Bladder augmentation
Definition
Bladder augmentation, also known as augmentation cystoplasty, is reconstructive surgery to increase the reservoir capacity of the bladder. The procedure is very common and involves tissue grafts (anastomosis) from a section of the small intestine (ileum), stomach, or other substitutes that are attached to the urinary bladder by sewing or stapling. Whether due to chronic obstructive bladder damage, birth defects that resulted in small reservoir capacity, or dysfunction due to nerve innervation of the bladder muscle (sphincter), surgery is chosen only after a thorough medical work-up that involves assessment of the lower urinary tract, functional physiological evaluation, and anatomic assessment. Some laparoscopic methods (surgery with a fiber-optic instrument inserted through the abdomen) of bladder augmentation have been tried, but reports indicate that these are technically arduous and may not have the long-lasting effects of open surgery.
Purpose
Bladder dysfunction and incontinence may be due to problems with the reservoir capacity of the bladder or with the "gatekeeping" muscle (the sphincter), which, instructed by the brain, allows urine to build up or to be released. Bladder augmentation is used to treat serious and irreversible forms of incontinence and to protect the upper urinary tract (kidney function) from reflexia (urine back up to the kidneys). Many candidates for the surgery are highly compromised individuals with other serious conditions like spinal cord injuries and multiple sclerosis, as well as patients likely to undergo kidney transplantation . Patients who undergo bladder augmentation must be free of bowel and urethral disease and be able to perform self-catheterization (able to place a urinary tube into their urethra).
Description
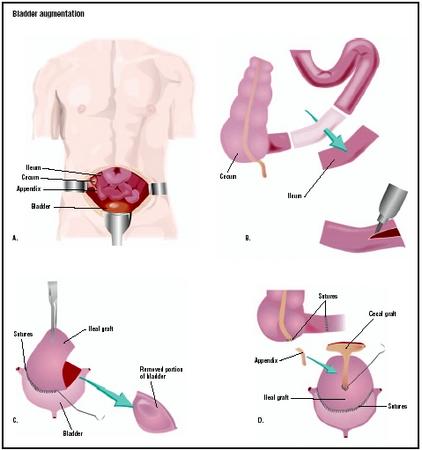
Standard augmentation involves segments of the bowel used to create a pouch or wider wall for the bladder in order to enhance its reservoir capacity. Often this reconstruction surgery is accompanied by procedures that tighten the neck of the bladder, as well. Milkulicz performed the first clinical augmentation cystoplasty using abdominal tissue in 1898. Couvelaire, in the 1950s, popularized bladder augmentation for the treatment of the contracted bladder due to tuberculosis. Until the 1970s it was thought that those with bladder dysfunction could be treated with bladder diversion, and that this procedure offered a simple and safe means of emptying the bladder. However, it was soon discovered that pressure from the bladder caused irreparable damage to the kidneys, with 50% of patients exhibiting such deterioration. The new diagnostic assessment of the bladder as well as the need for a new medical intervention for patients with severe bladder dysfunction opened the way for urinary tract reconstruction. Today, many techniques are available, along with new types of grafting substitutions.
The basic procedure involves open abdominal surgery with resection of a 10–20 in (25–30-cm) segment of ileum, cecum (first part of the large intestine), or the ileocecum (the junction of small and large intestines) cut down the middle (detubularized), and shaped into a U-configuration with a pouch at the bottom. This opening or pouch will be the "patch" for the bladder. During surgery, the bladder itself is also opened at the dome and cut at right angles to
Diagnosis/Preparation
Patients selected for bladder augmentation are chosen after they undergo a thorough physical exam, x-ray tests, and bladder physiology tests, as well as a renal and bladder ultrasound for any dilation of the kidneys or ureters or kidney obstruction. A VCUG (holding and voiding urine) test is performed to assess the contour of the bladder and to assess for ureteral reflux (back up of urine to the kidneys). Finally, a CMG (cystometrogram) is performed in the physician's office to judge the pressure and volume levels at which the urine leakage occurs. Once the tests, as well as the history and physical exam are completed, treatment plans commence.
