually the first line of treatment and target dealing with the acute phase of the condition, as well as attempting to stop the progression of the condition to a more serious form. Measures may include:
- rest and elevation of the affected foot
- eliminating any additional pressure on the tender area, perhaps by using soft slippers instead of shoes
- soaking the foot in warm water to improve blood flow
- use of anti-inflammatory oral medication
- an injection of a steroidal medication into the area surrounding the joint
- systematic use of an orthotic, either an over-the-counter product or one specifically molded to the foot
- the use of a cushioned padding against the joint when wearing a shoe
If these measures prove unsuccessful, or if the condition has worsened to significant foot deformity and altered gait, then a bunionectomy is considered. The doctor may use the term hallux valgus when referring to the bunion. Hallux means big toe and valgus means bent outward. In discussing the surgical option, it is important for the patient to clearly understand the degree of improvement that is realistic following surgery.
X rays to determine the exact angle of displacement of the big toe and potential involvement of the second toe will be taken. The angles of the two toes in relation to each other will be noted to determine the severity of the condition. Studies in both a standing as well as a seated or lying down position will be considered. These will guide the surgeon at the time of the surgery as well. In addition, blood tests, an EKG, and a chest x-ray will most likely be ordered to be sure that no other medical condition has gone undiagnosed that could affect the success of the surgery and the patient's recovery.
Aftercare
Recovery from a bunionectomy takes place both at the surgical center as well as in the patient's home. Immediate post-surgical care is provided in the surgical recovery area. The patient's foot will be monitored for bleeding and excessive swelling; some swelling is considered normal. The patient will need to stay for a few hours in the recovery area before being discharged. This allows time for the anesthesia to wear off. The patient will be monitored for nausea and vomiting, potential aftereffects of the anesthesia, and will be given something light to eat, such as crackers and juice or ginger ale, to see how the food is tolerated. Hospital policy usually requires that the patient have someone drive them home, as there is a safety concern after having undergone anesthesia. In addition, the patient will most likely be on pain medication that could cause drowsiness and impaired thinking.
It is important to contact the surgeon if any of the following occur after discharge from the surgical center:
- fever
- chills
- constant or increased pain at the surgical site
- redness and a warmth to the touch in the area around the dressing
- swelling in the calf above the operated foot
- the dressing has become wet and falls off
- the dressing is bloody
While the patient can expect to return to normal activities within six to eight weeks after the surgery, the foot is at increased risk for swelling for several months. When the patient can expect to bear weight on the operated foot will depend on the extent of the surgery. The milder the deformity, the less tissue is removed and the sooner the return to normal activity level. During the sixto-eight-week recovery period, a special shoe, boot, or cast may be worn to accommodate the surgical bandage and to help provide stability to the foot.
Risks
All surgical procedures involve some degree of risk. The most likely problems to occur in a bunionectomy are infection, pain, nerve damage to the operated foot, and the possibility that the bunion will recur. Sharing all pertinent past and present medical history with the surgical team helps to lower the chance of a complication. In addition to the risk of the surgery itself, anesthesia also has risks. It is important to share with the anesthesia team the list of all the vitamins, herbs, and supplements, over-the-counter medications, and prescription medications that the patient is taking.
Normal results
The expected result will depend on the degree of deformity that has occurred prior to surgery, the patient's medical condition and age, and the adherence to the recovery regimen prescribed. Some degree of swelling in the foot is normal for up to six months after the surgery. Once wound healing has taken place, the surgeon may recommend exercises or physical therapy to improve foot strength and range of motion. It is important to be realistic about the possible results before consenting to the surgery. Since over-pronation of the foot is not corrected with the surgery, orthotics to help keep the foot/feet in alignment are usually prescribed.
Morbidity and mortality rates
According to the American Orthopaedic Foot & Ankle Society, less than 10% of patients undergoing bunionectomy experience complications, and 85–90% of patients feel the surgery was successful.