The patient should plan for up to two weeks in the hospital. The patient will have been on a low-residue diet for a few days before admission. Surgery will take place two to three days after hospital admittance. In the hospital, a general examination will be performed and blood taken. The bowel will need to be cleaned in preparation. Clear fluids will be given, as well as a strong laxative prior to surgery.
Aftercare
Early complications of surgery include cardiovascular, thrombo-embolic (blood clot), gastrointestinal, and respiratory complications associated with major abdominal surgery. Many patients require three months after surgery to allow their augmented bladder to establish itself. This involves a special diet for a few months as well as patient familiarity with the fact that the augmented bladder empties after the native bladder. Two weeks after surgery tests are performed to ensure that the patch is leak proof. Once a watertight reservoir is demonstrated, the catheters and drains that were introduced for surgery are removed.
Risks
Long term risks of the procedure include peptic ulceration of the bladder and perforation of the gastric segment. Spontaneous perforation is rare but it is life threatening and has a 25% mortality rate. Other risks include bacterial infections, metabolic changes, urinary tract infections, and urinary tract stones. Nocturnal incontinence is sometimes a problem after the surgery.
Normal results
Although some patients recover spontaneous voiding function, this does not occur with reliable predictability. Preoperatively, patients should be prepared for the likelihood that they will have to perform lifelong intermittent catherization and irrigation of the augmented bladder. Other effects are a special diet for up to three months and pain after surgery.
Morbidity and mortality rates
Reported surgical risks include 3–5.7% rate of adhesive small bowel obstruction requiring operative intervention, 5–6% incidence of wound infection, 0–3% reoperation rate for bleeding. Long term complications include a 50% unchanged bladder compliance and renal deterioration. No reduction in growth in children has been reported, but the procedure is not recommended for children who have not reached puberty, unless there is the threat of kidney damage.
Alternatives
Bladder augmentation is a medical treatment of last resort for those patients unable to avoid incontinence through medical alternatives. Other surgeries may be indicated if the individual is not a candidate for self-catherization or has other medical or psychological conditions that would rule out bladder augmentation.
Resources
books
Dewan, P., and M. E. Mitchell, eds. Bladder Augmentation. Oxford Press, 2000.
periodicals
Abrams, P., S.K. Lowry, et al. "Assessment and Treatment of Urinary Incontinence." Lancet 355 (June 2000): 2153–58
Fantl, J. A., D. K. Newman, J. Colling, et al. "Urinary Incontinence in Adults: Acute and Chronic Management. Clinical Practice Guideline, Number 2, 1996." Agency for Health Policy and Research Publications (March 1996).
Greenwell, T. J., S. N. Venn, and A. R. Mundy. "Augmentation Cystoplasty." British Journal of Urology International 88, no. 6 (October 2001): 511–534.
Qucek, M. I., and D. A. Ginsberg. "Long-term Urodynamics Follow-up of Bladder Augmentation for Neurogenic Bladder." Urology 169 (January 2003): 195–198.
Rackley, R. R., and J. B. Abdelmalak. "Radical Prostatectomy: Laparoscopic Augmentation Cystoplasty." Urological Clinics of America 28 (August 2001).
organizations
National Association for Continence. P.O. Box 8310 Spartanburg, SC 29305. (800) BLADDER, (252-3337). http://www.nafc.org .
National Kidney and Urologic Diseases Information Clearing-house. 3 Information Way, Bethesda, MD 20892-3580. (301) 654-4415. http://www.niddk.nih.gov .
The Simon Foundation for Continence. P.O. Box 835 Wilmette, IL 60091. (800) 23SIMON (237-4666). http://www.simonfoundation.org .
other
"Bladder Augmentation." Dr. Rajhttp. [cited April 2003]. http://www.drrajmd.com/treatments/treatments.htm .
Carr, Michael, and M. E. Mitchell. "Bladder Augmentation." Digital Urological Journal. [cited April 2003]. http://www.duj.com/Article/Carr/Carr.html .
"Neurogenic Bladder." [cited April 2003]. http://www.med.wayne.edu/urology/DISEASES/neurogenicbladder.html .
Nancy McKenzie, Ph.D.
WHO PERFORMS THE PROCEDURE AND WHERE IS IT PERFORMED?
A urological surgeon who is an MD with advanced training in urology and special surgical training for this type of surgery. Surgery takes place in a general hospital.