Alternatives
It may be possible to avoid surgery by preventing bunion growth from worsening. Wearing shoes that are the right size and shape is a key factor. Try on new shoes in the afternoon when the foot is more tired and perhaps has some fluid buildup. Rather than going by size alone, make sure the shoe fits well, and that there is proper arch support. Additionally, there should be enough space in the toe box for the toes to wiggle around.
If diagnosed early, an injection of a steroidal anti-inflammatory medication around the joint may be enough to decrease the irritation in the area and allow the joint to recuperate. This, along with proper shoes, may halt progression of the condition. If there is no pain accompanying the bunion, surgery is not necessary. Some people find that a cream containing the same ingredient as found in chili peppers, capsaicin, applied locally to the joint can decrease the pain. However, once deformity and its accompanying severe pain has occurred, it is unlikely that surgery can be avoided.
Resources
books
Barker, L. Randol, John R. Burton, and Phillip D. Zieve, eds. Principles of Ambulatory Medicine. 5th edition. Baltimore: William & Wilkins, 1999.
Skinner, Harry B. Current Diagnosis & Treatment in Orthopedics. Appleton & Lange, 2000.
organizations
American Orthopaedic Foot & Ankle Society. 2517 Eastlake Avenue East, Seattle, WA 98102. http://www.aofas.org . American Podiatric Medical Association. http://www.apma.com .
Esther Csapo Rastegari, RN, BSN, EdM
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
Bunionectomies are performed by orthopedic surgeons, podiatric surgeons, and general surgeons. In selecting a surgeon, it is best to consider those who perform at least 20 bunionectomies each year. Most bunionectomies are performed as same-day, or ambulatory, surgery, in which the patient goes home the same day of the procedure. Sometimes a patient's condition may warrant staying overnight in the hospital.
QUESTIONS TO ASK THE DOCTOR
- How many bunionectomies do you perform each year?
- Are there any clinical trials for new medications or new types of procedures available?
- What complications have you seen with this procedure?
- What choices do I have for anesthesia?
- What can I expect during the recovery period?
- When can I return to my work and other regular activities?
- How soon after the surgery can I drive?
- How much improvement can I expect after surgery?
What will I receive for pain medication? How painfull is the surgery?
This occured beause I put weight on it too early. The Dr. was not clear that I needed to remain on crutches for four weeks. I am concerned that I will have to have the procedure again and that it will prolong my recovery and keep me from doing the second foot. Since the screw is loose, won't he have to tighten it anyway? Won't he have to take out the plate eventually?
I am really confused and daunted by all this. I just want to get this pver with so I can get the other foot done befor the school year starts in September ( a little more than a month away). ANy questions you can answer would be very helpful.
Tank goodness for family, friends and a great boss!
Five weeks on I can only put weight on it for ten miutes at a time as
becomes severe. I am still on painkillers every four hours.
I am due to see the surgeon on 5th July by which time I hope not to
be in pain. I am a very active person and find it very frustrating
to be limited to what I can do. Warning to all women 'Wear sensible shoes'
or suffer in later life. Fashion is not worth it.
Five weeks on I can only put weight on it for ten miutes at a time as
becomes severe. I am still on painkillers every four hours.
I am due to see the surgeon on 5th July by which time I hope not to
be in pain. I am a very active person and find it very frustrating
to be limited to what I can do. Warning to all women 'Wear sensible shoes'
or suffer in later life. Fashion is not worth it.
This new podiatrist (I moved out of state), will do the same type of surgery, but will put 3 screws in. This will keep me off my foot for only 4 wks. My bunions are hereditary. It's from your feet leaning inward as you walk. Orthopedic inserts are a must even after surgery.
Thanking you in advance.
I was able to put weight on my feet the day I came home from the surgery by using a walker and returned to work full time (office work with minimal to moderate walking)5 days after surgery.
The main problem I am having now is finding shoes that fit and that are comfortable. The doc inserted a screw in each big toe that will disintegrate in time making my big toes not very mobile right now. I also have a problem with flat feet which need arch support. I bought some expensive shoes recommended by someone who sells orthopoedic shoes, but after wearing them a few hours, they are just too confining across the top of my feet which causes this part of my feet to swell. Can anyone give me any ideas in the shoe area?
From what I have read, I am learning that these surgeries could take as long as 6 months to 1 year to recover so I am hoping that in another 3 months, my feet will be in better shape. I still have quite a bit of numbness in the surgical area. Also, my big toe on one foot has straightened out good, but the other is pulling back over. On my last post-op visit, my surgeon just told me to wear my splints for 2 more weeks, which made me wear them a total of 7 weeks, but that didn't make a difference to the one toe.
With all of the said and done, I still would recommend having this surgery done in both feet at the same time, if needed and if you have someone you can really count on to help you 24 hours a day for the first week.
probably be the deciding day. I do not want to go through all of this, surgery and a long
recovery, and have the condition reappear within a few years again. I wish I could get
information from patients who have had the surgery and are now 5 years out, and see if
they think the whole "nightmare" was really worth the pain and suffering of surgery.
Procedures and recovery times have come a long way!!! I only use 1 pain pill. Ready for summer shoes and sandals. PS i'm 54, this was a peice of cake. OK the first 3 weeks of limited activity was not fun. I love to keep in shape. Now I have to work DDBL time to get my tone back. Worthit though!
If you do have the surgery, be sure to stay continuously medicated - esp when going from hospital to home. Don't let the pain meds wear off. If you have a good doctor, your pain can be minimal to none, but FYI, the bunionectomy is a surgery they test new pain meds on. I had no pain and am thankful!
Do your homework on the doctor - if you have a big correction, don't pick someone who says they'll have you on your feet ASAP. I was horizontal for 2 weeks (except to get up to eat or go to the restroom) and non-weight bearing for 12 weeks. My doctor said that walking on it too soon is a big reason that bunions will return.
What is the likelihood that the caste will allow the bone to heal at this point in time? How long does it take for the slowest healer to develop evidence of a callus or healing of the bones? What are my options if there is no evidence of healing TEN WEEKS after surgery?
Thanks for your response/feedback!
most appreciative.
Mario
bottom of the foot under the big toe. My biggest complaint is that when I stand up my foot turns red and when I take a shower, it turns dark red or purple up to my ankle.I still use a shower chair. The color goes back to normal when I elevate the foot. Is this normal? It has me concerned. If it is normal how long before it goes back to normal? I am supposed to get the other foot done, but after this I am not sure I want to.
In my case...no pain yet. So far so good
went back to work too soon, could have stayed out longer than 4 weeks - when foot elevated at work desk it wasn't the best ergonomically with knee bent etc caused swelling, pain & discomfort in knee too; did PT for 2x3 which helped then started walking & eventually joined gym in late August 2011 & was doing bike, walking & 1-2 laps jogging & felt great;
Had R bunionectomy on Dec 8th- have had more help from family & friends & able to keep foot elevated in more compliant way - pain different than L foot post surgery & foot more bruised which doesn't show till about 1wk to 10 days post op, bruising from toes to ankle area with tenderness. Toes throb & still pain in foot after 4 weeks, but feel the foot will be fine this is just normal healing process. Good surgeon is important & don't be afraid to ask questions, doctors are human too not God. I will be out of work longer for R foot, it is so very important for the bones to heal correctly these are your feet which thru all this I have learnt HOW so important feet are! to walk, have balance etc & do not want to mess that up in any way- I am very glad & thankful I did both feet & I am looking foreward to no pain in both feet now for walking, running & enjoying my life pain free!!! great experience, just do your homework & follow peace in your heart/gutt before doing procedure & have peace with the right doctor - ask questions of the doctor till you are satisfied & have peace in their ability too... best wishes to all who decide on future bunionectomy's! ;-)
Post surgery ,I had Xray and morphine post op which I didn't have last time. I 've noticed that I had 2 pins when the stiches were removed .I guess my Ortho was concerned but said it looks fine .I'm in 11th week recovering doing my physio with no pain.Color is good but the front of my L big toe feels a bit numb and if I rub more, a bit tingly.I hope and pray that feeling will go away and be back to normal .Good luck to all who has bunions ,if it's not bad like pain don't have it remove just wear wide shoes .But it's great to wear
regular shoes with no pain after surgery.