QUESTIONS TO ASK THE DOCTOR
- How many bladder augmentation surgeries do you perform a year?
- What complications of this surgery do you think are the most likely and/or worrisome?
- Are there other patients with my underlying medical conditions who have had this surgery that I could contact?
- Is there a pre-op patient group with this hospital that could help me understand my rehabilitation and help with the compliance with the diet and self-catherization?
if u send me more details(comprehensive)
thanks
i had a clam bladder type operation. at surgery bladder was found tb unusealy small so a bigger strip of bowel was used.i have self catheriesd ever since, full glories control iam only now having problems with insertion of catheter now talkis of supra pubic device.ialso now have spinal damage with server ballance and mobility problems it has beem worth it to strees free control over my bladder.
If I don't have this bladder surgery my kidneys will be damaged, I am scared to death I am going to die, is there anyone out thre that can help me that has had this surgery, is it life threatning,, painful, will I need a caheria 24 hours aday,what is recovery like.. please somone help,, I ned to raise my young son I don't want to die..thanks for your help...Lou
Thanks
Chuck
CAN I ASK ABOUT THE SECREATIONS FROM THE AUGMENTATION PART (ILEUM), FOR HOW LONG IT REMAINS(LIFE LONG??)
The first time it worked but i was still running to to loo very often i have had to s.i.c since the op. I had it repeated over a week ago & am worse off now than i have ever been (back to square one)I am now being considered for the bladder augmentation & have been told i will have to go to England to have it performed. The thought of this scares me. Does any one or Dr know if it can be done here in Belfast? Your help is much appreciated. Any other info would gladly be also welcomed.
Thanks in advance
Using drugs like ditropan with intermittent catheterization can be an alternative to augmentation, but does not work for everyone. Obviously, the risk is kidney damage if the bladder pressure is high, so you need good diagnostics. Constipation and UTIs makes things worse, so make sure you are on top of that.
thanks
the truth how bad is it. I have interstituial cystitis, and my bladder is shrinking, it only holds
2-4 onces with severe pain, they tell me the surgery might not help the pain . just help me hold more,
if it holds over 4 oz now it is like passing kidney stones ever day over and over. and it bleeds at time.
and I usually go pee about 30-50 times in 24 hours. does anybody else have anything simmilar to this.
I also have a bad back, shoulders, well my body is shot, with constant pain. I am real nervious about this
surgery, I did real well with 3 back surgeries, shoulder surgery, and knee surgery. but my belly is differant.
moves more and softer than my back. seeking answers Thanks Robin
ago, and was told around about 11years ago that I had a diseased bladder, and only an augmentation would help, well for one
thing I was never told that I would have to use a catheter, or have a blocked urethra from the mucus which is the part of the intestine they use to make a larger bladder, and produce's this mucus, now every second week I'm on antibiotic's, and now they don't work any more, and the Urologist that did the procedure has retired, and the one I see now, tells me there's
only an infection, but the pain is so bad I feel like screaming, and live on pain killers, so sorry I had the operation, that's for sure!!!
I just need to rule this out . Thank you
Im still needing to urinate on low volumes and voiding also, is this common at this stage post the surgery?
Your views would be appreciated
I am a 34 years old female, currently paralyzed as a result of a spinal cord decompression fourteen years ago. T4-6. After using the Foley catheter for so long I began getting ongoing uti's which then saw my regular physician referring me to an Urologist.
Recently he performed an urodynamics test which showed that my bladder is merely operating like a tunnel rather than a reservoir like it should. If I remove the catheter urine just flows. Further test showed that I now have bacteriruia, which he said will not get any better if the catheter remains. Even though I have in the catheter now, by body has begun rejecting it. Intermittent catheterization was also suggested as the recommended way of emptying the bladder in the future. so of course i would need the mitrofanoff to do this.
I am really concern about this surgery because after reading numerous reviews in forums, many persons suffer long term effects. It is really difficult when you are told that there is only one solution to your problem. It has me feeling like i am backed into a wall. my other concern is the price. i live in the Caribbean and have to travel to the US to get this done. So lord forbids if anything goes wrong when I return to my country after the surgery.
I'm going to have one soon .!
Kind Regards
Desray
Waheeda
I have leaking every night just wish i didnt