My pod mentioned that I may need a mortens extension to my orthotics to ease the pain on the big toe joint. Guess I need patience, it is getting less painful as I use my foot more.
T MACK
i am a little stressed because a am a 15 year old girl and a few years back when i hurded my foot the hospital took x rays and it showed that my big toe is busy growing skew somedays it hurts and other days it doesn't but my mom said the docter said that day they can only fix it when i am 18 and i dont understand it.
The aftermath of surgery is pain! I could not tolerate any pain medication and roughed it out with ibuprofen and ice.
I had to stay completely off of the foot for 6 weeks. I wore a boot, ace bandage and bandage.
I highly recommend a wheel chair.
The pain and swelling lasted up to the 5th week, but the pain came back as soon as I was able to walk on the foot with a
boot.
The pain in my foot now that I am walking in the boot is excruciating. It shoots up to me hip. My foot sometimes swells to my knee.
And toe spasms, I've had way too many with pain sending me to the moon.
No one is the same, but this is a very painful surgery.
I have to walk in the boot for a month. I'm hoping pain will be over by then.
I hope you have better luck than me with the pain pills
I could not put any weight on my foot the first week and I kept it elevated no shower either. Today, first day of week #2 I had physical therapy and they say everything looks good. Pain is minimal don't need pain meds. I can walk on my heel and light weight bearing with crutches. Keeping foot elevated. Only allowed on my feet 20 minutes of an hour for the next few weeks. I also have a scooter that helps alot to get around. Do not suggest watching any little ones after this surgery. They move too quickly and you will be slow.
By the way, I followed the post-op instructions and PT exercises to the T.
My doctor and physiotherapist encouraged as much weight bearing as possible and to keep moving my ankle and wiggling my toe. After the first week I didn't have to elevate unless I felt pain, or thought it was swelling from walking with the crutches.
At my two week post-op appointment I had the remaining stitches removed and the wound cleaned and re-dressed. The nurse seemed pleased with my recovery at that point.
By week four I was walking around indoors with no crutch and only using one crutch when going out and by week five I found crutches more of a hindrance than a help and have been walking around with no issues for two weeks now.
Tomorrow I'll have my x-ray to ensure the bone has set correctly and I'll speak to a physio about strengthening the muscles I've been neglecting these past weeks.
I found the recovery difficult enough for the first two weeks, especially because I was worried about re-opening the wound. But if this means a winter without getting aches in my bunion from the cold, it will have not been in vain! Best of luck to anyone considering the surgery. It's manageable and beneficial.
I appreciate all the comments from people years after the first type of bunionecomies saying they still have pain.
THe lapidus sounds like a safer long-term procedure to me, but I'm clueless. I know the recovery time is longer, but if it's better long-term, I'd prefer it.
My doc said I have a choice, and that usually young people (i.e. in their 20s) do the lapidus bunionectomy, even though the recovery time is longer. Thanks for any insight, particularly from people who had the surgery several years ago.
Have been using coconut oil on the raised scar now that the stitches have come off. Also immersing foot in hot water with Epson salts every other night and then rubbing coconut oil all over the foot. Will be trying some essential oils this week (lavender and eucalyptus) this week for pain and slightly scarring. I can walk around the house at the moment but have to take regular breaks, put my foot up and ice it.
There is something I am very worried about and was wondering if anyone out there would be able to shed some light. My big toe is still 'floating' and not touching the floor at all. I have searched the internet but can't come up with anything. Was just wondering if this is the result of a botched job as the swelling is going down but the toe remains in the same position. Would be grateful for any assistance. Many thanks. Olivia
I had my big toe fused 4 weeks ago now. I had to use crutches and lie down for the first 2 weeks before I could put more weight on my foot from using the medical shoe (heel walking that is).
But it makes a difference to just walk around the house every so often without the crutches. I had some kind of pain the first few days but after that I didnt have any pain most likely just numbness all around and sometimes like a stingy feeling on the top of my toe?
Not pain but most likely annoying but you get used to it. I hope to get x rays done this week on my 4th week (fingers crossed).
Colin-